Potrebbero piacerti anche
- Theselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsDocumento10 pagineTheselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsFaizan MazharNessuna valutazione finora
- USPI - Med Guide - Feldene - Piroxicam - CapsulesDocumento15 pagineUSPI - Med Guide - Feldene - Piroxicam - CapsulesDini FarhatunnabilahNessuna valutazione finora
- Anaesthesia and EpilepsyDocumento10 pagineAnaesthesia and EpilepsyrYanDYNessuna valutazione finora
- Onsult: Ementia Reatment PdateDocumento5 pagineOnsult: Ementia Reatment PdateAxel Robinson HerreraNessuna valutazione finora
- Pharmaceuticals: Therapeutic Drug Monitoring of The Newer Anti-Epilepsy MedicationsDocumento27 paginePharmaceuticals: Therapeutic Drug Monitoring of The Newer Anti-Epilepsy MedicationsjayswalrameshNessuna valutazione finora
- Levetiracetam A Review of Its Use in The TreatmentDocumento7 pagineLevetiracetam A Review of Its Use in The TreatmentMuhammad Arif Budi PrakosoNessuna valutazione finora
- Antiepileptic Drug Interactions - Principles and Clinical ImplicationsDocumento14 pagineAntiepileptic Drug Interactions - Principles and Clinical ImplicationsErkan KirkNessuna valutazione finora
- Meyer 2010Documento24 pagineMeyer 2010deltanueveNessuna valutazione finora
- Oral Adverse Drug Reactions To Cardiovascular DrugsDocumento19 pagineOral Adverse Drug Reactions To Cardiovascular DrugsSuci RahmiNessuna valutazione finora
- Importance of Pharmacogenomics in The Personalized MedicineDocumento6 pagineImportance of Pharmacogenomics in The Personalized MedicineJames AustinNessuna valutazione finora
- Reversibledementias: Milta O. LittleDocumento26 pagineReversibledementias: Milta O. LittleLUCAS IGNACIO SANCHEZNessuna valutazione finora
- Clin Pharmacy ADRDocumento24 pagineClin Pharmacy ADRAnonymous DgPsK0oQNessuna valutazione finora
- Clin Pharmacy ADRDocumento36 pagineClin Pharmacy ADRAnonymous DgPsK0oQNessuna valutazione finora
- 2principles of Geriatric Pharmacotherapy - Lee - 10-19-10Documento53 pagine2principles of Geriatric Pharmacotherapy - Lee - 10-19-10Mbel'z Mbel'z Embil'zNessuna valutazione finora
- Anti-Epileptic Drugs - A Guide For The Non-NeurologistDocumento5 pagineAnti-Epileptic Drugs - A Guide For The Non-NeurologistArgentin2Nessuna valutazione finora
- Advarse Drug ReactionDocumento9 pagineAdvarse Drug ReactionAyanNessuna valutazione finora
- Hepatotoxicity Related To Anti-Tuberculosis Drugs: Mechanisms and ManagementDocumento13 pagineHepatotoxicity Related To Anti-Tuberculosis Drugs: Mechanisms and ManagementkhacthuanprovipNessuna valutazione finora
- Therapeutic Drug Monitoring: An Overview of Commonly Monitored DrugsDocumento7 pagineTherapeutic Drug Monitoring: An Overview of Commonly Monitored DrugsSerley WulandariNessuna valutazione finora
- Review Article: Pharmacogenomics of Drug Response in Type 2 Diabetes: Toward The Definition of Tailored Therapies?Documento11 pagineReview Article: Pharmacogenomics of Drug Response in Type 2 Diabetes: Toward The Definition of Tailored Therapies?James CowellNessuna valutazione finora
- Drug Induced LiverDocumento8 pagineDrug Induced LiverDita IndahNessuna valutazione finora
- Articles:: Q&A: Q&A: Dear SIRSDocumento5 pagineArticles:: Q&A: Q&A: Dear SIRSLucy WijayaNessuna valutazione finora
