Documenti di Didattica
Documenti di Professioni
Documenti di Cultura
Saludamay Vol IVNo1Feb2013 Final
Caricato da
crisjavaCopyright
Formati disponibili
Condividi questo documento
Condividi o incorpora il documento
Hai trovato utile questo documento?
Questo contenuto è inappropriato?
Segnala questo documentoCopyright:
Formati disponibili
Saludamay Vol IVNo1Feb2013 Final
Caricato da
crisjavaCopyright:
Formati disponibili
Saludamay Vol. IV No.
1 1
ISSN 2094-6104
Aquinas University of Legazpi Research, Planning and Development (RPD) Rawis, Legazpi City rpd@aq.edu.ph
The Official Research Publication of College of Nursing and Health Sciences Aquinas University of Legazpi (052) 482 0344
Thru the assistance of The Research, Planning and Development (RPD) Volume IV No. I February 2013 Publisher REV. FR. ERNESTO M. ARCEO, OP Editorial Advisers VICENTE B. PERALTA, RN,MSN CHRISTIAN E. RIVERO, JD, MGM Managing Editor HERMOGENA F. CAARES, RN, MAN Lay-Out CHRISTIAN E. RIVERO, JD, MGM SHERWIN F. SEVA
The words published in this volume are the sole responsibility of the authors. Publication does not mean endorsement by the Office of the Vice-Rector for Academic Affairs, Research, Planning and Development (RPD), and Office of the Dean, College of Nursing and Health Sciences. For questions and suggestions, write the editorial advisers care of the College of Nursing and Health Sciences, Aquinas University of Legazpi, Rawis, Legazpi City. Philippine Copyright 2013 By Aquinas University of Legazpi, Inc. ALL RIGHTS RESERVED ISSN 2094-6104
Saludamay Vol. IV No.1 iii
FOREWORD
A person is a behavioral system in which the functioning outcome is the observed behavior. Nursing contributes by facilitating effective behavioral functioning in the patient before, during, and after illness. Nurse Dorothy E. Johnson 1980
The Nursing Process stresses the importance of efficient and effective Assessment to come up with specific Diagnoses that shall serve as basis for Nursing Interventions. The Process includes, among others keen observation and documentation of behaviors of patients so that appropriate nursing actions are implemented. This fourth issue of the Saludamay of the AUL College of Nursing and Health Sciences features the researches of the colleges faculty and students for the last two years. It includes the observations on behaviors which we hope will help in formulating possible interventions for similarly situated situations. This issue is particularly special since the University is now celebrating its 65th Foundation Anniversary. As part of the Dominican University, the College has been steadfast in its role to educate Aquinian Nurses that imparts the mission and thrusts of the University which are: Moral Integrity, Academic Excellence and Emotional Maturity. Also, the fruition of this journal is a result of the collaboration between the College of Nursing and Health Sciences and the Research, Planning and Development Office of the University. We hope that similar endeavors in the future will be as gratifying as this one. We pray that these outputs contribute to the knowledge base of health information in the college, the region, and the nation.
Prof. Vicente B. Peralta, RN, MSN Dean, College of Nursing and Health Sciences
iv aquinas university of legazpi
TABLE OF CONTENTS
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iii Table of Contents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iv A Case Study of Adolescents with Obsessive Compulsive Behavior Manifestations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1 Case Study on Post Traumatic Stress Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . .26 Spirituality: Implication to the End-of-Life Care of Elderly Patients in Harong Kan Sagrada Familia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .47 Knowledge Level on Sexually Transmitted Infection of Nursing Students in Aquinas University of Legazpi. . . . . . . . . . . . . . . . . . . . . . . . . . . .57 Stressors in the Workplace, their Effects to the Faculty Members of Aquinas University of Legazpi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .68 Phenomenology of Male Same-Sex Practices and their Implications on Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .72
A CASE STUDY OF ADOLESCENTS WITH OBSESSIVE COMPULSIVE BEHAVIOR MANIFESTATIONS
Maricar C. Perez Raymond Boris Ll. Salazar Dwayne C. Templado
Abstract
Adolescents face considerable changes and pressures that are among the most complex in the life cycle. These changes and pressures converse in ways that challenge the stability and mental health of many, but not all, adolescents. Obsessive compulsive behaviors become a less observable diagnosis, and are too often left untreated until they are severe which led to an anxiety disorder called Obsessive-Compulsive Disorder. The symptoms of OCD are unwanted, intrusive and repetitive obsessions and compulsions, resulting in a negative impact on quality of life. Individuals often delay for many years before reporting their symptoms to any healthcare professional. This study aimed to assess adolescents with Obsessive-Compulsive Disorder manifestations, as well as their coping mechanisms on the stress and anxiety that the condition presents. It gathered answers and possible solutions to the following problems: 1) What is the socio-demographic profile of the participants in terms of age and status in the family? 2) What are the symptoms manifested by the participants in relation to obsessive-compulsive disorders in terms of obsessive thoughts and compulsive behaviors? 3) What problems are experienced by the participants when obsessive thoughts and compulsive behaviors occur? 4) How do participants cope when obsessive thoughts and compulsive behaviors occur? 5) What measures may be proposed to help the participants minimize the stress and anxiety brought about by their Obsessive-Compulsive Behaviors? This study used qualitative exploratory techniques to seek a deeper reality of the subject. The methods that were used by the researchers were interviewing, journalizing and categorizing. In order to facilitate and obtain an in-depth analysis, the data were examined using a thematic framework. This framework sorted out and organized the data gathered according to concepts, themes and categories.
2 aquinas university of legazpi
Introduction Obsessive compulsive disorder (OCD) is an ever present part of society today. Television shows and media coverage about people with this disorder shed light on a serious illness that plagues people. However, many people are mistaken with what OCD actually is. Knowing OCD facts is important for individuals who think they have this disorder or have friends/family members who do. Some think it is compulsive shopping, some think it is alcoholism and others think it has to do with being a perfectionist. While there might be similarities common with all of these and OCD, they are not the same. Some people who have OCD have both the obsessions and the compulsions. The rest of the people only have one or the other, but not both. Normally, the growth and development of children and adolescents encompasses rituals and obsessive thoughts which usually occur with a purpose and focus based on age. For instance, the mealtimes, bath, and bedtime of the preschool children could be considered as rituals and routines that help them stabilize their expectations and understanding of their world. School-aged children normally develop group rituals as they learn to play games, team sports, and recite rhymes, whereas, older children and teens begin to collect objects and develop hobbies. These rituals actually help children to socialize and learn to master anxiety; however, if rituals and obsessive thoughts occur in excess of the normal limits, it may be considered unusual resorting to obsessive-compulsive disorder (OCD). According to McCann, S. (n.d.), Obsessive Compulsive Disorder (OCD) is a neuro-biological illness, classified as an anxiety disorder, affecting millions. It is a potentially disabling condition that can persist throughout a persons life. The individual who suffers from OCD becomes trapped in a pattern of repetitive thoughts and behaviors that are senseless and distressing but extremely difficult to overcome. OCD occurs in a spectrum from mild to severe, but if severe and left untreated, it can destroy a persons capacity to function at work, at school, or even in the home. Usually adolescents with OCD are aware of the stigma that is associated with the symptoms of the disorder and may look for ways to devise explanations regarding their behaviors or ways to keep away from situations or places that trigger the behaviors, but they tend to hide the signs and symptoms because they fear of being considered as weird or crazy. On the other hand, some parents may not be concerned by the symptoms of OCD at the initial stage wherein compulsive rituals that are appropriate developmentally, or appear healthy are just taken for granted, not knowing that these are dangerous because. It means that the treatment will be done during the time when the behaviors have become very disruptive. In the Philippines, many Filipinos casually use the term obsessive compulsive or OC to describe a very organized and meticulous person. Despite the common use of such term, it must not be confused with the clinical obsessive-compulsive disorder. Fixation on certain things like cleanliness, orderliness and doing things to avoid diseases may not necessarily
Saludamay Vol. IV No.1 3
be traits of OCD. Some people may just be perfectionists or exhibit overly concern about some things. Based on the publication Statistics by Country for Obsessive- Compulsive Disorder by the group Cure Research, it is estimated people in the Philippines are affected by the disorder. However, this figure is merely a projection and not the actual statistics of OCD cases in the country. A lot of individuals still remain undiagnosed because they are not aware of their condition or ashamed of seeking medical help due to fear of being labeled crazy. There are a lot of people with OCD who need help (Yapchiongco, 2010). Given that OCD can bring about extreme distress and disruption for individuals when both socialization and self-actualization are crucial, the researchers aimed to have an in-depth understanding of how adolescents manifest symptoms related to obsessive compulsive behavior, how they cope with stress and anxiety and how would they be able to explore and how these behaviors affect their daily lives. This study is aligned with the Universitys research agenda on enhancing health care and protecting vulnerable groups to provide basis for developing new knowledge based on the actual testimonies of the participants that will contextualize prevailing knowledge. Statement of the Problem This study aimed to have an in-depth understanding of the adolescents with ObsessiveCompulsive Behavior manifestations. Specifically it sought answers to the following questions: 1. What is the socio-demographic profile of the participants in terms of age and status in the family? 2. What symptoms are manifested by the participants in relation to obsessive-compulsive disorders in terms of obsessive thoughts and compulsive behavior? 3. What problems are experienced by the participants when obsessive thoughts and compulsive behaviors occurred? 4. How do participants cope with their obsessive thoughts and compulsive behaviors? 5. What measures may be proposed to help the participants minimize the stress and anxiety brought about by their obsessive-compulsive behaviors? Review of Literature The reviewed literature and studies were found to have bearing on this present study. The literature of Retherford (n.d.) states that Obsessive Compulsive Disorder affects millions of people, including children. Children who suffer from OCD experience recurring rituals and thoughts. These thoughts are unwanted, but the children suffering from this disease cannot control them. They feel an extreme urge to perform certain rituals in order to prevent these thoughts from happening. Completing their rituals will provide for a temporary relief from anxiety for them. For children suffering from OCD, this can be devastating. Children often feel the need to fit in or be like other children around them. Therefore, they tend to hide their obsessions
4 aquinas university of legazpi
from their loved ones for fear of rejection, and because of this, it can be months or even years before a child is properly diagnosed. Similarly, West (2008) stressed that over 6.6 million people (one out of every 40 people) suffer from Obsessive-Compulsive Disorder (OCD). This disorder often begins at times of emotional stress, major life transitions, health problems, and events representing new levels of responsibility. OCD is a very time-consuming disorder and, according to the DSM-IV, it may preoccupy a person for an hour or more a day. According to Owen Kelly, Ph.D.(2010)although symptoms of OCD can begin at almost any age, research suggests that there are two distinct periods when OCD symptoms are most likely to appear. The first occurs around the ages of 10 to 12 or just before puberty and the second is between the ages of 18 to 23. People who develop OCD before puberty are considered to have early onset OCD while those who develop OCD later in life are considered to have late-onset OCD. Interestingly, there may be distinct differences in the symptoms, response to treatment, overlapping illnesses, brain structure and thinking patterns of people with early versus late onset OCD. Winkler (2008) cited in his article that more than 30 percent of adults with OCD have severe symptoms of obsession or compulsions since early childhood (early onset of OCD). Very often the diagnosis is missed because nobody thinks about the possibility of this neurobiological disorder. Kelly (2011) cited in his article that the key symptoms of OCD are compulsions. The compulsions are obsessive behaviors that a person repeats over and over again (often for hours on end) to relieve anxiety. He cited that the common obsessive behaviors among people with OCD include: repeatedly checking to make sure that doors and windows are locked or that appliances are turned off. Some individuals with OCD have to check their neighborhood to make sure they have not hit someone with their car or assaulted someone, cleaning of the house, clothes and/or body, counting objects, letters, words (or just about anything), requesting or demanding reassurance from family members or health care providers (e.g., have I molested someone? my hands should be clean now, right?), repeating phrases or sequences of words either out loud or in ones mind and rearranging objects to ensure a specific order and/or symmetry. Watkins (2009) a medical doctor said, at one time, OCD was believed to be fairly rare. When it was diagnosed, it seemed resistant to treatment. Community surveys of adolescents have suggested that at any given time, 1% to over 3% are experiencing symptoms of OCD. Children as young as 5 or 6 can show full-blown OCD. Between 30% and 50 % of adults with OCD reported that their symptoms started during or before mid-adolescence. Fortunately, there are now more effective treatments for OCD. In many ways the symptoms and treatments of OCD in both children and adults follow the same general principles. However, children differ from adults cognitively, developmentally and physiologically. Because of this, we modify techniques based on the particular stage of childhood or adolescence.
