Potrebbero piacerti anche
- Highlights On Globin Gene Switch: New Target For TherapeuticsDocumento33 pagineHighlights On Globin Gene Switch: New Target For TherapeuticsVijay RamananNessuna valutazione finora
- Thalassaemia 2016 - Lets Clear The DoubtsDocumento37 pagineThalassaemia 2016 - Lets Clear The DoubtsVijay RamananNessuna valutazione finora
- Bone Marrow Transplant in Thalassemia Major AnalysisDocumento4 pagineBone Marrow Transplant in Thalassemia Major AnalysisVijay RamananNessuna valutazione finora
- Bone Marrow Transplant Patient - Education - Booklet2Documento51 pagineBone Marrow Transplant Patient - Education - Booklet2Vijay RamananNessuna valutazione finora
- Donor Search Request Form For UNRELATED BONE MARROW DONOR SEARCHDocumento1 paginaDonor Search Request Form For UNRELATED BONE MARROW DONOR SEARCHVijay RamananNessuna valutazione finora
- Management of Acute Myeloid Leukaemia in Resource Constrained Setting and Elderly Patients!Documento5 pagineManagement of Acute Myeloid Leukaemia in Resource Constrained Setting and Elderly Patients!Vijay RamananNessuna valutazione finora
- Side Effect of Thalidomide and HydroxyureaDocumento2 pagineSide Effect of Thalidomide and HydroxyureaVijay RamananNessuna valutazione finora
- Autologous Transplant For Type I DMDocumento10 pagineAutologous Transplant For Type I DMVijay RamananNessuna valutazione finora
- Autoimmune Lymphoproliferative DisorderDocumento7 pagineAutoimmune Lymphoproliferative DisorderVijay RamananNessuna valutazione finora
- Allogenic and Autologus Stem Cell Transplants Per YearDocumento2 pagineAllogenic and Autologus Stem Cell Transplants Per YearVijay RamananNessuna valutazione finora
- Aplastic Anemia Bone Marrow Transplant AnalysisDocumento8 pagineAplastic Anemia Bone Marrow Transplant AnalysisVijay RamananNessuna valutazione finora
- Cord Blood Transplant AnalysisDocumento1 paginaCord Blood Transplant AnalysisVijay RamananNessuna valutazione finora
- Hemophilia ManagementDocumento11 pagineHemophilia ManagementVijay RamananNessuna valutazione finora
- Donor Search Request Form For UNRELATED BONE MARROW DONOR SEARCHDocumento1 paginaDonor Search Request Form For UNRELATED BONE MARROW DONOR SEARCHVijay RamananNessuna valutazione finora
- CML Pocket Guide For PatientsDocumento2 pagineCML Pocket Guide For PatientsVijay RamananNessuna valutazione finora
- Clinical experience with fetal hemoglobin induction therapy in patients with β-thalassemiaDocumento15 pagineClinical experience with fetal hemoglobin induction therapy in patients with β-thalassemiaVijay RamananNessuna valutazione finora
- WHO Dengue Guidelines 2013Documento160 pagineWHO Dengue Guidelines 2013Jason MirasolNessuna valutazione finora
- Treatment of MDSDocumento8 pagineTreatment of MDSVijay RamananNessuna valutazione finora
- Pre Bypass Blood Component ManagementDocumento3 paginePre Bypass Blood Component ManagementVijay RamananNessuna valutazione finora
- Algorithm For Post Coronary BypassDocumento3 pagineAlgorithm For Post Coronary BypassVijay RamananNessuna valutazione finora
- Use of Hydroxyurea With Wheatgrass in Thalassaemia MajorDocumento4 pagineUse of Hydroxyurea With Wheatgrass in Thalassaemia MajorVijay Ramanan100% (1)
- Ruby Hall Clinic BMT DepartmentDocumento1 paginaRuby Hall Clinic BMT DepartmentVijay RamananNessuna valutazione finora
- Study Recipes For Diabetes ReversalDocumento4 pagineStudy Recipes For Diabetes ReversalVijay RamananNessuna valutazione finora
- Ruby Hall Clinic BMTDocumento6 pagineRuby Hall Clinic BMTVijay RamananNessuna valutazione finora
- Thalassaemia Corporate Presentation For HelpDocumento10 pagineThalassaemia Corporate Presentation For HelpVijay RamananNessuna valutazione finora
- International Survey of Transplant For Sickle Cell DiseaseDocumento1 paginaInternational Survey of Transplant For Sickle Cell DiseaseVijay RamananNessuna valutazione finora
- Chemo-Interaction in HIVDocumento43 pagineChemo-Interaction in HIVVijay RamananNessuna valutazione finora
- Diabetes Type II and Be ReversedDocumento4 pagineDiabetes Type II and Be ReversedVijay RamananNessuna valutazione finora
- The Intestinal Microbiota Modulates The Anticancer Immune Effects of CyclophosphamideDocumento7 pagineThe Intestinal Microbiota Modulates The Anticancer Immune Effects of CyclophosphamideDaniel MarshallNessuna valutazione finora
