Potrebbero piacerti anche
- Panoramic: Radiographs: A Tool For Investigating Skeletal PatternDocumento22 paginePanoramic: Radiographs: A Tool For Investigating Skeletal Patterneddy1012805361Nessuna valutazione finora
- Anestesia Local Cara PDFDocumento16 pagineAnestesia Local Cara PDFeddy1012805361100% (1)
- Chest RadiographyDocumento23 pagineChest Radiographyapi-3773951100% (2)
- Prevention of Dry Socket PDFDocumento4 paginePrevention of Dry Socket PDFeddy1012805361Nessuna valutazione finora
- Tetraciclinas en Alveolitis SecaDocumento5 pagineTetraciclinas en Alveolitis Secaeddy1012805361Nessuna valutazione finora
- Prevention of Dry Socket PDFDocumento4 paginePrevention of Dry Socket PDFeddy1012805361Nessuna valutazione finora
- Prevention of Dry Socket PDFDocumento4 paginePrevention of Dry Socket PDFeddy1012805361Nessuna valutazione finora
- Clinical Concepts of Dry SocketDocumento11 pagineClinical Concepts of Dry Socketeddy1012805361Nessuna valutazione finora
- Abordaje TransparotideoDocumento6 pagineAbordaje Transparotideoeddy1012805361Nessuna valutazione finora
- Preauricular Incision Outlining During A Face-Lift - A Step-by-Step Description PDFDocumento5 paginePreauricular Incision Outlining During A Face-Lift - A Step-by-Step Description PDFeddy1012805361Nessuna valutazione finora
- OCO Biomedical 2013 Product Catalog 10-2013Documento28 pagineOCO Biomedical 2013 Product Catalog 10-2013eddy1012805361Nessuna valutazione finora
- Air Leak SyndromeDocumento57 pagineAir Leak Syndromeeddy1012805361Nessuna valutazione finora
- Anatomia de La Atm e Imagenologia PDFDocumento21 pagineAnatomia de La Atm e Imagenologia PDFeddy1012805361Nessuna valutazione finora
- Retro Mandibular Id Approach For ORIF of Condylar FracturesDocumento1 paginaRetro Mandibular Id Approach For ORIF of Condylar Fractureseddy1012805361Nessuna valutazione finora
- Biodegradable Fixation of Mandibular Fractures in ChildrenDocumento8 pagineBiodegradable Fixation of Mandibular Fractures in Childreneddy1012805361Nessuna valutazione finora
- Long Term FearDocumento12 pagineLong Term FearAdi PraTamaNessuna valutazione finora
- EzlaseDocumento7 pagineEzlaseeddy1012805361Nessuna valutazione finora
- Abordaje TransparotideoDocumento6 pagineAbordaje Transparotideoeddy1012805361Nessuna valutazione finora
- MDASscaleDocumento2 pagineMDASscaleeddy1012805361100% (2)
- Dental Anxiety ScaleDocumento2 pagineDental Anxiety Scaleeddy1012805361100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Intramedullary Headless Screw Fixation For Metacarpal FracturesDocumento7 pagineIntramedullary Headless Screw Fixation For Metacarpal FracturesErlin EsauNessuna valutazione finora
- Disseminated Intravascular CoagulationDocumento1 paginaDisseminated Intravascular CoagulationAnn Justine OrbetaNessuna valutazione finora
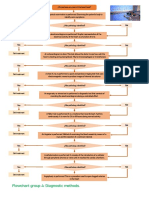
- Flowchart Group 4 Diagnostic Methods.Documento1 paginaFlowchart Group 4 Diagnostic Methods.Grupo 4 CardiologiaNessuna valutazione finora
- Tarrass FDocumento2 pagineTarrass FDr. Jatin GargNessuna valutazione finora
- Coronary Artery Bypass Grafting: Cabg - OpcabDocumento49 pagineCoronary Artery Bypass Grafting: Cabg - OpcabdeNessuna valutazione finora