- Jurnal MetilphenidateDocumento61 pagineJurnal MetilphenidateRegina EnggelineNessuna valutazione finora
- PropofolDocumento9 paginePropofolarturschander3614Nessuna valutazione finora
- 2008 - Antituberculosis Drug-Induced Hepatotoxicity Concise Up-To-Date ReviewDocumento12 pagine2008 - Antituberculosis Drug-Induced Hepatotoxicity Concise Up-To-Date ReviewCarlos LuqueNessuna valutazione finora
- Pharmacogenetics and The Concept of Individualized Medicine: BS ShastryDocumento6 paginePharmacogenetics and The Concept of Individualized Medicine: BS Shastrykunalprabhu148Nessuna valutazione finora
- RRLDocumento30 pagineRRLbealinniNessuna valutazione finora
- Acetaminophen-Induced Hepatotoxicity PDFDocumento12 pagineAcetaminophen-Induced Hepatotoxicity PDFFranklin AvilaNessuna valutazione finora
- Dosage Form For Personalized Medicine: HistoryDocumento11 pagineDosage Form For Personalized Medicine: HistoryNayeema KhowserNessuna valutazione finora
- Antiepilepsy Drugs: Pharmacodynamics and Principles of Drug SelectionDocumento22 pagineAntiepilepsy Drugs: Pharmacodynamics and Principles of Drug SelectionNaela RizqiNessuna valutazione finora
- Voican Et Al 2014 Antidepressant Induced Liver Injury A Review For CliniciansDocumento12 pagineVoican Et Al 2014 Antidepressant Induced Liver Injury A Review For Cliniciansxiaonguyen02Nessuna valutazione finora
- Pharmacogenetics of Cardiovascular Drug TherapyDocumento11 paginePharmacogenetics of Cardiovascular Drug Therapybalaji5563Nessuna valutazione finora
- Drug-Induced Acute Liver FailureDocumento12 pagineDrug-Induced Acute Liver FailurePamela WheelockNessuna valutazione finora
- Summary of Product Characteristics: PosologyDocumento9 pagineSummary of Product Characteristics: Posologyddandan_2Nessuna valutazione finora
- Adr and ManagementDocumento48 pagineAdr and ManagementDhanush G V DhanushNessuna valutazione finora
- Case StudiesDocumento5 pagineCase Studiespragna novaNessuna valutazione finora
- Rheumatoid Arthritis: Progressive Autoimmune ConditionDocumento40 pagineRheumatoid Arthritis: Progressive Autoimmune Conditionhussein alnasryNessuna valutazione finora
- Amlodipine-10mg TabletDocumento7 pagineAmlodipine-10mg TabletMd. Abdur RahmanNessuna valutazione finora
- Adderall (CII) : NDA 11-522/S-040Documento15 pagineAdderall (CII) : NDA 11-522/S-040Marlboro LightsNessuna valutazione finora
- Levetiracetam EpilepsiaDocumento6 pagineLevetiracetam EpilepsiaAndresPimentelAlvarezNessuna valutazione finora
- Gupisone 2Documento9 pagineGupisone 2ahibba.03862Nessuna valutazione finora
- Nteraksi Obat Dalam Praktek Edokteran Igi: Drg. Yayun Siti Rochmah SPBMDocumento29 pagineNteraksi Obat Dalam Praktek Edokteran Igi: Drg. Yayun Siti Rochmah SPBMtristiarinaNessuna valutazione finora
- Mycophenolate Therapy of SLE Membranous Nephropathy: D N. S, Y T, B H. R, T N, G N, T E. P, and L A. HDocumento5 pagineMycophenolate Therapy of SLE Membranous Nephropathy: D N. S, Y T, B H. R, T N, G N, T E. P, and L A. HdhineyNessuna valutazione finora
- Artritis ReumatoideaDocumento13 pagineArtritis Reumatoideaglau_lo8525Nessuna valutazione finora