- Thalassaemia Ideal TreatmentDocumento11 pagineThalassaemia Ideal TreatmentVijay RamananNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Pathophysiology Examination AnswersDocumento205 paginePathophysiology Examination AnswersFırat Güllü67% (6)
- Hubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan Warga Kebonsari Surabaya Di Masa Pandemi Covid-19Documento6 pagineHubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan Warga Kebonsari Surabaya Di Masa Pandemi Covid-19SavaNessuna valutazione finora
- Lista DiagnosticeDocumento566 pagineLista DiagnosticeGeanina MireaNessuna valutazione finora
- Leishmaniasis Pharmacology AsstDocumento7 pagineLeishmaniasis Pharmacology AsstHailat GNessuna valutazione finora
- Acute GastroenteritisDocumento48 pagineAcute Gastroenteritisansam kamalNessuna valutazione finora
- HIVSTI EpidemiologyDocumento61 pagineHIVSTI EpidemiologyZuriel San PedroNessuna valutazione finora
- Blood Products & Plasma SubstitutesDocumento15 pagineBlood Products & Plasma Substitutesahmadslayman1Nessuna valutazione finora
- Accomplishment Report (Individual)Documento9 pagineAccomplishment Report (Individual)Virliane Faith QuimsingNessuna valutazione finora
- Cepheid GeneXpert System Menu Flyer CE IVD 0293 EnglishDocumento2 pagineCepheid GeneXpert System Menu Flyer CE IVD 0293 EnglishTchouala DentrishNessuna valutazione finora
- BB Lab MidtermDocumento3 pagineBB Lab MidtermYo Issei HyodonoNessuna valutazione finora
- Pamphlet AmoebiasisDocumento3 paginePamphlet AmoebiasisAristotel Cabais100% (1)
- Revision For BioDocumento7 pagineRevision For BioJustt MeeNessuna valutazione finora
- Partial Record of Inventory Form of Vaccinated PaxDocumento18 paginePartial Record of Inventory Form of Vaccinated PaxDilg Asturias-CebuNessuna valutazione finora
- Algoritma Fever, DLLDocumento4 pagineAlgoritma Fever, DLLVanDoctor JerseyNessuna valutazione finora
- Difference Between Plasma and SerumDocumento4 pagineDifference Between Plasma and SerumQuraishi SahbNessuna valutazione finora
- Project in Mapeh (Health)Documento8 pagineProject in Mapeh (Health)guache warrinNessuna valutazione finora
- Unit 3 P Biotechnology 6th Semester Carewell PharmaDocumento20 pagineUnit 3 P Biotechnology 6th Semester Carewell PharmaSAHIL NABINessuna valutazione finora
- Prevention and Control of Diseases and DisordersDocumento45 paginePrevention and Control of Diseases and DisordersBhel San Pedro MarzanNessuna valutazione finora
- Rapid Test CovidDocumento2 pagineRapid Test CovidYuzia Birthdie C UNessuna valutazione finora
- Fastidious Gram Negative RodsDocumento74 pagineFastidious Gram Negative RodsMaria ClaraNessuna valutazione finora
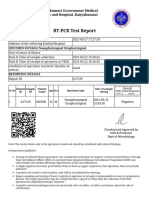
- RT-PCR Test Report: Kanyakumari Government Medical College and Hospital, KanyakumariDocumento2 pagineRT-PCR Test Report: Kanyakumari Government Medical College and Hospital, KanyakumariAnithaNessuna valutazione finora
- Guide to Understanding Autoimmune UveitisDocumento5 pagineGuide to Understanding Autoimmune UveitisHitesh ParmarNessuna valutazione finora
- Treatment and Prevention of Enteric (Typhoid and Paratyphoid) Fever - UpToDate 2020Documento17 pagineTreatment and Prevention of Enteric (Typhoid and Paratyphoid) Fever - UpToDate 2020Zubair Mahmood KamalNessuna valutazione finora
- Nicolle2008 PDFDocumento12 pagineNicolle2008 PDFRizki Noor AmeliaNessuna valutazione finora
- Origin, Transmission, Diagnosis and Management of Coronavirus Disease 2019 (COVID-19)Documento6 pagineOrigin, Transmission, Diagnosis and Management of Coronavirus Disease 2019 (COVID-19)Alfitrah NurjayaNessuna valutazione finora
- The Effect of Inflammation On BoneDocumento14 pagineThe Effect of Inflammation On BoneKelas CNessuna valutazione finora
- Microbiology Burton's Chapter 16Documento74 pagineMicrobiology Burton's Chapter 16Whenzhie Villaverde PampoNessuna valutazione finora
- Poststreptococcal Glomerulonephritis - UpToDateDocumento21 paginePoststreptococcal Glomerulonephritis - UpToDateHandre Putra100% (1)
- Ebook - Understanding Immune Cell Function in Cancer - IsoPlexisDocumento7 pagineEbook - Understanding Immune Cell Function in Cancer - IsoPlexisJ VelazcoNessuna valutazione finora
- Necrotizing Fasciitis: David Hough MSIII Penn State College of MedicineDocumento33 pagineNecrotizing Fasciitis: David Hough MSIII Penn State College of Medicineaaz220Nessuna valutazione finora