Saludamay Vol. IV No.1 5
Green (n.d.) pointed out that people with Obsessive Behavior are not crazy. They are fully aware of the excessiveness of their behavior and thoughts. In order to lessen obsessive behavior one must first understand it. One who has been in an accident remembers the feeling as the car was sliding into the tree or spinning uncontrollably, Feeling out of control is probably one of the worst feelings in the world, and experiencing that sensation all of the time is an anxiety disorder. However, the severity can be lessened with some help and knowledge. These steps can in no way completely stop obsessive behavior, but they can give you a good start with your determination to self- help. The study of Quinn (2010) noted that obsessive-compulsive personality disorder is marked by perfectionism, rigidity, poor time management, and poor emotional expression. It is not a temporary condition, but it is an ongoing and relatively permanent condition that causes a significant amount of pain and suffering for the individuals that have it. The purpose of her paper is to discuss the general features of the obsessive-compulsive personality disorder, its etiology, comorbidity and differential diagnosis, and gender and cultural issues in regard to prevalence. A general overview of treatment options indicates that individuals with obsessive-compulsive disorder are difficult to treat, but that successful treatment can result in greater self-awareness and an ability to develop skills that will enable them to have more productive and less painful lives. The American Psychiatry Association (2000) cited that in general, individuals with OCPD do not tolerate their own imperfections or the imperfections of others. Their relationships are usually serious in tone and they are very uncomfortable when other people express their emotions. They control their feelings of affection and have difficulty being tender and loving. They are difficult to work with and to live with because of their strict adherence to rules and to small details, and because of their stubbornness. People with OCPD are usually not able to respond appropriately or flexibly when they are confronted with new situations and with a need to compromise. Whereas, Eskedal and Demetri (2006) said people who have OCPD are often considered to be workaholics. They may display a Type A personality that is characterized by their preoccupation with work. They work diligently and tirelessly. They may be competitive, and they also experience stress due to time constraints and time urgency, which leaves them vulnerable to heart disease, such as, myocardial infarction. People with OCPD often sabotage their own efforts because they have a tendency to get caught up in small and irrelevant details, which results in falling behind and not meeting deadlines. The stress and anxiety associated with demands that are difficult or impossible for them to meet usually cause a person with OCPD to suffer emotionally and to seek professional help. As what Kelly (2010) cited in his articlethe unhealthy form of perfectionism has been strongly linked to OCD. Perfectionism appears to be particularly strong if one had a strong need for things to be done just right or require certainty. For example, unhealthy perfectionism tends to be very high if one feels that the compulsions have to be done exactly the right way. In
6 aquinas university of legazpi
these cases, it is not uncommon to believe that if the compulsion is carried out perfectly, a feared outcome, such as death of a loved one, will not take place. Likewise, unhealthy perfectionism tends to be high if the OCD symptoms revolve around checking. Specifically, if one does not feel he has perfect certainty that he has locked the door or turned off the stove, he might return to check these items over and over again. Tied to this is the excessive fear of making a catastrophic mistake, such as leaving the door open all day or burning down the house by leaving the stove on. Ironically, checking over and over again reinforces the idea that one is not perfect or possibly even losing his mind. This can make him feel even worse and less self-confident which, of course, sets him up to do more checking. Finally, unhealthy OCD perfectionism may help to perpetuate obsessions.For instance, like many people with OCD, one might believe that he must have complete control over his thoughts. As such, when a bizarre or distressing thought pops intrusively into his mind, he labels these thoughts as dangerous because they are out of his control. This causes to monitor the thought even more closely, which can help to create an obsession. In the study of Dombeck and Moran (2006) it was pointed out that apart from personality traits, people also tend to develop habitual modes and methods of managing stress and coping with upsetting emotions. By and large, these habitual methods do help people to manage and defuse stressful situations they find themselves in, but they are not all equally efficient at this task. Some work better than others. While some really do succeed in helping people to manage upsetting emotion, the lesser quality methods generally end up causing more problems than they solve. The person with OCPD is so occupied with striving to do a task properly that the person attempts to attain perfection. Such a person may impose all sorts of rules to maintain efficiency, but instead only succeed in making the task more difficult. The person with OCPD puts work before personal relationships or leisure time, and draws a very strict line when it comes to moral or ethical issues (Terwilliger & Williams, 2009). They further noted that the person with obsessive-compulsive is very controlling, and has a feeling of superior competence comparing him or herself to others. He or she will entrust tasks to others only under extreme caution, and has strict instructions as to how they are to be carried out. The person with OCPD will save money and be stringent with it, as money is a fail-safe in case something unavoidably catastrophic occurs. General rigidity and stubbornness is not uncommon: the OCPD patient takes comfort in the way its always been done, does not favor change, and will only relent reluctantly in an argument. Because it is a personality disorder, the person with OCPD is comfortable with their high standards and rigid mindset, seeing it as a virtue even though more often than not it hampers success. The person with OCPD will justify actions instead of admitting any sort of problem, because in the persons mind he or she is right. Edwards (n.d.) stressed that without treatment, the symptoms of OCPD can progress to the point that the sufferers life becomes consumed, inhibiting their ability to keep a job and
Saludamay Vol. IV No.1 7
maintain important relationships. Many people with OCD have thoughts of killing themselves, and about 1% complete suicide. In terms of the prognosis for the specific symptoms, it is rare for any to progress to a physically debilitating level. However, problems like compulsive hand washing can eventually cause skin to become dry and even to break down. Repeated trichotillomania can result in unsightly scabs on the persons scalp. Turcanu (2010) noted that there are many ways to fight against OCD thoughts. They are not easy and will not cure a person of OCD. But by taking conscious steps to fight the invasion of these OCD thoughts, a patient can lower the intensity of the condition and help in treating himself. He said, a simple trick is to develop and image of a big, bold, red stop sign in the mind. Each time OCD thoughts begin to enter the mind, focus on the stop sign and use it as a symbol of your inner strength an ability to fight against these negative OCD thoughts. When negative thoughts begin to enter the mind, try and focus on the positives of life all the good things that are going on or have happened in the past. Keeping a notebook where all the positives of ones life are noted down is good idea. When OCD thoughts begin to emerge, going through this notebook and looking at the reason why one should not fear makes the sense. Joining a support group, being able to share experiences will lighten the load and will able him to learn from the experiences of others in dealing with these negative thoughts. One may also derive strength from knowing that others share the problem. Keep self involved in social activities. The less isolated one is, the better he will be able to fight the OCD thoughts. Tell the family and friends of the problem and ask for their support. Stay away from alcohol or drugs and self medication. These are short term coping mechanisms that will only serve to increase the problem. In the study of Ciarrochiand Deane (2004) it was cited that based on past cross-cultural research, it was hypothesized that people who had strong individualistic values and beliefs within an individualistic culture would have smaller social support networks, lower emotional competence, lower intention to seek help from a variety of sources, and poorer mental health. As detailed, the person with OCPD is so occupied with striving to do a task properly that the person attempts to attain perfection. Such a person may impose all sorts of rules to maintain efficiency, but instead only succeed in making the task more difficult. The person with OCPD puts work before personal relationships or leisure time, and draws a very strict line when it comes to moral or ethical issues. Hoarding with no traceable cause or sentiment was at one time thought to be a key symptom; however these criteria are under review and may be omitted in the next version of the DSM (Claiborne, 2009). Obsessive-Compulsive Behavior is an anxiety disorder which carries a persons ordinary concerns to an extreme. (The American Academy of Child and Adolescent Psychiatry) The disorder is characterized by a series of obsessions, which are reoccurring thoughts, or fears, that constantly persist throughout a single day and which inevitably drive an individual crazy. Compulsions are actions, or thoughts, that the individual performs to briefly relieve their obsessions. Obsessive behavior is characterized by unwanted thoughts that recur repeatedly, do not make
8 aquinas university of legazpi
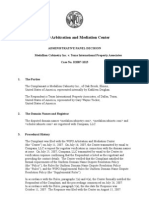