- Review: Hepatocellular Damage From Non-Steroidal Anti-Inflammatory DrugsDocumento5 pagineReview: Hepatocellular Damage From Non-Steroidal Anti-Inflammatory Drugsshessy-jolycia-kerrora-3047Nessuna valutazione finora
- Therapeutic Drug Monitoring of Antiepileptic Medications: Matthew D. KrasowskiDocumento27 pagineTherapeutic Drug Monitoring of Antiepileptic Medications: Matthew D. Krasowskikannan6461Nessuna valutazione finora
- Section 9 Anti Parkinsonism MedicinesDocumento14 pagineSection 9 Anti Parkinsonism MedicinesAmra ahmedNessuna valutazione finora
- 95 101 Hepatotoxicity of Paracetamol and Related FatalitiesDocumento7 pagine95 101 Hepatotoxicity of Paracetamol and Related Fatalitiesfabrizzio asdasdNessuna valutazione finora
- Antiepileptic Drugs and Liver Disease: Syed Nizamuddin Ahmed, Zaeem A. SiddiqiDocumento9 pagineAntiepileptic Drugs and Liver Disease: Syed Nizamuddin Ahmed, Zaeem A. SiddiqikurniawanNessuna valutazione finora
- AbriefguidetoadrsDocumento5 pagineAbriefguidetoadrsSri HariNessuna valutazione finora
- Drug Induced Hepatitis With Anti-Tubercular Chemotherapy: Challenges and Difficulties in TreatmentDocumento5 pagineDrug Induced Hepatitis With Anti-Tubercular Chemotherapy: Challenges and Difficulties in Treatmentmufqifitra160491Nessuna valutazione finora
- AAFP Diabetes MedicationsDocumento7 pagineAAFP Diabetes MedicationsThaysa LimaNessuna valutazione finora
- Pharmacokinetic-Pharmacodynamic Crisis in The Elderly: Ehab S. Eldesoky, MD, PHDDocumento11 paginePharmacokinetic-Pharmacodynamic Crisis in The Elderly: Ehab S. Eldesoky, MD, PHDMonica LucaciuNessuna valutazione finora
- Drug-Induced Hepatotoxicity: BackgroundDocumento13 pagineDrug-Induced Hepatotoxicity: BackgroundrianiNessuna valutazione finora
- Rebound Phenomenon - Important and Ubiquitous inDocumento5 pagineRebound Phenomenon - Important and Ubiquitous inCITRA AYU APRILIANessuna valutazione finora
- Common Adverse Effects of Antiretroviral Therapy For HIV DiseaseDocumento9 pagineCommon Adverse Effects of Antiretroviral Therapy For HIV DiseaseJonathan FoerNessuna valutazione finora
- Antiepileptic Drug Therapy in The Elderly - A Clinical Pharmacological ReviewDocumento11 pagineAntiepileptic Drug Therapy in The Elderly - A Clinical Pharmacological ReviewSandra QuinonesNessuna valutazione finora
- Drug Interaction of Dental DrugsDocumento14 pagineDrug Interaction of Dental DrugsAnubhuti SabhlokNessuna valutazione finora
- Drug Interaction Profesi New (PRT)Documento72 pagineDrug Interaction Profesi New (PRT)auliaNessuna valutazione finora
- Triple WhammyDocumento3 pagineTriple WhammyKhairul IzzatNessuna valutazione finora
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDa EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesValutazione: 4 su 5 stelle4/5 (2)
- Pharmacokinetics and Dose Selection of A Novel, Long-Acting Transdermal Fentanyl Solution in Healthy Laboratory BeaglesDocumento6 paginePharmacokinetics and Dose Selection of A Novel, Long-Acting Transdermal Fentanyl Solution in Healthy Laboratory BeaglesRhanna AbreuNessuna valutazione finora
- CV UpdatedDocumento6 pagineCV Updatedapi-535481376Nessuna valutazione finora
- 10 Rights in Drug AdministrationDocumento25 pagine10 Rights in Drug AdministrationNathaniel PulidoNessuna valutazione finora
