If Mailing Completed Form From the If Mailing Completed Form From All Other
United States: Places:
U.S. Department of Veterans Affairs U.S. Department of Veterans Affairs
Manila Regional Office 1131 Roxas Blvd.
PSC 501 0930 Manila Philippines
FPO AP 96515-1100
STATEMENT IN SUPPORT OF CLAIM (Filipino Veterans Equity Compensation Fund)
PRIVACY ACT INFORMATION: The VA will not disclose information collected on this form to any source other than what has been authorized under the Privacy Act of 1974 or Title 38,
Code of Federal Regulations 1.576 for routine uses (i.e., civil or criminal law enforcement, congressional communications, epidemiological or research studies, the collection of money owed to
the United States, litigation in which the United States is a party or has an interest, the administration of VA Programs and delivery of VA benefits, verification of identity and status, and
personnel administration) as identified in the VA system of records, 58VA21/22, Compensation, Pension, Education and Rehabilitation Records - VA, published in the Federal Register. Your
obligation to respond is required to obtain or retain benefits. VA uses your SSN to identify your claim file. Providing your SSN will help ensure that your records are properly associated with
your claim file. Giving us your SSN account information is voluntary. Refusal to provide your SSN by itself will not result in the denial of benefits. The VA will not deny an individual benefits
for refusing to provide his or her SSN unless the disclosure of the SSN is required by Federal Statute of law in effect prior to January 1, 1975, and still in effect. The requested information is
considered relevant and necessary to determine maximum benefits under the law. The responses you submit are considered confidential (38 U.S.C. 5701). Information submitted is subject to
verification through computer matching programs with other agencies.
RESPONDENT BURDEN: We need this information to obtain evidence in support of your claim for benefits (38 U.S.C. 501(a) and (b)). Title 38, United States Code, allows us to ask for this
information. We estimate that you will need an average of 15 minutes to review the instructions, find the information, and complete this form. VA cannot conduct or sponsor a collection of
information unless a valid OMB control number is displayed. You are not required to respond to a collection of information if this number is not displayed. Valid OMB control numbers can be
located on the OMB Internet Page at www.whitehouse.gov/omb/library/OMBINV.VA.EPA.html#VA. If desired, you can call 1-800-827-1000 to get information on where to send comments
or suggestions about this form.
FIRST NAME - MIDDLE NAME - LAST NAME OF VETERAN (Type or print) SOCIAL SECURITY NO. VA FILE NO.
C/CSS -
The following statement is made in connection with a claim for benefits in the case of the above-named veteran:
I am applying for a one-time payment from the Filpino Veterans Equity Compensation Fund as a honorably discharged veteran who served, before July
1, 1946, in the organized military forces of the Government of the Commonwealth of the Philippines, including certain service in the Philippine Scouts or
in organized guerrilla forces recognized by the United States Army, while such forces were in the service of the Armed Forces of the United States.
I served in: Commonwealth Army Recognized Guerilla New Philippine Scouts
Date of Birth: Place of Birth:
Service Number:
Unit in Which Served:
Dates of Service: From: To:
Father’s Name: Mother’s Name:
Name of Current Spouse:
Date of Marriage: Spouse’s Date of Birth:
Address of Current Spouse
(If different from veteran’s
current address):
PVAO Account Number:
(If applicable)
I Am a U.S. Citizen: U.S. Passport No.:
YES NO
IMPORTANT - Use this form only with claims under the Filipino Veterans Equity Compensation Fund. The Department of Veterans
Affairs must receive this form on or before February 16, 2010, to consider your claim for this benefit.
I CERTIFY THAT the statements on this form are true and correct to the best of my knowledge and belief.
SIGNATURE DATE SIGNED
ADDRESS TELEPHONE NUMBERS (Include Area Code)
DAYTIME EVENING
PENALTY: The law provides severe penalties which include fine or imprisonment, or both, for the willful submission of any statement or evidence of a material fact,
knowing it to be false.
VA FORM
FEB 2009 21-4138(CF)
Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Basu and Dutta Accountancy Book Class 12 SolutionsDocumento14 pagineBasu and Dutta Accountancy Book Class 12 SolutionsGourab Gorai23% (30)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Preboard Civil ServiceDocumento26 paginePreboard Civil ServiceYaj CruzadaNessuna valutazione finora
- Know Your Power - Visualization and Affirmation ExercisesDocumento51 pagineKnow Your Power - Visualization and Affirmation ExercisesLorna Dietz100% (1)
- San Francisco Exhibit: Weaving Peace and Dreams - Textile Arts of MindanaoDocumento2 pagineSan Francisco Exhibit: Weaving Peace and Dreams - Textile Arts of MindanaoLorna DietzNessuna valutazione finora
- Elections Strikes D11 Candidate's Chinese Name and Replaces It With Gibberish - Francisco Herrera For D11 Board of SupervisorsDocumento1 paginaElections Strikes D11 Candidate's Chinese Name and Replaces It With Gibberish - Francisco Herrera For D11 Board of SupervisorsLorna DietzNessuna valutazione finora