- Ot TechniqueDocumento21 pagineOt TechniqueVelpulakavyasree SonuNessuna valutazione finora
- Abdominal ExaminationDocumento9 pagineAbdominal Examinationthunderlike30Nessuna valutazione finora
- Cruz vs. Agas, Jr.Documento10 pagineCruz vs. Agas, Jr.June Glenn Barcarse UgaldeNessuna valutazione finora
- Surgical Instruments 3Documento110 pagineSurgical Instruments 3Gerald Resubal OriñaNessuna valutazione finora
- Ultimate Examination Bundle - 221111 - 203054Documento717 pagineUltimate Examination Bundle - 221111 - 203054musayyab muz100% (1)
- Carotid UltrasoundDocumento9 pagineCarotid UltrasoundLora LefterovaNessuna valutazione finora
- Contoured 3D Mesh in Laparoscopic Inguinal Hernia Repair: Does It Reduce Inguinodynia?Documento8 pagineContoured 3D Mesh in Laparoscopic Inguinal Hernia Repair: Does It Reduce Inguinodynia?RiddhiNessuna valutazione finora
- Post Test AtlsDocumento6 paginePost Test Atlsnurul huda85% (62)
- Full Announcement - PIN - IKABDI - 2023Documento21 pagineFull Announcement - PIN - IKABDI - 2023kucing9956Nessuna valutazione finora
- Primary Open Rhinoplasty: Preoperative Assessment and PlanningDocumento16 paginePrimary Open Rhinoplasty: Preoperative Assessment and PlanningМаратNessuna valutazione finora
- Minimally Evasive SurgeryDocumento4 pagineMinimally Evasive Surgerydivine venturoNessuna valutazione finora
- Central Vein Stenosis: A Nephrologist's PerspectiveDocumento10 pagineCentral Vein Stenosis: A Nephrologist's PerspectiverinayondaNessuna valutazione finora
- Liver AbscessDocumento6 pagineLiver AbscessKenneth SunicoNessuna valutazione finora
- Hip ExaminationDocumento84 pagineHip ExaminationDeepak KumarNessuna valutazione finora
- Medical TextilesDocumento30 pagineMedical TextilesDr Muhammad Mushtaq MangatNessuna valutazione finora
- Significance of Sushrutokta Chedana Karma in BhagandaraDocumento5 pagineSignificance of Sushrutokta Chedana Karma in BhagandaraResearch ParkNessuna valutazione finora
- Pregnancy in Women With Congenital Heart DiseaseDocumento24 paginePregnancy in Women With Congenital Heart DiseaseGian AlvaradoNessuna valutazione finora
- Basic Echocardiography: Presentor:-Dr. Ashutosh DATE: - 14/09/2017Documento71 pagineBasic Echocardiography: Presentor:-Dr. Ashutosh DATE: - 14/09/2017Ms. ISHA SHARMANessuna valutazione finora
- Colonoscopy ProcedureDocumento2 pagineColonoscopy ProcedureNick Arngel CorporalNessuna valutazione finora
- MAC Vs TIVADocumento2 pagineMAC Vs TIVARicky JalecoNessuna valutazione finora
- Presention SdaDocumento13 paginePresention SdaBikhu MatreNessuna valutazione finora
- Bullets: "Victory Belongs To Those Who Are Most Persevering. Ad Majorem Dei Gloriam."Documento15 pagineBullets: "Victory Belongs To Those Who Are Most Persevering. Ad Majorem Dei Gloriam."Johnmer Avelino100% (1)
- Final Rectal Cancer GEC ESTRO Handbook of BrachytherapyDocumento14 pagineFinal Rectal Cancer GEC ESTRO Handbook of BrachytherapyRakesh JadhavNessuna valutazione finora
- MCQ On Paediatric SurgeryDocumento3 pagineMCQ On Paediatric Surgeryhabtsh habshaNessuna valutazione finora
- Biology ProjectDocumento21 pagineBiology ProjectsivaNessuna valutazione finora