Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Kemu Hsci 225 Seminar Lecture MaterialsDocumento50 pagineKemu Hsci 225 Seminar Lecture MaterialsAlice WairimuNessuna valutazione finora
- Most Expected Vocabulary Ebook by Prashant SirDocumento35 pagineMost Expected Vocabulary Ebook by Prashant SirPriya GuptaNessuna valutazione finora
- Uwise HYDocumento3 pagineUwise HYJack GuccioneNessuna valutazione finora
- The Tonsils (Waldeyer's Ring) - Lingual - Pharyngeal - Palatine - Tubal - TeachMeAnatomyDocumento4 pagineThe Tonsils (Waldeyer's Ring) - Lingual - Pharyngeal - Palatine - Tubal - TeachMeAnatomywachito ricoNessuna valutazione finora
- Breathing A FoundationDocumento267 pagineBreathing A FoundationJanaki100% (1)
- Xanthone Ekstrak Kulit Manggis Sebagai Antibakteri Pada Karies DentinDocumento5 pagineXanthone Ekstrak Kulit Manggis Sebagai Antibakteri Pada Karies DentindlopitaaNessuna valutazione finora
- Bone Morphogenic Protein ReviewDocumento7 pagineBone Morphogenic Protein ReviewdlopitaaNessuna valutazione finora
- Bone-Graft Substitutes:: Facts, Fictions & ApplicationsDocumento0 pagineBone-Graft Substitutes:: Facts, Fictions & ApplicationsdlopitaaNessuna valutazione finora
- Evaluating Iodine Deficiency in Pregnant Women and Young Infants-Complex Physiology With A Risk of MisinterpretationDocumento6 pagineEvaluating Iodine Deficiency in Pregnant Women and Young Infants-Complex Physiology With A Risk of MisinterpretationdlopitaaNessuna valutazione finora
- Urinary Incontinence Following Gynaecological SurgeryDocumento6 pagineUrinary Incontinence Following Gynaecological SurgeryDwickyNessuna valutazione finora
- 10.anatomy of Respiratory SystemDocumento23 pagine10.anatomy of Respiratory SystemMai Z HaniyaNessuna valutazione finora
- Tutorial 1.1 - Measuring Disease Occurence (Morbidity) - Students - UpdateDocumento3 pagineTutorial 1.1 - Measuring Disease Occurence (Morbidity) - Students - UpdateFebriansyah 'ebhi'100% (1)
- Fapc Finals ReviewerDocumento303 pagineFapc Finals ReviewerC BajamondeNessuna valutazione finora
- MLAB 2361 Clinical II Immunohematology Assignment Activity 6: ABO Discrepancies Case StudiesDocumento7 pagineMLAB 2361 Clinical II Immunohematology Assignment Activity 6: ABO Discrepancies Case Studiespikachu0% (1)
- Prostho#8Documento9 pagineProstho#8api-19840404Nessuna valutazione finora
- Neumonia Oculta Por DeshidratacionDocumento2 pagineNeumonia Oculta Por DeshidratacionLorena BuitragoNessuna valutazione finora
- Methemoglobin Reductase PathwayDocumento2 pagineMethemoglobin Reductase PathwayinshNessuna valutazione finora
- Reproductive Nursing SystemDocumento17 pagineReproductive Nursing SystemBobby Dwi PutraNessuna valutazione finora
- Useful Phrases For Sensational WritingDocumento3 pagineUseful Phrases For Sensational WritingNor Azizah BachokNessuna valutazione finora
- Trial SPM SBP 2010 Biology Marking SchemeDocumento24 pagineTrial SPM SBP 2010 Biology Marking SchemeMr.D-SIM100% (6)
- AcknowledgementDocumento9 pagineAcknowledgementJovin AshickNessuna valutazione finora
- Retention and RelapseDocumento32 pagineRetention and RelapseRana SayedNessuna valutazione finora
- Diagnostic MethodsDocumento93 pagineDiagnostic MethodsSyukri La Ranti100% (3)
- TCM Tongue Diagnosis - Join The RAWvolutionDocumento4 pagineTCM Tongue Diagnosis - Join The RAWvolutionJing CruzNessuna valutazione finora
- Module 11Documento7 pagineModule 11Jamille Nympha C. BalasiNessuna valutazione finora
- BeekeepingDocumento17 pagineBeekeepingApollon Phebo0% (1)
- Chapter XNXXXDocumento3 pagineChapter XNXXXclaudette100% (2)
- Host Parasite InteractionDocumento20 pagineHost Parasite InteractionRhomizal MazaliNessuna valutazione finora
- Mother's Class BFDocumento55 pagineMother's Class BFriz04_fortitudessa5178Nessuna valutazione finora
- 356 India Fact Sheets PDFDocumento2 pagine356 India Fact Sheets PDFgomathi ShankarNessuna valutazione finora
- Concept Map On CVA Bleed Left Thalamo-Ganglionic Bleed Patient Name: Mr. DGDDocumento1 paginaConcept Map On CVA Bleed Left Thalamo-Ganglionic Bleed Patient Name: Mr. DGDBert Brian Bolido100% (1)
- Practical PhysiologyDocumento436 paginePractical Physiologyaastha212002100% (1)
- Kawasaki DiseaseDocumento47 pagineKawasaki DiseaseChristine Karen Ang Suarez100% (1)
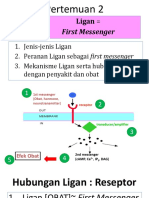
- 2 Ligan First MassengerDocumento32 pagine2 Ligan First MassengerikhararaNessuna valutazione finora