Potrebbero piacerti anche
- Giant Bullous Reaction in Response To Tuberculin Test in A Patient of Pelvic Inflammatory DiseaseDocumento2 pagineGiant Bullous Reaction in Response To Tuberculin Test in A Patient of Pelvic Inflammatory DiseaseGopal ChawlaNessuna valutazione finora
- 5 PPFDocumento4 pagine5 PPFGopal ChawlaNessuna valutazione finora
- 8 FB EmpyemaDocumento3 pagine8 FB EmpyemaGopal ChawlaNessuna valutazione finora
- 4 NpeDocumento3 pagine4 NpeGopal ChawlaNessuna valutazione finora
- 3 NIV BRonchiectaisDocumento6 pagine3 NIV BRonchiectaisGopal ChawlaNessuna valutazione finora
- Use Only: Obstructive Sleep Apnoea With Co Existent Kleine-Levine Syndrome in A Middle-Aged ManDocumento3 pagineUse Only: Obstructive Sleep Apnoea With Co Existent Kleine-Levine Syndrome in A Middle-Aged ManGopal ChawlaNessuna valutazione finora
- Use Only: Obstructive Sleep Apnoea With Co Existent Kleine-Levine Syndrome in A Middle-Aged ManDocumento3 pagineUse Only: Obstructive Sleep Apnoea With Co Existent Kleine-Levine Syndrome in A Middle-Aged ManGopal ChawlaNessuna valutazione finora
- 5 PPFDocumento4 pagine5 PPFGopal ChawlaNessuna valutazione finora
- 8 FB EmpyemaDocumento3 pagine8 FB EmpyemaGopal ChawlaNessuna valutazione finora
- 4 NpeDocumento3 pagine4 NpeGopal ChawlaNessuna valutazione finora
- Lung Cancer (Autosaved)Documento35 pagineLung Cancer (Autosaved)Gopal ChawlaNessuna valutazione finora
- Congenital Anomalies of Airway and Lung ParenchymaDocumento71 pagineCongenital Anomalies of Airway and Lung ParenchymaGopal ChawlaNessuna valutazione finora
- Giant Bullous Reaction in Response To Tuberculin Test in A Patient of Pelvic Inflammatory DiseaseDocumento2 pagineGiant Bullous Reaction in Response To Tuberculin Test in A Patient of Pelvic Inflammatory DiseaseGopal ChawlaNessuna valutazione finora
- Bronchiectasis Sicca Napcon12Documento1 paginaBronchiectasis Sicca Napcon12Gopal ChawlaNessuna valutazione finora
- Tuberculosis and Chronic Renal FailureDocumento38 pagineTuberculosis and Chronic Renal FailureGopal ChawlaNessuna valutazione finora
- Tuberculosis and Chronic Renal FailureDocumento38 pagineTuberculosis and Chronic Renal FailureGopal ChawlaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Negative AutopsyDocumento21 pagineNegative Autopsydr rizwanNessuna valutazione finora
- Indonesia Health SectorDocumento84 pagineIndonesia Health SectorBung RandiNessuna valutazione finora
- MeningitisDocumento2 pagineMeningitisapi-491868042Nessuna valutazione finora
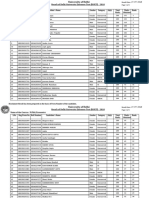
- Name of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Documento5 pagineName of The Course:-M.Phil, Economics: Result of Delhi University Entrance Test (DUET) - 2018Saiganesh RameshNessuna valutazione finora
- Dengue ReportDocumento1 paginaDengue Reportjed larsen capulong gavinoNessuna valutazione finora
- Colorectal Disease - 2023 - Freund - Can Preoperative CT MR Enterography Preclude The Development of Crohn S Disease LikeDocumento10 pagineColorectal Disease - 2023 - Freund - Can Preoperative CT MR Enterography Preclude The Development of Crohn S Disease Likedavidmarkovic032Nessuna valutazione finora
- Chronic Obstructive Pulmonary Disease COPDDocumento25 pagineChronic Obstructive Pulmonary Disease COPDKat OrtegaNessuna valutazione finora
