Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Coagulation Cascade (Hema)Documento4 pagineCoagulation Cascade (Hema)MarjoNessuna valutazione finora
- Assessment Hema PDFDocumento9 pagineAssessment Hema PDFAnne MorenoNessuna valutazione finora
- HemophiliaDocumento135 pagineHemophiliaDivyashri Baraniya100% (1)
- Vita KDocumento31 pagineVita KPabitra ThapaNessuna valutazione finora
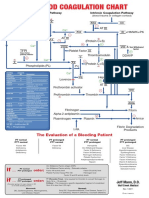
- Blood Clotting ChartDocumento1 paginaBlood Clotting ChartBianca SimionescuNessuna valutazione finora
- Hemostasis and Blood CoagulationDocumento9 pagineHemostasis and Blood CoagulationHans De GuzmanNessuna valutazione finora
- DivitiDocumento36 pagineDivitiMarLeniRNNessuna valutazione finora
- Hemostasis Practice: State-Of-The-Art: Giuseppe Lippi, Emmanuel J. FavaloroDocumento6 pagineHemostasis Practice: State-Of-The-Art: Giuseppe Lippi, Emmanuel J. FavaloroRilia IrianiNessuna valutazione finora
- HEMOPHILIADocumento70 pagineHEMOPHILIAtoyyibNessuna valutazione finora
- Direct Oral Anticoagulants From Pharmacology To Clinical PracticeDocumento283 pagineDirect Oral Anticoagulants From Pharmacology To Clinical PracticesunhaolanNessuna valutazione finora
- Chapter Blood: RBC Platelet HemostasisDocumento89 pagineChapter Blood: RBC Platelet Hemostasisapi-19916399100% (1)
- 2020 Therapeutic Strategies For Thrombosis - New Targets and ApproachesDocumento20 pagine2020 Therapeutic Strategies For Thrombosis - New Targets and ApproachesVladimir BasurtoNessuna valutazione finora
- Diajukan Untuk Melengkapi Persyaratan Mencapai Gelar Dokter Spesialis Penyakit DalamDocumento70 pagineDiajukan Untuk Melengkapi Persyaratan Mencapai Gelar Dokter Spesialis Penyakit DalamMohammad SutamiNessuna valutazione finora
- Anticoagulants, Fibrinolytics, AntiplateletsDocumento88 pagineAnticoagulants, Fibrinolytics, Antiplateletspmuawiyah25Nessuna valutazione finora
- 2.7.4. Assay of Human Coagulation Factor VIIIDocumento1 pagina2.7.4. Assay of Human Coagulation Factor VIIIMulayam Singh Yadav100% (1)
- Ain Shams University - Clinical Pathology Ain ShamsDocumento182 pagineAin Shams University - Clinical Pathology Ain ShamsRowaa SamehNessuna valutazione finora
- Andexxa-An Antidote For Apixaban and RivaroxabanDocumento2 pagineAndexxa-An Antidote For Apixaban and RivaroxabanHabib G. Moutran BarrosoNessuna valutazione finora
- Hemostasis, Surgical Bleeding and TransfusionDocumento10 pagineHemostasis, Surgical Bleeding and TransfusionCarl Earvin L. FavoritoNessuna valutazione finora
- Hemophilia PDFDocumento135 pagineHemophilia PDFJavier Alvarez100% (1)
- Coag Made EasyDocumento15 pagineCoag Made Easygus_lionsNessuna valutazione finora
- Biochemistry A (RKTP, RMT) - Blood ChemistryDocumento10 pagineBiochemistry A (RKTP, RMT) - Blood ChemistryGaelle Lisette MacatangayNessuna valutazione finora
- Chapter 48 - Drugs Affecting Blood CoagulationDocumento12 pagineChapter 48 - Drugs Affecting Blood CoagulationJonathon100% (1)
- Overview of The Coagulation SystemDocumento9 pagineOverview of The Coagulation SystemaksinuNessuna valutazione finora
- Basic Concepts of Hematology (Hemostasis)Documento53 pagineBasic Concepts of Hematology (Hemostasis)Hendra SshNessuna valutazione finora
- Guyton Chapter 36Documento6 pagineGuyton Chapter 36g_komolafe100% (1)
- Hemostasis, Clotting Disorder and AnticoagulantsDocumento87 pagineHemostasis, Clotting Disorder and AnticoagulantsSomit Jain100% (1)
- CoagulationDocumento3 pagineCoagulationHerho-nyl CesNessuna valutazione finora
- Drugs Used in Haematology : Anticoagulants, Antiplatelet Agents and Thrombolytic AgentsDocumento42 pagineDrugs Used in Haematology : Anticoagulants, Antiplatelet Agents and Thrombolytic AgentsIrum RafeeqNessuna valutazione finora
- HemophiliaDocumento60 pagineHemophiliavibhurocksNessuna valutazione finora
- Hemodynamic Disorders-RevisedDocumento118 pagineHemodynamic Disorders-Revisedspringding0% (1)