sense, causes fear and doubt, and can distract from important activities, International OCD Foundation (IOCDF). These thoughts can be anxiety provoking or distressing, and will vary depending on the thoughts in the persons consciousness. Compulsive behaviors, or rituals, are the repetition of activities in which a person engages that neutralize, counteract or make obsessions go away, according to the IOCDF. Compulsions can also cause a person to avoid the situation that triggered the excessive behavior, and the repetitive rituals help to reduce the anxiety from the obsessive thoughts (FamilyDoctor.org). Common compulsions on the other hand may include; (a) Repeated bathing, showering, or washing hands (b) refusing to shake hands or touch doorknobs; (c) repeatedly checking things, such as locks or stoves; (d) constant counting, mentally or aloud, while performing routine tasks; (e) constantly arranging things in a certain way; (f) eating foods in a specific order; (g) being stuck on words, images or thoughts, usually disturbing, that wont go away and can interfere with sleep; (h) repeating specific words, phrases, or prayers; (i) needing to perform tasks a certain number of times and (j) collecting or hoarding items with no apparent value. Freudian psychoanalysts view OCD as the result of conflict between the ego and the id; impulses that are repugnant to the ego are controlled by unconscious defense mechanisms. Behaviorists on the other hand, see OCD as a conditioned response to anxiety-provoking events. In a behaviorist point of view, linking anxiety with a neutral object or event causes obsessional preoccupation. Such behavior would therefore help control the patients anxiety and is thought to be helpful (Shieves, 2007). Although the ritual may make the anxiety go away temporarily, the person must perform the ritual again when the obsessive thoughts return. This OCD cycle can progress to the point of taking up hours of the persons day and significantly interfering with normal activities. People with OCD may be aware that their obsessions and compulsions are senseless or unrealistic, but they cannot stop themselves. Conceptual Framework This study anchored on two intersecting theories; (a) Johnsons Behavioral System Model, and (b) Sister Callista Roys Adaptation Model. Johnsons theory defined nursing as an external regulatory force which acts to preserve the organization and integration of the patients behavior at an optimal level under those conditions which the behavior constitutes a threat to physical or social health or in which illness is found. Sister Callista Roys Adaptation Model states that the goal of nursing is the promotion of adaptive response in relation to four adaptive modes (a) physiological-physical; (b) self-concept- group identity role; (c) role function and (d) interdependence. Roys model suggests that nurses seek to identify influencing stimuli and intervention strategies centering on the changing internal and external environment of a person. Using the frameworks of Sister Callista Roys Adaptation Model and Johnsons Behavioral System Model, the researchers examined the adolescents obsessive-compulsive behaviors. It was
Saludamay Vol. IV No.1 9
Adolescents Manifesting Obsessive-Compulsive Behaviors
Johnsons Behavioral System Model
Sister Callista Roys Adaptation Model
Profile of Participants Age Rank number in the family
Symptoms Manifested in relation to common Obsessive-Compulsive Behaviors
Problems Experienced
Coping Mechanisms used
Proposed Measures
Improved Coping Skills/Stress Free Individual
used as a guide to explore the difficulties encountered by the participants and their ways in coping with the stress and anxiety that come with it. It worked on the premise that the participants age, gender and educational attainment are interrelated to other variables. The researchers attempted to know the symptoms manifested by the participants in relation to the different types of Obsessive-Compulsive Disorders, determined the difficulties they met and coping mechanisms used by the participants when exposed and faced with stress and anxiety, which in turn, help the participants minimize the stress and anxiety brought about by their Obsessive-Compulsive behaviors in such a way that their coping mechanisms will improve so that they will become a stress-free individuals.
10 aquinas university of legazpi
Methodology This study used qualitative exploratory and inductive methods in order to seek a deeper truth and have a broader understanding about the adolescents manifesting Obsessive-Compulsive Behavior manifestations. Two participants were recruited through purposive sampling. The goal was to talk to adolescents about their experiences in manifesting symptoms of obsessivecompulsive behavior without assuming what it could mean and how it could play out in different participant contexts. Each participant was interviewed for an average of 1 hour. There was no formal, structured, interview schedule. Instead, each participant began sharing their stories with an initial invitation to share his story about specific experiences in manifesting symptoms related to obsessive compulsive behaviors. Follow-up questions of missing data based on what was shared were done by journalizing. Both participants talked about their different experiences. In gathering relevant data, interview, direct observation (DO), key informant (KI) interview, and journalizing were done. The focus of this study is the adolescents who, although not medically diagnosed with Obsessive-Compulsive Behaviors, are unaware that they are manifesting its symptoms. Interview was conducted personally with each participant on one-on-one basis regarding the subject of the study through in-depth approach. Direct observation was done covertly by observing the participants behavior while being interviewed in order to get the nonverbal cues. Key informant interview was done by getting information from an individual who is considered to be particularly knowledgeable about the topic of interest and who is accessible and has in-depth knowledge about a topic. The semi-structured interview was conducted in a face-to-face setting which permitted the researchers to seek new insights, ask questions, and assess phenomena in different perspectives. In order to cross-validate the information provided by the participants, key informant interview was conducted to members of the family, relatives and friends to rectify biases of the data. All conversations have been recorded with the use of a tape recorder to facilitate the transcription of data and journalizing the results of the interview. Each interview was recorded and transcribed. Eventually, an in-depth analysis and discussion were made by the researchers after all the recorded data have been encoded followed by clustering, categorizing and the matizing approaches. Narratives were analyzed to identify themes and lines of inquiry. The researchers observed the basic ethical principles to protect the human subjects. The prospective participants were informed in writing and in person during the explanation and signing of the informed consent. An informed consent is a pre-requisite for all identifiable subjects which are grounded in the ethical principle of autonomy. Furthermore, participants were treated with dignity and respect thereby upholding the principles of beneficence and justice. Respondents may, however, refuse to participate in and drop out of the study at anytime, before, during or after this study is completed. It is through this that the welfare of the participants was protected.
Saludamay Vol. IV No.1 11
Discussion of Results In-depth interviews conducted with the two participants revealed some recurrent themes as their common point-of-view and experiences. The themes that emerged from discussions seemed to directly correspond to the challenges that participants described. Content analysis of this study was based on the differences between the two participants who came from diverse environments. Based on the categories identified several themes were extracted such as self- image and perfectionism along personality, organizer, compulsion, security and obsession on behavior and acceptance and diversionary activities along coping mechanisms categories. Table 1 shows the summary of categories and themes. Socio-Demographic Profile of the Participants Participant 1 Paul (not his real name) is 19 years old, male and a third year college student presently staying in an apartment rented by his family. He is the eldest among five siblings. Table 1. Summary of Categories and Themes Categories Personality Themes Self Image Perfectionism Organizer Compulsion Security Obsession Acceptance Diversionary activities
Behavior
Coping Mechanisms
Participant 2 Edward (not his real name) is 25 years old, male, a third year college student and a second courser. He is also the eldest among five siblings. Symptoms Manifested by the Participants in Relation to Obsessive-Compulsive Disorders This part of the discussion determines, the symptoms manifested by the participants in relation to obsessive-compulsive disorders. Although the participants were not medically diagnosed with obsessive-compulsive disorders, the possible symptoms were identified based on the storyline of two participants regarding their personality. This study identified three main
12 aquinas university of legazpi
categories such as personality, behavior and coping mechanisms. The analysis of the transcribed interview shows that self image and perfectionism appeared as the themes along the personality. While, in terms of behavior, the themes identified include organizer, compulsion, security, competitiveness, and obsession. Personality Personality is made up of the characteristic patterns of thoughts, feelings and behaviors that make a person unique. While there are many different theories of personality, the first step is to understand exactly what is meant by the term personality. A brief definition would be that personality is made up of the characteristic patterns of thoughts, feelings and behaviors that make a person unique. In addition to this, personality arises from within the individual and remains fairly consistent throughout life (Kendra, 2008). Self Image Basically, self-image is how people see themselves and how they believe others perceive them. If one has a poor opinion of himself or herself, the self-esteem will be low. The way to conceive self is very important as it will affect thinking, mannerism and relationship with others. People will respond positively or negatively depending on how confident one is; confidence depends on the image of self. This description of self-image could be observed to Paul as he perceived himself as straightforward and choosy with whom he wants to be with and an irritable person. He deemed that other people had that impression that he is plastic and moody, as what he stated: For negative aspect, Im frank, I choose people to be with, I identify them first, people think Im plastic and moody. Irritable ako every morning, patterned yun. Taliwas ang isip ko sa ibang tao. Kasi yung ideas di nagja-jibe. Ina-identify and kinikilala ko muna ang mga tao. (I am Irritable every morning, its patterned. My way of thinking is always contrary to other people thinking because their ideas dont jibe with mine. I tried to know them first.) Paul continued describing himself as an individualist, a person who shows independence and individuality in his behavior, opinions, or actions. Palaging taliwas ang isip ko, basta iba yung aspect sa ibangtao yung output or outcome. May pagka individualist din ako.Halimbawa, since high school, pero nung elementary pa talaga. Pag may group project, mas gusto ko gumawa ng mag-isa kasi pag may kasama parang useless.