- Gambaran Usia Pada Kejadian Covid-19: Rosyada Elviani Chairil Anwar Rico Januar SitorusDocumento6 pagineGambaran Usia Pada Kejadian Covid-19: Rosyada Elviani Chairil Anwar Rico Januar SitorusRizka ZahroNessuna valutazione finora
- Sexually Transmitted DiseasesDocumento54 pagineSexually Transmitted DiseasesMowlidAbdirahman Ali madaaleNessuna valutazione finora
- Clinical Treatment of Rabbits Experimentally Infected With Staphylococcus Aureus Using Different AntibioticsDocumento4 pagineClinical Treatment of Rabbits Experimentally Infected With Staphylococcus Aureus Using Different Antibioticsarum pratiwiNessuna valutazione finora
- NTP MOP 6th Ed Module 4 Diagnosis of Tuberculosis 10.20.20Documento50 pagineNTP MOP 6th Ed Module 4 Diagnosis of Tuberculosis 10.20.20gbNessuna valutazione finora
- Nursing Care PlanDocumento5 pagineNursing Care PlanChriss Una PacamalanNessuna valutazione finora
- Complete Education MudrasDocumento10 pagineComplete Education MudrasRomanoJovanovicNessuna valutazione finora
- Brucellosis BmelitensisDocumento38 pagineBrucellosis Bmelitensisalvaro acNessuna valutazione finora
- Part C - Multiple SclerosisDocumento4 paginePart C - Multiple SclerosisStaph AureusNessuna valutazione finora
- ATLS Post TestDocumento1 paginaATLS Post Testanon_57896987836% (56)
- The Role of Imaging in The Diagnosis of Bronchiectasis: The Key Is in The DistributionDocumento3 pagineThe Role of Imaging in The Diagnosis of Bronchiectasis: The Key Is in The DistributionrosmeniNessuna valutazione finora
- Measurements in EpidemiologyDocumento24 pagineMeasurements in EpidemiologyAnand gowda75% (4)
- Health Resources Center: Kingsport ScheduleDocumento2 pagineHealth Resources Center: Kingsport ScheduleJack MiguelNessuna valutazione finora
- Disease and Immunity Paper 2 QuestionsDocumento38 pagineDisease and Immunity Paper 2 QuestionsBalachandran PalaniandyNessuna valutazione finora
- Baby Massage Consultation Form - November 2017Documento1 paginaBaby Massage Consultation Form - November 2017api-257327106Nessuna valutazione finora
- Fracture PathophysiologyDocumento1 paginaFracture PathophysiologyIrene Joy Gomez100% (2)
- Bloodborne Pathogens PPT v-03!01!17Documento44 pagineBloodborne Pathogens PPT v-03!01!17kunalphalswal0005Nessuna valutazione finora
- Health Declaration Form Health Declaration FormDocumento1 paginaHealth Declaration Form Health Declaration FormGerone NavaeraNessuna valutazione finora
- Answers To ExercisesDocumento19 pagineAnswers To ExercisesBea ValerioNessuna valutazione finora
- Aids HivDocumento140 pagineAids HivKarina Flores RezpkaNessuna valutazione finora
- DR Thomas Levy COVID 19 Viral DefenseDocumento24 pagineDR Thomas Levy COVID 19 Viral DefenseKaterina PoposkaNessuna valutazione finora
- Community Medicine Module Book PDFDocumento37 pagineCommunity Medicine Module Book PDFLiya SuwarniNessuna valutazione finora
- HIV in Children: Preventing Mother-to-Child Transmission (Dr. Laura Guay)Documento27 pagineHIV in Children: Preventing Mother-to-Child Transmission (Dr. Laura Guay)National Press FoundationNessuna valutazione finora
- BIU Clinic FormsDocumento4 pagineBIU Clinic FormsMarvellous AbrahamNessuna valutazione finora