- June 24, 2016 - Kalayaan SF Cecile Licad Piano Concert and Gala Reception, Philippine Independence Day CelebrationDocumento1 paginaJune 24, 2016 - Kalayaan SF Cecile Licad Piano Concert and Gala Reception, Philippine Independence Day CelebrationLorna DietzNessuna valutazione finora
- Philippine Independence Day 2016 On June 11, 2016 at Hercules LibraryDocumento1 paginaPhilippine Independence Day 2016 On June 11, 2016 at Hercules LibraryLorna DietzNessuna valutazione finora
- San Francisco Police Department Philippine Exchange Training: Executive Summary As of January 2005Documento4 pagineSan Francisco Police Department Philippine Exchange Training: Executive Summary As of January 2005Lorna DietzNessuna valutazione finora
- Philippine Cacao Summit - Program As of May 18 2016Documento8 paginePhilippine Cacao Summit - Program As of May 18 2016Lorna DietzNessuna valutazione finora
- 2nd ENFiD General Assembly and Regional European Conference To Be Held in MaltaDocumento4 pagine2nd ENFiD General Assembly and Regional European Conference To Be Held in MaltaLorna DietzNessuna valutazione finora
- Federation 2015 Registration Form For Nov. 6-8, 2015, Las Vegas, NVDocumento4 pagineFederation 2015 Registration Form For Nov. 6-8, 2015, Las Vegas, NVLorna DietzNessuna valutazione finora
- Your Guide To Nuvali: Ayala Land in The PhilippinesDocumento9 pagineYour Guide To Nuvali: Ayala Land in The PhilippinesLorna DietzNessuna valutazione finora
- Situational Analysis of Public Health Nursing Personnel in IndiaDocumento60 pagineSituational Analysis of Public Health Nursing Personnel in IndiaTamilNurse.com100% (1)
- Practical Guide For PHD Candidates at Epfl: Version: August 12, 2008Documento91 paginePractical Guide For PHD Candidates at Epfl: Version: August 12, 2008rjohn1Nessuna valutazione finora
- Sai Vidya Institute of Technology: Department of Civil EngineeringDocumento9 pagineSai Vidya Institute of Technology: Department of Civil EngineeringSrinivasNessuna valutazione finora
- Bruno - 2018.02.06 - TESI DEF PDFDocumento349 pagineBruno - 2018.02.06 - TESI DEF PDFΝικολαος ΑΥτιαςNessuna valutazione finora
- Checkpoint: Code of EthicsDocumento2 pagineCheckpoint: Code of EthicsFathalla ElmansouryNessuna valutazione finora
- EXTAC - 1010 - Rev - NONCOMBATANT EVACUATION OPERATIONSDocumento96 pagineEXTAC - 1010 - Rev - NONCOMBATANT EVACUATION OPERATIONSAbrarNessuna valutazione finora
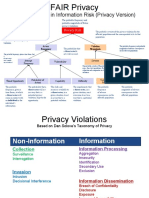
- Factor Analysis in Information Risk (Privacy Version)Documento8 pagineFactor Analysis in Information Risk (Privacy Version)Otgonbayar TsengelNessuna valutazione finora
- ITE182 Syllabus AY2020-2021 2ndsemDocumento6 pagineITE182 Syllabus AY2020-2021 2ndsemLucman AbdulrachmanNessuna valutazione finora
- The 10th HouseDocumento7 pagineThe 10th HouseRavindra LeleNessuna valutazione finora
- DCP Chapter 8Documento7 pagineDCP Chapter 8hemkumar DahalNessuna valutazione finora
- Dale Carnige TTT RequirementsDocumento4 pagineDale Carnige TTT RequirementskrishnachivukulaNessuna valutazione finora
- HRM Jury Assignment - Part 1.case StudyDocumento7 pagineHRM Jury Assignment - Part 1.case StudyNAMITHA KINessuna valutazione finora
- 18 06 08 Primark-2Documento2 pagine18 06 08 Primark-2Sachin RailhanNessuna valutazione finora
- Teaching Methodology For LiteratureDocumento7 pagineTeaching Methodology For Literaturekaif us sehar shaikhNessuna valutazione finora
- CRediT Author StatementDocumento2 pagineCRediT Author StatementCarlos MaroveNessuna valutazione finora
- Defining Literacies - Language Arts.1Documento26 pagineDefining Literacies - Language Arts.1drwindsurfNessuna valutazione finora
- Action Plan For Closing The Achievement Gap in A Foreign Language ClassroomDocumento8 pagineAction Plan For Closing The Achievement Gap in A Foreign Language Classroomsw4738100% (1)
- CV Muhammad Imran Riaz 1 P A G e MobiSerDocumento3 pagineCV Muhammad Imran Riaz 1 P A G e MobiSerAmna Khan YousafzaiNessuna valutazione finora
- ACI Policies and Recommended Practices Seventh Edition FINAL v2Documento129 pagineACI Policies and Recommended Practices Seventh Edition FINAL v2Valmir AndradeNessuna valutazione finora
- Services Marketing Course TasterDocumento54 pagineServices Marketing Course TasterAmit KumarNessuna valutazione finora
- Kennedy School BrochureDocumento2 pagineKennedy School BrochureBrennan GamwellNessuna valutazione finora
- Reading V - Customs and Warehouse ServicesDocumento3 pagineReading V - Customs and Warehouse ServicesRous TobarNessuna valutazione finora
- Please Introduce Yourself Briefly ?Documento2 paginePlease Introduce Yourself Briefly ?Wahyu SaputroNessuna valutazione finora
- Books British English TeacherDocumento6 pagineBooks British English TeacherJohn SmithNessuna valutazione finora
- Muhammad Alif B. Mohd AnuarDocumento2 pagineMuhammad Alif B. Mohd AnuarAlif AnuarNessuna valutazione finora
- MCQ On Smart GridDocumento4 pagineMCQ On Smart GridJoshi RohitNessuna valutazione finora
- Community Health Nursing Notes (Second Year)Documento6 pagineCommunity Health Nursing Notes (Second Year)anette katrinNessuna valutazione finora
- Learn With Facebook - Digital-Skills-Modules-Combined-04-24 PDFDocumento182 pagineLearn With Facebook - Digital-Skills-Modules-Combined-04-24 PDFMostesareNessuna valutazione finora