Saludamay Vol. IV No.1 13
(My ideas are always in contradiction with others on different aspect, output or outcome, for example, since I was in high school and mostly during elementary. Once there is a group project, I want to do it alone, because if I work with someone, it seems useless.) Gusto ko yung idea ko lang. kaya pag may group project, di ko na lang linalabas idea ko.(I chose to have my own idea whenever there is group project. I never shared my idea.) The statements of Paul implied that he displayed strong individualistic values and beliefs of himself where he has lower intentions to seek help from a variety of sources. To cross-validate his statements, the researchers interviewed the sister of Paul who served as the key informant. Anoibang kwarto kasi kami. Kasi yun ano..halimbawa may kainan sa baba, andun lang siya niyan sa taas, gusto niya solo lang siya, nagaaral lang, books lang. kahit nga famiy bonding ayaw niya sumamasige niya ang taram. (We are in a different room. If theres party downstairs, he will just stay upstairs. He preferred to be alone, studying, he just read books, even family bonding, he does not want to go with us. He is always talking.) Uhm. Hindi siya pag tinatanong ni mama, hindi masyado nagsasalita, tahimik lang. Mga dalawang beses mo lang siya marinig magsalita sa isang buwan. (Uhmm, Hes not....When our mom asks him, sometimes hes not responding. Hes just keeps silent. You can only hear him talk maybe twice a month.) The confirmation of the key informant depicts the personality of Paul as individualistic, to the point that he isolates himself. Seemingly, he tries to detach himself from other people. Probably, the affirmation of the key informant that Paul keeps on talking alone is actually a manifestation of his obsessive thoughts that he could not get rid of for wanting not to seek help from others. This could be attributed to the study of CiarrochiJ. & Deane, F. (2004) where it was cited thatbased on past cross-cultural research, it was hypothesized that people who had strong individualistic values and beliefs within an individualistic culture would have smaller social support networks, lower emotional competence, lower intentions to seek help from a variety of sources, and poorer mental health. Likewise, Paul portrayed himself as an independent person. Basically, self-image is the mental picture of how one sees himself. Men and women usually are resistant to change their self-image because it was defined and shaped at an early age. Family and friends too can contribute to a poor self-image of a person.
14 aquinas university of legazpi
Since elementary, wara akong katabang sa paggibo ki project.Naging independent ako. Bako ako mahilig mag seek ki help. Hanggan kaya ko, dai ako naghahagad tabang. (Since elementary, no one helped me in making my project. I became independent. Im not used to seek help, for as long as I could do it, I never sought help.) Since, wara computer kaito an pag gibo ko book report manual up to grade 6. I learned not to cut pictures instead draw. Bako arog ngunyan na mabakal ka na sana chart na may drawing pwede mo na i-cut.(Since there was no computer before, I made my book report manually, up to grade six. I learned not to cut pictures instead draw. Unlike these days that you can buy chart with drawing and you can cut it out.) According to Soto (2008), obsessive-compulsive disorder can be a rough thing for someone to have to face. It can be really hard when a person is not quite sure what is happening. If one does a little fact gathering on OCD, the knowledge base will increase and this will make a person brave and be able to deal with it a lot easier. When Paul was asked if he tried to ask himself why he used to draw instead of cutting pictures he said that he could not answer it clearly and stated that it is kind of a weird feeling only. Di ko siya masagot clearly. Pero feeling weird act lang siya.(I cant answer it clearly. But it seems a weird feeling only.) Most people experience feelings of anxiety before an important event such as major exam, interview appointment and many others. Anxiety, however, is mental disorder that causes people to feel frightened, distressed and uneasy for no apparent reason. Nonetheless, the declaration of Paul for weird feeling seems conflicting to the real feelings he had. Perfectionism More often, perfectionists standards are high beyond reach or reason, straining compulsively toward impossible goals. They tend to set high goals and work hard towards them. However, a high achiever can be satisfied with doing a great job and achieving excellence (or something close), even if their very high goals are not completely met. Once faced with failure they become dysfunctional and depressed, overly defensive when criticized and reluctant to share vulnerable feelings. These characteristics of person with OCD clearly illustrate on Paul when he said: Feeling ko gusto ko mag attract attention sa teacher ko ta kan grade 1 ako, an teacher ko sa Arts when it comes sa drawing and stroking gusto niya legible and clean. An pag grade niya first come first serve. An first na maka pass titawan ki high grade. (I felt, I wanted to attract the attention of my teacher because when I was in Grade 1, my teacher in Artswhen it
Saludamay Vol. IV No.1 15
comes to drawing and stroking, wanted it legible and clean. When she gave grades, its first come first serve. The first one to pass will have high grade.) I see to it na maka pass ako first to attain high grade. Tapos, kapag dai ako naka pass first I felt disappointed and got jealous sa naenot mag pass. Kaya, next time na may project ulit, I see to it na maka recover ako. (I saw to it that, I could be the first one to pass to attain high grade. Then, if I was not able to do it, I felt disappointed and got jealous of the one who passed first. So, the next time there is another project, I would see to it that I could recover.) Deeper analysis of the narrative of Paul actually illustrates his character indirectly of being a perfectionist which could be attributed to what Terwilliger and Williams (2009) stated, that the person with Obsessive-Compulsive Personality Disorder (OCPD) is so occupied with striving to do a task properly that the person attempts to attain perfection. Such a person may impose all sorts of rules to maintain efficiency, but instead only succeed in making the task more difficult. The person with OCPD puts work before personal relationships or leisure time, and draws a very strict line when it comes to moral or ethical issues. It was further noted that the person with obsessive-compulsive is very controlling, and has a feeling of superior competence comparing him or herself to others. He or she will entrust tasks to others only under extreme caution, and have strict instructions as to how they are to be carried out. General rigidity and stubbornness is not uncommon: the OCPD patient takes comfort in the way its always been done does not favor change, and will only relent reluctantly in an argument. Because it is a personality disorder, the person with OCPD is comfortable with their high standards and rigid mindset, seeing it as a virtue even though more often than not it hampers success. The person with OCPD will justify actions instead of admitting any sort of problem, because in the persons mind he or she is right. On the contrary of what Paul said concerning his negative personality, he stressed that he is approachable. However, his statement is somewhat conditional indicative of being choosy. Approachable naman ako. Basta yung taong mag aaproach sayo ay willing talaga, hindi yung napilitan lang or may kailangan lang sayo. Tapos yun lang Masaya akong tao. I have lots of friends, I have circle of friends. (I am also approachable, for as long as the person who will approach me is willing and not forced or only needs something from me. Thats all! I am a happy person. I have lots of friends. I have a circle of friends.) In the case of Edward, he outspokenly admitted that he is a perfectionist from this, for having statements: Negative muna. Ano ako perfectionist, habo ko lang kang bagay na gari maraot, gusto ko pirmi maray. Ta siyempre kung involve na ang sarong tawo, lalo na kung ako involve na sa sarong bagay gusto ko pirming maray. Lalo na pag abot sa academic.
16 aquinas university of legazpi
(Ill start with the negative first, I am a perfectionist. I just do not like bad things. I prefer things to be always good. Of course, when a person is involved, especially if I am already involved in one thing, I want it always right, especially when it comes to academics.) From the narratives of Paul and Edward on how they perceived themselves, it could be seen that their personality can be analyzed in terms of elements or aspects. Its specific articulation reflects the idea that people may have seen them differently from how they viewed themselves. For example, Paul said that other people think he is plastic and moody but he believes otherwise or it is not true. He believes that he has different ideas from other people and that is why he used to identify and know well first other people, Edward wants everything to be in place. As what Kelly (2010) cited in his article the unhealthy form of perfectionism has been strongly linked to OCD. Perfectionism appears to be particularly strong if one had a strong need for things to be done just right or require certainty. For example, unhealthy perfectionism tends to be very high if one feels that the compulsions have to be done exactly the right way. In these cases, it is not uncommon to believe that if the compulsion is carried out perfectly, a feared outcome, such as death of a loved one, will not take place. Likewise, unhealthy perfectionism tends to be high if your OCD symptoms revolve around checking. Specifically, if you do not feel you have perfect certainty that you have locked the door or turned off the stove, you might return to check these items over and over again. Tied to this is the excessive fear of making a catastrophic mistake, such as leaving the door open all day or burning down the house by leaving the stove on. Ironically, checking over and over again reinforces the idea that one is not perfect or possibly even losing ones mind. This can make one feel even worse and less self-confident which, of course, sets one up to do more checking. Finally, unhealthy OCD perfectionism may help to perpetuate obsessions. For instance, like many people with OCD, one might believe that he must have complete control over his thoughts. As such, when a bizarre or distressing thought pops intrusively into his mind, he labels these thoughts as dangerous because they are out of his control. This causes to monitor the thought even more closely, which can help to create an obsession. Behavior Behavior is the manner of acting whether good or bad. This case study depicts how the two participants manifest behaviors typical to a person with obsessive-compulsive behaviors such as organizer, compulsion, security and obsession. As an organizer, Paul stated that he is fond of arranging miniatures on their divider since he was seven years old. Once he observed that somebody moved the miniatures he got irritated but just kept silent and then arranged them in place again.
