Potrebbero piacerti anche
- Pharmacologist: Passbooks Study GuideDa EverandPharmacologist: Passbooks Study GuideNessuna valutazione finora
- Lange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesDocumento2 pagineLange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesSolNessuna valutazione finora
- Introduction to commonly used antibioticsDocumento2 pagineIntroduction to commonly used antibioticsAmir AmirulNessuna valutazione finora
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Documento48 pagineNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanNessuna valutazione finora
- Clinical Medication ListDocumento181 pagineClinical Medication Listsophia onu100% (2)
- Congenital Heart DefectsDocumento1 paginaCongenital Heart DefectsBeck33ers5826Nessuna valutazione finora
- Sample Personal Statement For Pulmonary Critical Care FellowshipDocumento1 paginaSample Personal Statement For Pulmonary Critical Care FellowshipnutoNessuna valutazione finora
- Sri Lankan Biology Olympiad 2011Documento7 pagineSri Lankan Biology Olympiad 2011Science Olympiad Blog100% (1)
- Pediatrics Clerkship Shelf ReviewDocumento78 paginePediatrics Clerkship Shelf Reviewlcaskidsn12s100% (1)
- Vancomycin ReviewDocumento26 pagineVancomycin Reviewkhangsiean89Nessuna valutazione finora
- Care of Clients With Problems Related To Neurological SystemDocumento44 pagineCare of Clients With Problems Related To Neurological Systemapi-3735995100% (1)
- Pharmacy Law & Ethics Regulations StandardsDocumento62 paginePharmacy Law & Ethics Regulations Standardsaberhaneth1163Nessuna valutazione finora
- Critical Heart Disease in Infants and Children PDFDocumento997 pagineCritical Heart Disease in Infants and Children PDFBeck33ers5826Nessuna valutazione finora
- Chapter 73: Drug Therapy of Rheumatoid Arthritis Test Bank: Multiple ChoiceDocumento4 pagineChapter 73: Drug Therapy of Rheumatoid Arthritis Test Bank: Multiple ChoiceNurse Utopia100% (1)
- 001 Introduction To PharmacologyDocumento29 pagine001 Introduction To Pharmacologynancy alsharuNessuna valutazione finora
- 8 B. Social, Behavioral, Economic, and Administrative SciencesDocumento140 pagine8 B. Social, Behavioral, Economic, and Administrative SciencesSamson SeiduNessuna valutazione finora
- Practical Medical MicrobiologyDocumento12 paginePractical Medical MicrobiologyAli RazaNessuna valutazione finora
- Pharm Chapter 2 and 3 Study GuideDocumento10 paginePharm Chapter 2 and 3 Study GuideamkNessuna valutazione finora
- Vancomycin: Group 5 R.M 2Documento31 pagineVancomycin: Group 5 R.M 2vi_wiviaNessuna valutazione finora
- 2-Principles of Antimicrobial Therapy 2 PDFDocumento29 pagine2-Principles of Antimicrobial Therapy 2 PDFShashidharan MenonNessuna valutazione finora
- 201060antibiotics and ChildrenDocumento2 pagine201060antibiotics and ChildrencillenujmwNessuna valutazione finora
- Immunization GuideDocumento26 pagineImmunization GuideRob CrosbyNessuna valutazione finora
- MCQ 1-7Documento9 pagineMCQ 1-7جعغر آل حيدرNessuna valutazione finora
- QuestionsDocumento13 pagineQuestionsMikee MeladNessuna valutazione finora
- Pathology MCQ - Infectious Disease PDFDocumento5 paginePathology MCQ - Infectious Disease PDFsilas mosha100% (2)
- OTC TableDocumento64 pagineOTC TableHenry SpencerNessuna valutazione finora
- ProeukaryoticADMModule - Grade12 - Quarter1STEM - BIO12-Ia-c-3 (1) Lyka Mae B. BenitoDocumento27 pagineProeukaryoticADMModule - Grade12 - Quarter1STEM - BIO12-Ia-c-3 (1) Lyka Mae B. BenitoLyka Mae Benito75% (4)
- PAA CellCultureMediaDocumento20 paginePAA CellCultureMediaNilabh Ranjan100% (1)
- Natasha Campbell McBride - Food AllergyDocumento11 pagineNatasha Campbell McBride - Food AllergyChalida HayulaniNessuna valutazione finora
- NURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYDa EverandNURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYNessuna valutazione finora
- Life and DeathDocumento23 pagineLife and DeathJea Joel MendozaNessuna valutazione finora
- Alligation Practice Problems AnswersDocumento5 pagineAlligation Practice Problems AnswersNash C. UsopNessuna valutazione finora
- Class Medication MOA Side Effects: Intranasal SteroidsDocumento2 pagineClass Medication MOA Side Effects: Intranasal SteroidsChron MedNessuna valutazione finora
- 6.3 Defence Against Infectious DiseaseDocumento43 pagine6.3 Defence Against Infectious DiseaseAlacrity Xenoion SpadesNessuna valutazione finora
- Pedia Stickers PDFDocumento8 paginePedia Stickers PDFAshNessuna valutazione finora
- Using Consumer Medicine Information (CMI)Documento15 pagineUsing Consumer Medicine Information (CMI)Joseph OchoaNessuna valutazione finora
- Meglitinide Works by Stimulating The Release of Insulin in The Presence of GlucoseDocumento53 pagineMeglitinide Works by Stimulating The Release of Insulin in The Presence of GlucoseWil LesterNessuna valutazione finora
- ADULT CRITICAL CARE SEDATION GUIDELINESDocumento12 pagineADULT CRITICAL CARE SEDATION GUIDELINESBeatriz Maria Espinosa HernandezNessuna valutazione finora
- Alcohol and Drug QuizDocumento6 pagineAlcohol and Drug Quizapi-285898641Nessuna valutazione finora
- Dr. Dewi-Geriatric PharmacologyDocumento41 pagineDr. Dewi-Geriatric PharmacologyAnne Gustriwati0% (1)
- Look Under Drugs Affecting Nutritional and Metbolic FunctionDocumento1 paginaLook Under Drugs Affecting Nutritional and Metbolic FunctionChrissieNessuna valutazione finora
- Antibiotics 101Documento49 pagineAntibiotics 101Tony VoNessuna valutazione finora
- Patho Unit 5Documento37 paginePatho Unit 5Shafiya ShaikNessuna valutazione finora
- M. Pharm Review NAPLEX07Documento1 paginaM. Pharm Review NAPLEX07JUSASBNessuna valutazione finora
- Drugs Used in TuberculosisDocumento27 pagineDrugs Used in Tuberculosisapi-3705123Nessuna valutazione finora
- Pharmacology of The GITDocumento31 paginePharmacology of The GITmarviecute22Nessuna valutazione finora
- Guidebook MathematicsDocumento67 pagineGuidebook MathematicsJohn HamiltonNessuna valutazione finora
- Infective Endocarditis: Akriti DahalDocumento79 pagineInfective Endocarditis: Akriti DahalAkriti100% (1)
- Quinolones, Folic Acid Antagonist and Urinary Tract Antitb and LeprosyDocumento124 pagineQuinolones, Folic Acid Antagonist and Urinary Tract Antitb and LeprosyrenNessuna valutazione finora
- Clinical trial peer review and drug information resourcesDocumento2 pagineClinical trial peer review and drug information resourcesagent2catNessuna valutazione finora
- Residencymanual 2015 2016 PDFDocumento53 pagineResidencymanual 2015 2016 PDFcelecosibNessuna valutazione finora
- OSCE - Sample Chapter PDFDocumento32 pagineOSCE - Sample Chapter PDFAndrés LLanos PrietoNessuna valutazione finora
- Piperacillin-Tazobactam AntibioticDocumento9 paginePiperacillin-Tazobactam Antibiotic배기숭Nessuna valutazione finora
- IV PO Conversion CAPDocumento3 pagineIV PO Conversion CAPdamondouglasNessuna valutazione finora
- Therapeutic Drug MonitoringDocumento10 pagineTherapeutic Drug MonitoringAnnie SethiNessuna valutazione finora
- Drug Assessment Paper: InstructionsDocumento6 pagineDrug Assessment Paper: InstructionsRAZEN PARAS0% (1)
- APHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDocumento13 pagineAPHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDrSamia El WakilNessuna valutazione finora
- Anti Neoplastic and Immunosupressant DrugsDocumento29 pagineAnti Neoplastic and Immunosupressant DrugsAshraf Moby100% (1)