- (Minoxidil Topical Solution USP) : Prescribing InformationDocumento2 pagine(Minoxidil Topical Solution USP) : Prescribing InformationHamid Ila InarrudNessuna valutazione finora
- OspeCon VademecumDocumento30 pagineOspeCon VademecumpatriciacarlasariNessuna valutazione finora
- NLN Medication Exam Study Guide QuizletDocumento36 pagineNLN Medication Exam Study Guide Quizletmaniz442Nessuna valutazione finora
- Tyramine: Drug Class: Indirectly Acting Sympathomimetic (A Byproduct of Tyrosine Metabolism) Mechanism of ActionDocumento2 pagineTyramine: Drug Class: Indirectly Acting Sympathomimetic (A Byproduct of Tyrosine Metabolism) Mechanism of ActionZobayer AhmedNessuna valutazione finora
- ClarithromycinDocumento3 pagineClarithromycinapi-3797941Nessuna valutazione finora
- Receptor Pharmacology Cheat Sheet (4f6203b546fa5)Documento5 pagineReceptor Pharmacology Cheat Sheet (4f6203b546fa5)sinthreckNessuna valutazione finora
- Bisacodyl (Dulcolax)Documento1 paginaBisacodyl (Dulcolax)ENessuna valutazione finora
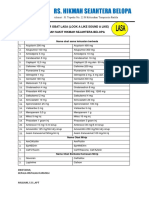
- Daftar Obat LasaDocumento3 pagineDaftar Obat LasaKhadijah MunawarNessuna valutazione finora
- Master Barang - CONTOH DidikDocumento2.803 pagineMaster Barang - CONTOH DidikVaniaNessuna valutazione finora
- Medications For FibromyalgiaDocumento3 pagineMedications For FibromyalgiaAl ClarkeNessuna valutazione finora
- So Apotek Jan 2021Documento104 pagineSo Apotek Jan 2021arin yuliaNessuna valutazione finora
- AlprazolamDocumento2 pagineAlprazolamGLen CaniedoNessuna valutazione finora
- HARGA Apotek Al LatifDocumento12 pagineHARGA Apotek Al LatifMarogi Al AnsorianiNessuna valutazione finora
- Formulation of Metformin HCL Floating Tablet Using HPC, HPMC K100M, and The CombinationsDocumento4 pagineFormulation of Metformin HCL Floating Tablet Using HPC, HPMC K100M, and The CombinationsPradnya Nagh KerenzNessuna valutazione finora
- Respiratory Drugs Midterm ExamDocumento10 pagineRespiratory Drugs Midterm ExamKevin VillaranteNessuna valutazione finora
- Pharmaceutical Jurisprudence MCQ PDF DownloadDocumento5 paginePharmaceutical Jurisprudence MCQ PDF DownloadDev TyagiNessuna valutazione finora
- Setup Rak ObatDocumento161 pagineSetup Rak Obatmuna barajaNessuna valutazione finora
- Pharmacist's Knowledge, Practice and Attitudes Toward Pharmacovigilance and Adverse Drug Reactions Reporting ProcessDocumento7 paginePharmacist's Knowledge, Practice and Attitudes Toward Pharmacovigilance and Adverse Drug Reactions Reporting ProcessAnnafiatu zakiahNessuna valutazione finora
- Opioid AllergyDocumento4 pagineOpioid AllergyJay100% (1)
- AnalgesicDocumento42 pagineAnalgesicVinayak SinghNessuna valutazione finora
- DDS ReviewDocumento30 pagineDDS ReviewIvymae TrillesNessuna valutazione finora
- 5 Adrenoceptor BlockersDocumento52 pagine5 Adrenoceptor BlockersHamid Hussain HamidNessuna valutazione finora
- 111 BBBDocumento99 pagine111 BBBjoelrequenaNessuna valutazione finora
- TTDexDocumento2 pagineTTDexSparKY NIghtcoreNessuna valutazione finora
- Laxative Guidelines Nov 2013Documento2 pagineLaxative Guidelines Nov 2013Purim KTshipNessuna valutazione finora
- STOKDocumento60 pagineSTOKanisaeka panNessuna valutazione finora
- Daftar Obat ApotekDocumento4 pagineDaftar Obat ApotekSriNessuna valutazione finora