Saludamay Vol. IV No.1 17
Mahilig ako mag-arrange sa divider miarranging mga tao-tao. Kapag nahihiro, naiinis ako. Pero dai lang ako umiimik inaayos ko na lang.(Im fond of arranging miniatures in our divider then, once they were moved, I got irritated but I just kept silent and return it in place.) Gare nag evolved an sako. Natuto akong magpuyat. Ginigibo ko an paglinis na 11:00 p.m. (It seems it evolved on me. I learned to sleep late at night. I did the cleaning at 11: pm.) Paul further elucidated the reason why he shifted cleaning from the morning to late at night as shown in his statement: Pigdadagitan ako kapag nahiling ninda na naglilinis ako. Saka, para wara disturbance and maka work ako efficiently ta may klase ako na aga. (I am reprimanded when they see me cleaning. And so that there will be no disturbance, and so, I can work efficiently, since I have classes the next morning.) Through analysis of the narratives of Paul it could be deduced that his action is extraordinary and not typical of a normal behavior since it has evolved from childhood till his adolescence period. In such case, Paul is deemed to be an organizer more than normal limits. In the same way, ritualistic behaviors could be viewed as normal but once it becomes repetitious for a longer period of time and continuously lingers in the mind of an individual, it could be considered compulsion. Compulsion is one of the symptoms of obsessive-compulsive behavior. This is true to Paul having stressed that it all started during his childhood days till the present time. Similarly, in the case of Edward, he also manifests an organizers characteristic and as a perfectionist by showing obsessive thoughts and compulsive behavior such as checking door and cabinet locks, and fixing his bed everyday that could not be impeded. When asked if he has ritualistic behaviors he confirmed it by stating: Igwa po! Pagkaaga, inaayos ko an higdaan ko. Gusto ko maayos and bako gusot. Before ako mapa school pigchecheck ko an cabinet ko na maayos and naka lock, mga 3-4 times. (Yes I have! In the morning, I used to fix my bed. I want it well fixed and not wrinkled. Before I go to school I often check my cabinet 3-4 times,to be sure it is well fixed and safely locked.) Gusto ko an mga personal kong gamit like deodorant and perfumes inaayos ko before ako mag pa school. Kapag banngi na, before ako magturog pigchecheck ko an mga lock kan pinto. Minsan pati grills pig sishake ko para maka siguro na dai kami mahabasan. (smiling)... Saro pa, sa paglaba, iabot ako ki 2-3 hours lalo na pag puti ta gusto ko talaga malinis. (I want all my personal belongings like deodorant and perfumes
18 aquinas university of legazpi
are well fixed before I go to school. At night, before I go to sleep, I wonder check all the door locks. Sometimes I wonder to shake the grills to ensure that no intruders can barge in. (smiling...) One more thing, in washing clothes, it takes me 2-3 hours especially if it is white for I want it very clean.) The acceptance of Edward of being a perfectionist was substantiated by all his statements regarding his ritualistic behaviors. He claimed that it is normal to him since childhood but as he gets matured, the more that he enhanced it. Dai po, natural ko na po an. Since aki pa ako arog na ako kaini pero kan nag matured na ako mas lalo ko pa pig enhance. (No, its natural to me. Since I was a child, I am like this but when I became matured the more that I enhanced it.) Satisfied po ako sa piggigibo ko kase kapag dai ko nagibo gare may kulang sa sadiri ko na dai ko nagibo sa arog kaining aldaw. Ngunian na matured na ako mas lalo kong piggigibo pati na an pag shake kan grills na dati ko man dai pig gigibo kan sadit pa ako. (I am satisfied of what I am doing because if I could not do it, as if something is missing on that particular day.) Kelly (2011)stated that the key symptoms of OCD are compulsions. The compulsions are obsessive behaviors that a person repeats over and over again (often for hours on end) to relieve anxiety. He cited that the common obsessive behaviors among people with OCD include: repeatedly checking to make sure that doors and windows are locked or that appliances are turned off. Some individuals with OCD have to check even their neighborhood to make sure they have not hit someone with their car or assaulted someone, cleaning of the house, clothes and/or body, counting objects, letters, words (or just about anything), requesting or demanding reassurance from family members or health care providers (e.g., have I molested someone? my hands should be clean now, right?), repeating phrases or sequences of words either out loud or in ones mind and rearranging objects to ensure a specific order and/or symmetry. Most of these traits of obsessive-compulsive behavior described by Kelly could be observed in Edward and probably could be construed that he manifests symptoms related to obsessive compulsive disorder. Problems Experienced by the Participants Given the fact that obsessive compulsive behavior is considered an anxiety disorder which consists of undesired, troubling thoughts and/or of seemingly irresistible desires to repeat certain actions, it could be construed that the ritualistic behaviors of Paul and Edward are in themselves problems that they encountered. The irresistible obsessive thoughts that led them to perform compulsive behaviors were actually their biggest problem. Based on their narratives, it is apparent that Paul had difficulty in choosing the best among his friends, having statement as:
Saludamay Vol. IV No.1 19
May mga close friends ako, pero bako best friends. (I have close friends but not best friends.) Kasi ang iniisip ko, first of all. Ano ang meron sa iba mong friends na wala sa bestfriend mo? Kasi ang bestfriend mo, one day pwede mo siya maging enemy (What I have in mind is that... first of all, what do some of your friends possess that could not be found in your best friend? And that one day your best friend might become your enemy.) Paul also shared his feeling of anxiety. He said that being away from their parents is a very stressful situation for him. At present, naka istar kami sa apartment na magturugang, si papa and mama nag taga bisita na sana samo. (At present, my brood and I are staying in an apartment. My father and mother are just visits us.) Nasa Sta. Magdalena, Sorsogon, duman sinda nagtatrabaho. Pigtataga bisita na sana ninda kami. Dati si papa pirmi man kami nagduduman samo para magbisita ngunian si mama na sana. (They are in Sta. Magdalena, Sorsogon, they are working there. They just visit us. Before, my father used to visit us but now its only my mother.) Dati kaya, nagkiklinik siya sa Diabetes Clinic sa my Gaisano. Poon kan wara na, dai na siya nagduduman samo ta bisihunon siya sa work niya. (Previously, hes having clinic duty at the Diabetic Clinic at Gaisano. When it was stopped, he cannot visit us anymore because hes too busy with his work.) The situation of Paul implied that being the eldest in the family and apart from their parents greatly affects him in taking the responsibilities of his parents which probably causes him anxiety. On the other hand, Edward seems to have difficulty in accepting himself having an extreme ritualistic behavior by repetitively stressing that what he is doing is just normal for him. With such an act, it shows that he tries to suppress the reality. Ganun talaga ako. Pag may nailing ako, minsan nalilingawan ko ang su tigagibo ko. Medyo arog talaga ako kaini. Ipabayaan ko na lugod su tiga gibo ko, maski dapat tawan mo ki priority. (Thats the real me. Sometimes, when I see something, I tend to forget what I am doing. I am indeed like this. I leave the things that I am doing eventhough they need to be prioritized.) Another situation found to be a problem experienced by Edward is his inability to adjust himself to the decisions of others. His actuation of not conforming to the decision of his group-
20 aquinas university of legazpi
mates indicates superiority complex. As what he cited: So, kunwari may group project, ang gusto ko lang minsan pag nakakailing ako ki para sako negative na sinasabi kang ibang tawo na bako maray para sako, tiga supla ko agad. Mahilig ako magbara. Arog kaini, tiga sabihan ko agad, an mga magiging advantage and disadvantage kaiyan. Minsan masyado akong nag iinsist. (So, for instance theres a group project. Sometimes, if I see something negative on what others had said which is not good for me, I suddenly seized them. I am fond of striking back, like I will immediately tell them of the advantage and the disadvantage of it. Sometimes, Im too insistent.) As confirmation on the description of Edward, the key informant described him as an illhumored person. So, digdi sa classroom mkarawun siya sa mga kaklase.. Dai man siya napipikon, siya ang namimikon. (So, in our classroom, he is very naughty to our classmates. He is not short-tempered instead, he annoys others.) The manifestations of Paul and Edward are significant enough to deduce that both of them displayed some symptoms of obsessive-compulsive behavior. The extreme ritualistic behaviors themselves provide them problems. Coping Mechanisms In actuality, the ritualistic behaviors in obsessive-compulsive are already considered coping mechanism. A person who has this disorder attempts to perform rituals in order to counteract their anxiety. These ritualistic behaviors are both common to Paul and Edward such that when they were asked what other coping mechanisms they used in times of their anxiety, Paul said that he copes within his anxiety by just being passive and viewing movie marathon. Pipabayaan ko na sana ta inisip ko na mawawara na lang siya ta aram ko na makukua ko man an muya ko next timepatiently waiting ako hangang maging orderly an schedule ninda. (I tend to be passive with the thought that it will just vanish for I know I can just get what I wanted next time. I am patiently waiting till their schedule becomes orderly.) Saro pa, nanonod ako ki movie marathon. (One more thing, I viewed movie marathon.) Ako sa trabaho sometimes, lalo na pag arog kaiyan pag kunwari exam tomorrow dipisilun ang mag adal lalo na pagsarabay sabay ang exam, ta cramming talaga.
Saludamay Vol. IV No.1 21
Minsan ma sacrifice ka na lang ki mga subjects na kaipuhan o importante talaga. Kaya minsan nagiging ugakun din pag may trabaho. (Sometimes in my work, particularly if there is an exam the following day, its too hard to study especially if loaded with exams. I find myself cramming. Sometimes, you have to sacrifice other subjects needed or with utmost importance. Thats why I also felt lazy when I have work.) Given the fact that Edward, displayed ritualistic behaviors based on his testimonies he sees to it that he will do everything that comes in his mind to make sure that he is able to do it. Para mawara an doubt ko, gigibuhon ko talaga an dapat na inisip ko para ma sure ko na nagibo ko. (In order that my doubt will be driven away, I really have to do whats in my mind to make sure that I have it done.) Another coping mechanism utilized by Edward to strike-out his stress is by voicing-out what he really felt. Iyo po! Kapag kami my group work sa classroom and dai ko nagustuhan an pinaghururunan, ta na stress ako, mina voice out ako. Gusto ko an decision ko an masunod. (Yes! Once we have groupwork in the classroom and I dont like what transpired since I am stressed, I voiced it out. I want my decision to prevail.) In the study of Dombeck and Moran (2006) it was pointed out, that apart from personality traits, people also tend to develop habitual modes and methods of managing stress and coping with upsetting emotions. By and large, these habitual methods do help people to manage and defuse stressful situations they find themselves in, but they are not all equally efficient at this task. Some work better than others. While some really do succeed in helping people to manage upsetting emotion, the lesser quality methods generally end up causing more problems than they solve. Measures Proposed Many common symptoms in obsessive compulsive disorder appear to reflect a high need for control and may be understood as attempts to establish control. In order to manage the overwhelming urges of the participants the following may be helpful in controlling their inevitable urges by engaging in other activities such as going for a walk, seeking social support by calling friends, making distraction such as watching television and breathing retraining and relaxation exercise. If these measures are ineffective contacting a therapist is necessary. Involvement of family members in controlling the obsessive thoughts and compulsive behaviors of their child is of utmost importance. For many therapists and other mental health pro-
22 aquinas university of legazpi
fessionals, the symptoms of obsessive compulsive disorder are fairly clear. But for parents of children who suffer from related difficulties, it is not always a straightforward matter to distinguish between positive and unhelpful behaviors, and sometimes parents efforts to help their children can have the opposite effect. Validating the behaviors associated with OCD is a common, and often unintentional, result of parents reactions to their childrens symptoms. But through consultation with a mental health professional and a better understanding of how OCD tends to work, parents can provide the care they seek to bestow upon their children without worsening the symptoms. It is also important to assess the overall context of the childs personality, functioning, and developmental adaptation to his or her family, school, and social environment. A careful developmental history is necessary to identify areas of delay or difficulty. The presence of depression, anxiety, perfectionism, irritability, impulsivity, aggression, eating or body image concerns, or psychotic symptoms and their relationship to the obsessions and compulsions should be assessed. Family history of OCD and related anxiety disorders should be elicited, as these disorders are often familial. The childs school performance should be assessed to determine if compulsive re-reading or re-writing; pathological perfectionism; co-morbid anxiety, attention and impulse problems; or associated cognitive impairments have an adverse impact. That a concrete program for individual with OCD be created to be have a support system for these individual during the periods of the obsession and their compulsion. Most importantly, the school should establish specific program on how to deal with students manifesting obsessive-compulsive behavior particularly the Students Development Service. It must contain strategies on preventive measures on how to cope and overcome their anxiety in order not to worsen their misdiagnosed situation. Implications Obsessive compulsive disorder is a relatively common disorder that can cause severe disruption and distress which can be treated effectively in several ways using exposure and response prevention. Less severe cases can be treated using a wide range of interventions. This study found that the participants manifest symptoms of obsessive compulsive behavior and are unaware with the difficult situations they are into and cope with them through various ways; such as behavioral, physical and emotional. However, they are unaware that implications on their quality of life may complicate in the long run if they remain untreated. This poses a major problem not only to the participants but their families as well. Conclusions Based on the content analysis applied in this study, it could be concluded that the two participants manifest symptoms of obsessive compulsive behaviors. Although both of them were undiagnosed of having obsessive compulsive behavior their personality is indicative of an indi-
Saludamay Vol. IV No.1 23
vidual having OCD which has a negative impact on several domains in both the participants. The presentation of their manifestations is affected by socio-cultural factors that are subject to rapid changes and instability in the current time. Hence, it is essential that both the participants should seek professional therapy to confirm whether or not they are indeed exhibiting maladaptive behaviors relative to obsessive- compulsive disorder for their own prevention and significant others. Recommendations Based on the conclusions reached through this thesis, the following recommendations are forwarded Educate the family and friends about the condition in order to help them to manage behavioral problems more sympathetically, and watch out for the warning signs. Parents who note signs of severe anxiety or obsessive or compulsive behaviors in their child or teen show help by seeking an early evaluation and treatment to prevent future problems. Family members particularly the parents should get involve and provide extra time to know the problems of their children by initiating an open communication. Support groups may also be helpful in accepting and changing Obsessive-Compulsive behaviors. Relaxation, meditation, physical exercise, regular sleep, and a balanced diet should be provided in maintaining this focus. Keep a diary to help identify those stressful situations that help to trigger compulsive reactions, enabling them to focus on more constructive activities.