- Guideline Antibiotic RationalDocumento35 pagineGuideline Antibiotic RationalIstianah EsNessuna valutazione finora
- ANTIBIOTICS Pharmacology NursingDocumento10 pagineANTIBIOTICS Pharmacology NursingRalph Alfonse De JesusNessuna valutazione finora
- Pharmacy Practice Lec1Documento18 paginePharmacy Practice Lec1كسلان اكتب اسميNessuna valutazione finora
- Flashcards for Admin ConsiderationsDocumento1 paginaFlashcards for Admin ConsiderationsAntonette Joy SolinapNessuna valutazione finora
- Chapter 55 - Drugs Acting On The Lower Respiratory TractDocumento13 pagineChapter 55 - Drugs Acting On The Lower Respiratory TractJonathonNessuna valutazione finora
- Pharmacology QuestionsDocumento10 paginePharmacology QuestionsEthel Gretchen CasallaNessuna valutazione finora
- Anxiety Disorders Treatment OptionsDocumento5 pagineAnxiety Disorders Treatment OptionsJohn HolmesNessuna valutazione finora
- Drugs of ChoiceDocumento3 pagineDrugs of ChoiceReeti R. Bhat100% (1)
- Inhaled InsulinDocumento17 pagineInhaled InsulinH.k. VamshidharNessuna valutazione finora
- NURSING CARE OF ADULTS II: Passbooks Study GuideDa EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNessuna valutazione finora
- Subclavian Artery BranchesDocumento1 paginaSubclavian Artery BranchesBeck33ers5826Nessuna valutazione finora
- Pharyngeal Arches 1Documento1 paginaPharyngeal Arches 1Beck33ers5826Nessuna valutazione finora
- Abdominal Arteries ChartDocumento1 paginaAbdominal Arteries ChartBeck33ers5826Nessuna valutazione finora
- CN 10 VagusDocumento1 paginaCN 10 VagusBeck33ers5826Nessuna valutazione finora
- Emc Campus Mapp 2012 VerticalDocumento1 paginaEmc Campus Mapp 2012 VerticalBeck33ers5826Nessuna valutazione finora
- CN 5 V2 Maxillary NerveDocumento1 paginaCN 5 V2 Maxillary NerveBeck33ers5826Nessuna valutazione finora
- Neck Sympathetic ChainDocumento1 paginaNeck Sympathetic ChainBeck33ers5826Nessuna valutazione finora
- CN 11 and CN 12Documento1 paginaCN 11 and CN 12Beck33ers5826Nessuna valutazione finora
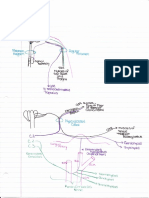
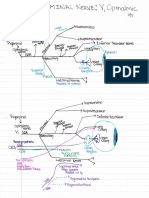
- CN 5 V1 Opthalmic NerveDocumento1 paginaCN 5 V1 Opthalmic NerveBeck33ers5826Nessuna valutazione finora
- Pulmonary Journal ClubDocumento19 paginePulmonary Journal ClubBeck33ers5826Nessuna valutazione finora
- Block 11 Resident Education 2020Documento1 paginaBlock 11 Resident Education 2020Beck33ers5826Nessuna valutazione finora
- EKG TemplateDocumento3 pagineEKG TemplateBeck33ers5826Nessuna valutazione finora
- Renal Drug EffectsDocumento1 paginaRenal Drug EffectsBeck33ers5826Nessuna valutazione finora
- First Floor Options for Bucknell at Mews at Laurel CreekDocumento1 paginaFirst Floor Options for Bucknell at Mews at Laurel CreekBeck33ers5826Nessuna valutazione finora
- EKG Page 1Documento1 paginaEKG Page 1Beck33ers5826Nessuna valutazione finora
- Upload 1Documento1 paginaUpload 1Beck33ers5826Nessuna valutazione finora
- EKG EtcDocumento1 paginaEKG EtcBeck33ers5826Nessuna valutazione finora
- Diabetic Foot Ulcer Classification System ExplainedDocumento2 pagineDiabetic Foot Ulcer Classification System ExplainedBeck33ers5826Nessuna valutazione finora
- EkgsDocumento3 pagineEkgsBeck33ers5826Nessuna valutazione finora
- Asthma ClassificationDocumento1 paginaAsthma ClassificationYak NafarNessuna valutazione finora
- Diabetic Foot Ulcer Classification System ExplainedDocumento2 pagineDiabetic Foot Ulcer Classification System ExplainedBeck33ers5826Nessuna valutazione finora
- Post Op ComplicationsDocumento1 paginaPost Op ComplicationsBeck33ers5826Nessuna valutazione finora
- Renal Drug Ion Actions Cells Response 1Documento1 paginaRenal Drug Ion Actions Cells Response 1Beck33ers5826Nessuna valutazione finora
