Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Ophthalmology PDFDocumento28 pagineOphthalmology PDFKukuh Rizwido PrasetyoNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Stress Management PPT FinalDocumento7 pagineStress Management PPT FinalAdarsh Meher100% (1)
- The Role of Orthodontics in Temporomandibular DisordersDocumento19 pagineThe Role of Orthodontics in Temporomandibular DisordersAngel Rubén Orozco RodríguezNessuna valutazione finora
- Obstetric + Co Morbid AnesthesiaDocumento247 pagineObstetric + Co Morbid AnesthesiaPandhu Suprobo100% (3)
- A Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESDocumento57 pagineA Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESLane Mae Magpatoc NoerrotNessuna valutazione finora
- 4.management of Vertical Discrepancies (2) 2Documento97 pagine4.management of Vertical Discrepancies (2) 2Arun Joy100% (2)
- Educational Training Manual: Certification Board, IncDocumento58 pagineEducational Training Manual: Certification Board, IncAlexander MaukinNessuna valutazione finora
- Nursing Process DiagnosisDocumento20 pagineNursing Process DiagnosisGabz Gabby100% (1)
- Genu ValgumDocumento2 pagineGenu ValgumPurohit_R0% (1)
- Reliability of Pulse Palpation in The Detection of Atrial Fibrillation in An Elderly PopulationDocumento6 pagineReliability of Pulse Palpation in The Detection of Atrial Fibrillation in An Elderly PopulationAnonymous SWtvkTYGONessuna valutazione finora
- ALERTEC (Modafinil) Product Monograph For CanadaDocumento38 pagineALERTEC (Modafinil) Product Monograph For Canadajennabush100% (2)
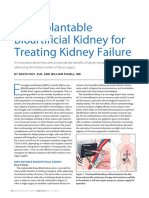
- An Implantable Bioartificial Kidney For Treating Kidney FailureDocumento2 pagineAn Implantable Bioartificial Kidney For Treating Kidney FailureAnugrah Pangeran100% (1)
- Health Problem Family Nursing Problem Goal of Care Objectives of Care Intervention PlanDocumento2 pagineHealth Problem Family Nursing Problem Goal of Care Objectives of Care Intervention PlanCarol MalcoNessuna valutazione finora
- Introduction of The ResearchDocumento3 pagineIntroduction of The Researchcristine baldazoNessuna valutazione finora
- Adr ReportingDocumento8 pagineAdr ReportingDRRAJAN1Nessuna valutazione finora
- Altered Sensorium and Care of Unconscious PatientsDocumento17 pagineAltered Sensorium and Care of Unconscious PatientsChhabilal BastolaNessuna valutazione finora
- BooksDocumento12 pagineBookschakriy9Nessuna valutazione finora
- ESCHAROTOMYDocumento31 pagineESCHAROTOMYSusan Rose FuertesNessuna valutazione finora
- Entreprenurse BrochureDocumento2 pagineEntreprenurse Brochurederic100% (2)
- Legal and Ethical Issues-ModifiedDocumento29 pagineLegal and Ethical Issues-Modifiedmonir61100% (1)
- Encopresis and EnuresisDocumento10 pagineEncopresis and EnuresisRoci ArceNessuna valutazione finora
- Essay On AidsDocumento6 pagineEssay On AidsBharat SinghNessuna valutazione finora
- HMS-PSG Revenue Maximization Proposal To WV Dept of Health and Human Resources (2012)Documento278 pagineHMS-PSG Revenue Maximization Proposal To WV Dept of Health and Human Resources (2012)Rick ThomaNessuna valutazione finora
- Camp Hulaco Permission FormDocumento1 paginaCamp Hulaco Permission Formmattkimbennett2495Nessuna valutazione finora
- Diabetic RetinopathyDocumento55 pagineDiabetic RetinopathyMuhammad Bilal SaifulhaqNessuna valutazione finora
- Director Emergency Medical Services in Nashville TN Resume Steve FustonDocumento2 pagineDirector Emergency Medical Services in Nashville TN Resume Steve FustonSteveFustonNessuna valutazione finora
- Rheumatoid 4Documento14 pagineRheumatoid 4Mohamed AbozeidNessuna valutazione finora
- MDS UpdrsDocumento42 pagineMDS UpdrsdquebradasNessuna valutazione finora
- Paederus Dermatitis: A Case SeriesDocumento5 paginePaederus Dermatitis: A Case SeriesrositaNessuna valutazione finora
- Nursing Care and Do-Not-Resuscitate (DNR) Decisions: PurposeDocumento6 pagineNursing Care and Do-Not-Resuscitate (DNR) Decisions: PurposeBea-ayesha A. PandaoNessuna valutazione finora