24 aquinas university of legazpi
REFERENCES Watkins, C.E. (2009).Obsessive-compulsive disorder in children and adolescents. Retrieved fromhttp://www.healthyplace.com/anxiety-panic/ocd-center/obsessive-compulsive-disorder-in-children-and-adolescents/ CiarrochiJ. & Deane, F. (2004). Disadvantages of being an individualist in an individualistic culture: Idiocentrism, emotional competence, stress, and mentalhealth. Retrieved from www. ingentaconnect.com/ content/tandf/taps/2004/00000039/00000002/ Terwilliger D. & Williams M. (2009.).Obsessive compulsive personality. Retrieved from http:// www.brainphysics.com/oc-personality.phpDanicasuan (n.d.). How to overcome obsessive compulsive disorder. Retrieved from www.articlesnatch.com/Article/...Obsessive-Compulsive-Disorder/ 3110293 Dombeck M. & Moran P. (2006). Coping strategies and defense mechanisms: Basic and intermediate defenses. Retrieved from http://www.mentalhelp.net/poc/ Eskedal, G. & Demetri, J. (2006).Etiology and treatment of cluster c personality disorders.Retrieved from www.biomedsearch.com/ article/Etiology-treatment-Cluster-C Green T. (n.d.). How to stop obsessive behavior. Retrieved from http://www.ehow.com/ how_2192830_stop-obsessive-behavior.html Kelly G. (2010).OCD and perfectionism.Retrieved from http://ocd.about.com/od/causes/a/ Ocd-And-Perfectionism.htm Winkler, M. (2008).Age of onset of obsessive compulsive disorder (OCD). Retrieved from http:// web4health.info/en/answers/anx-ocd-onset.htmobsessive Kelly, O. Ph.D. 2010 Early versus late onset ocd. Retrieved from http://ocd.about.com/od/ whatisocd/a/Onset.htm Quinn, M. K. (2010). Obsessive-compulsive personality: Painful perfectionism. Retrieved from Disorderhttp://voices.yahoo.com/obsessive-compulsive-personality-disorder-6012138. html?cat=5
Saludamay Vol. IV No.1 25
Retherford E. (n.d.). What are the symptoms of childhood OCD? Retrieved from http://www. ehow.com/about_5085057_childhood-ocd-symptoms.html Edwards, R. (n.d.). Obsessive compulsive disorder (OCD).Retrieved from http://www.medicinenet.com/obsessive_compulsive_ disorder_ocd/page3.htm McCann, S. (n.d.). What is obsessive compulsive disorder? Retrieved from http://www.anonymousone.com/faq119.htm Soto, D. J. (2008). Obsessive Compulsive Behavior- Beat Obsessions with this planwww.zimbio. com/Obsessive-compulsive+disorder/articles/55/ Turcanu, G. (2010). Coping with ocd thoughts. Retrieved from www.zimbio. com/Obsessive-compulsive+disorder/articles/Dikt7ZMwheN/view_doc. php?type=doc&id=9791&cn=353 West, J. (2008). Obsessive compulsive disorder: signs and symptoms. Retrieved from http:// www.totallifecounseling.com/2008/07/obsessive-compulsive-disorder-signs-and-symptoms/ Yapchiongco G. K. (2010). Obsessive-compulsive disorder: Are you oc?Retrieved from www. thepoc.net/thepoc-features/health-and-wellness/
26 aquinas university of legazpi
CASE STUDY ON POST TRAUMATIC STRESS DISORDER
Bryan James G. Carillo
Abstract
Human behavior is one of the factors that defines the distinct individuality of a person. One of the indications substantiating mans existence here on earth is the fact that his nature predisposes him to be superior from all other dwelling mammals, including the fact that behavior plays a key role in his survival. Human behavior is one facet in his being that helps him decide the outcome of his life. The mere logical decisions that span from years of conscious thinking would determine the probable paths he will undertake in life. A mere deviation from this systematic guide would send anyone spiraling out of control. The fact that the environment easily affects human behavior would put man at great risk of experiencing psychosocial disturbances. This is the substance of the research, a study on a particular disorder in the behavior and psyche where the person experiences a traumatic life experience that shatters the core of his being and predisposes himself into a series of disorders that affects her social interactions. This research specifically aimed to answer the following questions: the demographic profile of the client including age and activities of daily living, the predisposing events that led to the development of Post- Traumatic Stress Disorder, the existing coping mechanisms used by the client and suggested nursing interventions to help the participant become a functional individual. The research utilized a comprehensive and extensive examination of data which includes direct observation, interview, a four day immersion, and voice recordings from the interview, asthis provides a most veracious account of the patients profile. A detailed account of a person experiencing Post Traumatic Stress Disorder (PTSD) due to a traumatic event which involves parental separation, culture shock and rape, and having to suffer lockjaw from the struggle with the rapist, is presented in the study.