- Acid-Base Disorders Worksheet GuideDocumento1 paginaAcid-Base Disorders Worksheet GuideBeck33ers5826100% (1)
- Emma Holliday LecturesDocumento1 paginaEmma Holliday LecturesBeck33ers5826Nessuna valutazione finora
- Try AgainDocumento1 paginaTry AgainBeck33ers5826Nessuna valutazione finora
- Document 1Documento1 paginaDocument 1Beck33ers5826Nessuna valutazione finora
- SOIL EXPLORARION ReportDocumento8 pagineSOIL EXPLORARION ReportCampto GamingNessuna valutazione finora
- Topik: Pengenalan Perosak Tanaman Dan Kepentingannya Dalam PertanianDocumento230 pagineTopik: Pengenalan Perosak Tanaman Dan Kepentingannya Dalam PertanianHazimHashimNessuna valutazione finora
- Research Proposal CapsuleDocumento12 pagineResearch Proposal CapsuleClaire GonoNessuna valutazione finora
- Bacterial Reverse Mutation TestDocumento12 pagineBacterial Reverse Mutation TestOtilia TeixeiraNessuna valutazione finora
- Literature Review - Packaging Storage and Shelf Life AnalysisDocumento24 pagineLiterature Review - Packaging Storage and Shelf Life AnalysisDeepak BhanjiNessuna valutazione finora
- WATER TREATMENT TECHNOLOGY (TAS 3010) LECTURE NOTES 2 - Environmental MicrobiologyDocumento30 pagineWATER TREATMENT TECHNOLOGY (TAS 3010) LECTURE NOTES 2 - Environmental Microbiologymamat88100% (2)
- Probiotics For Cancer Alternative Prevention and TreatmentDocumento10 pagineProbiotics For Cancer Alternative Prevention and TreatmentRafael OesterreichNessuna valutazione finora
- ANTIBACTERIAL POTENTIALDocumento7 pagineANTIBACTERIAL POTENTIALPratiwi IshakNessuna valutazione finora
- 6 Antibiotic AbbreviationsDocumento2 pagine6 Antibiotic AbbreviationsDeladem EmmanuelNessuna valutazione finora
- Disease Detectives Cheat SheetDocumento2 pagineDisease Detectives Cheat SheetBereket LakiNessuna valutazione finora
- 1-Basics of MicrobiologyDocumento53 pagine1-Basics of MicrobiologyKiran ShresthaNessuna valutazione finora
- Oxoid RapID Systems 171209Documento4 pagineOxoid RapID Systems 171209mohdkhairNessuna valutazione finora
- Benefits of genetically altered bacteria in agricultureDocumento7 pagineBenefits of genetically altered bacteria in agriculturefadhilah rasyadNessuna valutazione finora
- A Model To Study The Effect of Boiling On Water Borne Bacterial Diarrheal AgentsDocumento6 pagineA Model To Study The Effect of Boiling On Water Borne Bacterial Diarrheal AgentsjamonlineNessuna valutazione finora
- WS2 - Engelmann DemonstrationDocumento3 pagineWS2 - Engelmann DemonstrationTsang Ka ChunNessuna valutazione finora
- Well Rehabilitation 2Documento23 pagineWell Rehabilitation 2شايد همين امروزNessuna valutazione finora
- Bio 108: Introductory Biology and Microbiology Course Outline SynopsisDocumento5 pagineBio 108: Introductory Biology and Microbiology Course Outline SynopsisKiEl GlorkNessuna valutazione finora
- Sagan, L. On The Origin of Mitosing Cells. J. Theoret. Biol. (1967) 14, 225-274Documento56 pagineSagan, L. On The Origin of Mitosing Cells. J. Theoret. Biol. (1967) 14, 225-274Jéssica CristinaNessuna valutazione finora
- Test Bank For Microbiology The Human Experience Preliminary EditionDocumento36 pagineTest Bank For Microbiology The Human Experience Preliminary Editionquinazolmadraguevlvvsh100% (42)
- Halophiles PDFDocumento11 pagineHalophiles PDFWulan PurnamasariNessuna valutazione finora
- SLM Biotech Wekk 1 2Documento7 pagineSLM Biotech Wekk 1 2Petronila LumaguiNessuna valutazione finora
- College B Otan Y: (NimohDocumento1.209 pagineCollege B Otan Y: (NimohFATIMA HASANNessuna valutazione finora
- Therapeutic Effects of Dairy ProductsDocumento8 pagineTherapeutic Effects of Dairy ProductsSachin VermaNessuna valutazione finora
- Keneuoe MohlakoanaDocumento137 pagineKeneuoe MohlakoanaDurga BhavaniNessuna valutazione finora