Saludamay Vol. IV No.1 27
Introduction Envisioning the state of mind of a person was once a far-flung dream of man. The interest that clings to the study of human behavior was full of eccentricities then that most who would delve in the subject oftentimes give up on it. Still, the lure of human behavior can never be disregarded as more and more would seek to understand the undertakings one has to undergo to develop that kind of personality, and ultimately, the individuality. This proclivity for human behavior has brought this research to consider this behavioral condition as topic for research; Post Traumatic Stress Disorder (PTSD). The situation that presents to a person who suffers from Post Traumatic Stress Disorder has complex physical and psychological alterations that would manifest after experiencing a very traumatic event, to the extent that their relationship with their family and the society is devastated (American Psychology Association (2009)). The worldwide statistics that revolve around those who suffer from Post Traumatic Stress Disorder are quite staggering, with the results from countries who are poorly developed to have a higher account of experiencing stress related symptoms. Whats good with the Filipinos are their inherent resiliency that makes them adapt to various stresses in life as quoted by Dr. Evy Sarmiento of Department of Health, Mental Health Department Coordinator. But this doesnt mean they are immune to developing Post Traumatic Stress Disorder. The Philippines has a prevalence of 1,648,738 in an extrapolated statistic done to an estimated population of 86,241,697(US Census Bureau, Population Estimates, (2004) and US Census Bureau, International Data Base, (2004.) This research is in line with the Aquinas University Research Agenda which is enhancing health care. The researchs purpose is to provide an in-depth account of the life lived and being lived by an individual who suffers from PTSD. Furthermore, this study suggested methods on how the person will cope with her present mental condition. The effectiveness of this research depended on various factors that were strictly observed since it is a rather sensitive case and required the complete privacy of the respondents profile. Eventually, this in-depth exploration would supplement the researchers knowledge about Post Traumatic Stress Disorder and would help appreciate the overwhelming duties a nurse should do for a person aggrieved by this malady. Statement of the Problem An in-depth account of a patient who is recently suffering from a post-traumatic stress disorder due to a trauma she experienced is presented in this study. Specifically, the research sought answers to the following questions: 1) What is the profile of the patient in terms of: age, and activities of daily living? 2) What are the predisposing events that led to the development of Post Traumatic Stress
28 aquinas university of legazpi
Disorder to the participant? 3) What are the existing coping mechanisms utilized by the patient? 4) What nursing interventions may be proposed to effectively support the participant in becoming a well-adapted and functional individual? Review of Literature What strikes most is the fact that most of those who suffer from Post traumatic Stress Disorder (PTSD) are females (Kimerling, R., et al, 2002). We could never deny the fact that rape or abuse is a life threatening event to almost all person, but that women are most prone to develop PTSD requires us the need to delve deeper into what Post traumatic stress disorder really is. Post-traumatic stress disorder is virtually defined as an event that is life threatening that severely compromises the emotional well-being of an individual. This form of anxiety disorder is developed after exposure to that psychologically traumatic event (American Psychiatric Association, 2000) Being classified as an anxiety disorder, it is characterized by aversive, anxietyrelated experiences, behaviors and physiologic responses that develop after exposure to either physical or psychological trauma such as rape, war terrorist attacks or to its less likely causes which are trauma caused by natural disasters (Atkinson et al, 2000). One of the debilitating effects of PTSD is that it severely affects the daily functioning of the person. Daily activities that spans from basic household cleaning to the more complex faade of life like socialization and communication are greatly affected because of the reoccurrence of troubling memories and experiences that hinders normal functioning (Field 2005). According to the American Psychology Association, (2000) the severity and duration of the trauma and the proximity of the person to the event are the most important factors affecting the likelihood of developing PTSD. Some of the reasons that triggers the development of PTSD are: the experience of witnessing a person suffering from severe accident or has encountered physical injury, receiving a life threatening medical diagnosis, being a victim of kidnapping or torture, exposure to war combat or to a natural disaster, exposure to other disasters like plane crash or terrorist attacks, being the victim of rape, mugging, robbery or assault, enduring physical, sexual, emotional or other forms of abuse, involvement in civil conflict, and events that may not qualify as traumatic but can be a devastating life event like divorce or unemployment. PTSD sufferers exhibits three cluster of symptoms which include the re-experiencing of the traumatic event in some way, the tendency to avoid places, people or other things that remind them of the event (avoidance) and the exquisite sensitivity to normal life experiences (hyperarousal). The recurrent reliving of the trauma (troublesome memories, flashbacks that are usually caused by the reminders of the traumatic events, recurring nightmares about the trauma, and dissociative reliving of the trauma is the first that plague the patient and would usually occur in the first week after trauma. Avoidance to the point of having phobia of places, people and experiences that remind the sufferer of the trauma or general numbing of emotional responsive-
Saludamay Vol. IV No.1 29
ness and chronic physical signs of hyperarousal, including sleep pattern disturbances, trouble in concentrating and focusing on matters at hand, irritability, anger, blackouts or difficulty in remembering what just happened, an increased tendency and reaction to being startled and hypervigillance (excessive watchfulness to threat). The emotional numbing of PTSD may manifest as lack of interest in activity that was used to be enjoyed (anhedonia), emotional deadness, distancing oneself from people and a sense of shortened future which stems from the fear that they could not resolve. Children and adults may develop PTSD symptoms by experiencing bullying or mobbing, though there is no evidence that susceptibility to PTSD is hereditary. Models done for research about PTSD has found that childhood trauma, chronic adversity and familial stressors increase risk for PTSD, as well as risk for biological markers of risk for PTSD after a traumatic event in adulthood. Studies have also observed that women are likely to develop PTSD than men. Also, children who have seen parent killed or endured sexual assault or abuse to develop PTSD and more than one-third of youths who are exposed to community vigilance (shooting, stabbing or assault) will suffer from the disorder. Persons who are at risk of developing PTSD also has a higher risk of abusing cigarettes, alcohol and marijuana. Almost all aspects of a persons life would be affected by this disorder. One of the most devastating aspects is when a pregnant mother has PTSD. Symptoms would include having emotional problems, poor health behaviors, and memory problems. Women who were sexually abused at earlier ages are more likely to develop complex PTSD and borderline personality disorder. Babies who were born to mothers who suffer from PTSD during pregnancy are more likely to experience a change in at least one of chemical in their body that predisposes the baby to develop PTSD later in life. Globally, the occurrence of PTSD has been observed to be higher in African Americans, Hispanics and Native Americans compared to Caucasians in the US. This is due to the fact that higher rates of dissociation soon before and after the traumatic event (peritraumatic). Also, most individuals in minority ethnic groups tend to blame themselves. They have less social support, increased perception of racism, as well as difference between how ethnic group express distress. There are three areas of the brain that is affected by PTSD: prefrontal cortex, amygdala and the hippocampus. The researcher would like to stress out the part of the brain which is the amygdala and hippocampus. The amygdala is strongly involved in the formation of memories (emotional) especially fear-related memories. People exposed to some stressors have smaller hippocampus; this is significant in understanding the effects of trauma in general, specifically since the hippocampus is the part of the brain that is thought to have an important role in developing new memories about life events. Assessment of PTSD can be difficult for practitioners to make since sufferers often come to complain symptoms other than anxiety associated with traumatic experiences. Other symptoms that they tend to include in their complaints are body symptoms (somatization), depression, or
30 aquinas university of legazpi
drug addiction. Diagnosis is through the use of Diagnostic and Statistical Manual of Mental Disorders IV (Text Revision) DSM-IV-TR. Treatments for PTSD usually include psychological and medical interventions. Most often, providing information about the illness, helping the individual manage the trauma by talking about it directly, teaching the person ways to manage symptoms of PTSD, and the exploration and modification of inaccurate ways of thinking about the trauma has been found to effectively alleviate the symptoms. Specifically, helping sufferers learn how to manage their anger and anxiety, improve their communication skills, and use breathing and other relaxation techniques can help individuals with PTSD gain a sense of mastery over their emotional and physical symptoms. According to Videbeck (2011) 16% of the parents with children affected by PTSD sought help and that 20% sought help for themselves. Suggested ways for coping with PTSD includes learning to talk to friends, family, professionals and PTSD survivors for support. Through this, the person can reduce stress through relaxation technique (breathing pattern and positive imagery), this would secure the active participation in treatments recommended by professionals. Also, increasing positive lifestyle process (exercising healthy eating, distracting oneself through keeping a healthy work schedule if employed, volunteering whether employed or not) and minimizing negative lifestyle practices like substance abuse, social isolation, working to excess, self destructive and suicidal behaviors greatly increases the social interaction of the person with PTSD. Conceptual Framework Alterations in Human behavior can be difficult to handle since one assumes the role of a support structure to the patient who is devoid of it. The fact that almost all who suffer PTSD have compromised ability to cope with their anxiety proves that it is imperative that the needed care to promote eventual independence is provided. Hildegard Peplaus Interpersonal Relations Theory describes a four phase phenomenon known as the nurse-patient interaction. This proved to be a valuable approach to clients who are mentally ill since it primarily addresses the functional needs of the client which is support, open communication, and a sense of being gratified. In this theory, the patient is accepted unconditionally, which is the backbone in approaching all PTSD clients. There is also recognition of and response to the patients readiness for growth, as his initiative, and power in the relationships shift to the patient, as the patient is able to delay gratification and to invest in goal achievement (Stuart and Laraia, 2005). Peplaus theory comprised of four distinct phases which are guided by principles that is best suited for PTSD patients. As stated earlier, Interpersonal Relations Theory seeks to provide what is missing in a person a sense of support, open communication, and gratification. The four phases start with the orientation phase , but before that, one must assess the participant. Data
Saludamay Vol. IV No.1 31
collection and continuous analysis should be done to create an evolving plan of care that would meet the needs of the participant. Orientation phase, otherwise known as problem defining phase, is the first phase of the interrelationship, and it starts when the client meets the nurse as a stranger. At this phase, the nurse defines the problem and decides what mode of therapy will be used for the participant. After the nurse has established trust and rapport, and has been considered as a significant others in the patients life, the participant will try to seek assistance, convey needs, ask questions, share preconceptions and expectations of experiences while the nurse will respond, explain roles to participant, help identify problems and use available resources and services. There are various factors that affect the Orientation Phase, significant of which are values and beliefs, expectations and preconceived ideas. Identification phase is the next step in the process. It deals with the selection of appropriate professional assistance. In this stage, the patient begins to develop a sense of belongingness and a capability to deal with the problem, which decreases the feeling of helplessness and hopelessness. Exploitation phase occurs when the participant feels as if she is an integral part of the helping environment. The use of professional assistance for problem solving alternatives is utilized based on the needs and interests of the patient. Interview techniques were utilized in this phase as it provided a means for exploring, understanding and adequately dealing with the underlying problem. The nurse aids the patient in exploiting all avenues of help, and progress is made towards the final step which is the Resolution Phase. The last phase is described succinctly as the termination of the professional relationship. The patients needs are already met through the collaborative effort of the participant and the nurse. Dissolving the therapeutic relationship may sometimes be difficult for both the participant and the nurse as there persist a psychological dependence. But if everything goes as planned, the patient drifts away and breaks bond with the nurse and healthier emotional balance is demonstrated and both becomes mature individuals. Peplau regarded nursing as a significant therapeutic interpersonal process, and that the physiologic demands and interpersonal conditions of the patient who is mentally ill were addressed through this. She also considered health as a word that symbolizes movement of the personality and other ongoing human processes that directs the person towards creative, constructive, productive, and community living; that the verifiable importance this hold to a person and of maintaining it is the foundation of a healthy mind. Another theory that proves to be relevant to this research is Callista Roys Adaptation theory. Her theory generally speaks of humans interacting with a changing environment and coping with the environment through bio-psychosocial adaptation mechanisms. The focus of the study is on how an individual, family, group, communities, or society develop and further implement their adaptation to change. Also, a persons health status is determined by the way that individual cope to the external and internal stressors like environmental or physical trauma.
32 aquinas university of legazpi
Figure 1. Conceptual Framework Model
The amalgamation of these two theories would provide a support structure upon which this research can rest. The theory that Hildegard proposes in providing therapeutic relationhip to a participant with psychosocial disorder provided the appropriate approach to the patient with PTSD. Also, Roys Adaptation Model succinctly elaborated the coping mechanisms and the various adaptations that would prove therapeutic to the participant. To have a concrete view of the input, process and output of the study, a conceptual framework was observed, as seen in Figure 1. The framework model provided a thorough description of the approach during the encounter with a particiant with PTSD. The framework utilized Peplaus Interpersonal Relations Theory as the process in approaching the participant, and Callista Roys Adaptation Model elaborated the various coping mechanisms and adaptation that are deemed therapeutic to the participant. An assessment of the profile of the patient which includes the age and activities done daily provided an analysis and was relevant in discussing and relating the predisposing events that led to PTSD. A consideration of the exisiting coping mechanisms that were utilized by the patient was done since it determined the appropriate nursing interventions; and this would effectively support the participant to become a well-adapted and functional individual. Methodology This research utilized a therapeutic one-on-one communication and direct observation between the identified participant, key informant and the researcher. All accounts were written verbatim and a voice recorder was utilized for further verification of all the conversations done. The researcher assumed that this strategy provided the most comprehensive and extensive pres-
Saludamay Vol. IV No.1 33
entation of data since almost all aspects of the client were addressed. Also, a four day immersion was done in the time frame of the study. This provided a valuable resource to the study as the researcher examined the activities of daily living of the client. The Daily Living Activities Functional Assessment was utilized as a framework for the observation and interview of the client. This provided an in-depth account on the lifestyle of the patient. The process included the consent of the participant and the family to accommodate the researcher in their respective household. Data gathered during the immersion and interviews were coded and categorized so as the discussion of results is structural. Clustering of relevant data and thematizing were done so that an in-depth structural account of the life of the participant with PTSD is shown. This was the premise of which the research took into account the patient with post traumatic stress disorder. Further inquiries were also observed to provide an in-depth structural visualization of the data crucial to this research. Discussion of Results In the assessment of a participant having Post Traumatic Stress Disorder, a thorough investigation of the precipitating factors was imperative as various clusters of the symptoms of PTSD were observed and documented. This would also help the researcher to note the gravity of which the patient might or may not be experiencing. The themes that surfaced throughout the discussions were coherent to the physical and mental experiences that a person suffering from PTSD has. This would structuralize the data which support the various concepts of care that are relevant to the participants needs. Centered from the categories identified, various themes were made into light. The Table 1 shows the summary of categories and themes. Table 1. Summary of Categories and Themes Categories Activities of Daily Living Themes Health Perceptions Functionality Communication Self-Preservation Lack of Social Support Dysfunctional Adaptation Pattern Rape Trauma Occupational Therapy
Predisposing Events Coping Mechanisms
34 aquinas university of legazpi
Demographic Profile of the Participant JB is 48 years old, female and single, and is a plain housewife. She lives together with her sister in a two-storey house which they own. She is second in a brood of three; the youngest died of typhoid fever while was still young; both her parents are deceased. She is diagnosed with delayed chronic PTSD with signs and symptoms of hyperarousal, avoidance behavior during evenings and at night, and hypervigillance. Activities of Daily Living Activities of Daily Living are technically defined as areas of activities that a normal functioning person can perform within the standard criteria, which involves independence and thorough assessment of strengths and weaknesses. This functional assessment pattern has been proven to be reliable and valid in assessing what daily living areas are impacted by disability or mental disorders (Presmanes, 2005). In the discussion made with the participant, four major themes were concurrently observed, mainly: health perceptions, functionality, communication and self-preservation. Health perceptions deals with the assessment of the participants health status, mainly focusing on participants independence in self-care for physical and mental health, general health issues, mood management, sleep, and therapeutic regimen. Functionality delves more on the self-sufficiency to maintain an independent holistic functioning without the hindrances of external factors. Communication focuses on the interrelation between the participant and the society, and it measures the extent of participation emotionally, psychologically and socially. Lastly, self-preservation depicts the optimization of self-protection against harm, self-inflicted or inflicted by others. The discussion below discusses the four themes explicitly to provide background of the study in Post Traumatic Stress Disorder. Health Perceptions Health Perceptions is a major indicative factor in the assessment of almost all persons with physical or mental illness. They provide the larger factor, compared to the other categories because they are involved in the assessment of the participants perception of health status. Awareness also plays a key factor in this category as the participant must be conscious of her physical and mental needs. In effect, health practices provide the groundwork where all other categories must coincide and provide structure in the assessment and plan of care for the participant. The participants perception of her general health includes her awareness of her body. As stated: Ok naman. Di naman ako umiinom at nagsisigarilyo. Malusog naman baga ako kay nakakagawa ako trabaho dito sa bahay. Tapos umiinom naman ako ng gamot ko. Yun lang talaga na madali akong matakot. Parang sa isip na baga yun. (I guess its fine. I dont drink or smoke. I guess Im healthy because I can help in the chores in this house. And I also take my medicines. Its just that I get scared easily; its like in my mind.)
Saludamay Vol. IV No.1 35
She doesnt do anything that might harm her body physically like smoking or alcoholism. The only thing that she is concerned with is her irrational fear of the unknown which triggers a cascade of symptoms relating to PTSD. One of the first observations the researcher has discovered and has remained constant throughout the duration of the immersion is that throughout conversations, the participant kept glancing at the window. This action is usually associated with the feelings of reoccurrence which is an observable symptom of PTSD. During this period, the participant is reliving the anxiety she acquired while having to suffer the thought of a stranger raping her. This anxiety invaded her subconscious and made her think that every person or anything seen or invisible would cause her harm. Thus, this undue anxiety causes her to look at the window. Another observable symptom is that she displayed aversion of the topics or situations regarding her past experiences related to the incident. This is a type of avoidance where the participant actively avoids the topic regarding the memories that led to the trauma. Aversion of the topic would lead to denial and repression of the memories, which would further incapacitate the clients ability to have a functional life. One of the phrases the participant said about not blaming others of the pain that are selfinflicted, shows a level of understanding in her awareness of the illness she has.Alam ko na dapat di dapat natin isala ung ibang tao sa pagkakamali na alam nating tayo ang may kagagawan. Tulad ko, madaling matakot, pero alam ko ang rason kung bakit natatakot ako. Kaya ako dapat ang magadapt, di sila. (I know that we shouldnt blame other people of the things we know ourselves are self-inflicted. Like me, easily scared, but I know the reasons for my fear. So I should be the one who must adapt, not them.) This would prove important in being the first step to a therapeutic health improvement. This is adapted in Peplaus Interpersonal Relations theory as a marker for self-improvement with the aid of a professional psychiatrist and health care provider, since her need for gratification can be primarily addressed; the first step to a healthy functional person. Mood management in the participant can be said to be somewhat compromised. As stated: Hmmm, ok lang. natatakot kasi ako sa kanila, pagkatapos ng ginawa nila saakin. Mas natakot ako lumabas pag gabi. Ayaw ko na basta sa kanila. Gusto ko na sila makalimutan (Hmmm, I guess so. Its just that Im afraid of them, after what they did to me. I dont want them anymore. I just want to forget about them) The participant is easily startled and agitated by anyone, specifically a male stranger, and showed behaviors that signify fear and open irritability to the immediate environment. In the clusters of symptoms of PTSD, this would be indicative of hyperarousal or hypervigillance. The reactions that the participant showed are detrimental to her health as they impair her physical and mental functioning. One of the observations that support this phenomenon was when the participant became agitated and started crying after seeing a stranger looking at her. This is developed from the fear and anxiety of the event, which then became a constant reliving of the
36 aquinas university of legazpi
same event. This constant reliving increases the anxiety and fear that even a stranger, as long as it can be related to the event, becomes a source of fear and anxiety to the participant. This fear of strangers eventually led to fear of going outside, a sign of social inhibitions. Participant is scared to go outside of the house during evenings and night. This would be a symptom of avoidance. Most would develop this symptom from the anxiety that was associated with a certain event leading to the trauma. Since the participant was raped at night, she developed an undue fear of the dark. It was also observed that she becomes anxious and agitated at night, a demonstration of the feeling of impending doom whenever night arrives. Most of the discussions regarding PTSD involve the occurrence of nightmares. This is the manifestation of the stress and anxiety a patient has because of the trauma she suffered. In the table above, the participant was observed to be having sleep difficulties, as manifested by her decreased sleeping hours, physical manifestations of lack of sleep like dark eye bags, and constant twitching and turning while asleep. During sleep, the subconscious takes over the functioning of the brain, to the extent that it causes hyperactivity of the frontal lobe which controls the emotions. Nightmares occur because of the hyperactivity of the frontal lobe and the interjection of the subconscious. Since there is repression of memories of rape, and increased level of unresolved anxiety, the nightmare causes physical manifestations like turning and talking. The participant was also observed to have scratch marks on her left arm, probably self-inflicted while moving in her sleep, an eventual complication of having nightmares and having to move in bed. Scratching of the left arm can be associated with the nightmare related to her struggle with the assailant. As the memories are relived during her sleep, physical manifestations would include the actions of fighting someone, and this would most probably cause self-inflicted harm. Functionality One of the debilitating factors of PTSD is its capacity to inhibit the persons ability to function normally. Since the overwhelming anxiety and stress hinder the persons functionality, it is imperative that an assessment of the activities relating to personal health in the environment must be done in order to note if the patient is still capable of taking care of herself. One observation noted was that her room was messy, with clothes and paper scattered everywhere. This clearly depicts the disarray or the loss of prioritization that most PTSD patients have to suffer. The emotional and mental weight that these clients carry puts a burden in other aspects of their living. A disarrayed environment around a PTSD patient clearly states that they harbor an anxiety level that disrupts their way of living. Another observation noted was that she could focus attention to work at hand but became easily distracted if faced with a situation related to her incident. Focus on tasks at hand is a sign of progress to a participant with PTSD. This would mean that the patient has
Saludamay Vol. IV No.1 37
developed a form of coping mechanism that she tries to adapt to her lifestyle, and having this type of mechanism would mean that the participant has made goals in attaining a functional lifestyle. But, there exist the fact that she gets distracted of situations relating to her traumatic experience. This diversion of focus would mean that even though the participant has adapted a coping mechanism, the fear and anxiety of the trauma still haunts her. In these instances however, the key informant, her sister, becomes readily available to comfort her and give her support. Ayun, may mga oras na nagigising na lang yan at nagsisigaw. Tatakbo niyan ako papuntang kwarto niya para icomfort ko. Minsan mahirap na, pero kelangan mo talagang gawin. Ako nalang ung natitira niyang kapatid at pamiya. (There are times that she would wake up at night and start shouting. I would run to her room to comfort her. There are times that I find it hard to do, but I know I must. Shes the only family I have.) This support is very significant to almost all patients suffering PTSD because it provides the emotional backrest when thoughts of fear and dying comes to their mind. It also encourages the participant to develop the feelings of being needed and gratified; the foundations of healing in a mentally ill patient. Communication Communication is synonymous to socialization. The act of relating to other persons, your thoughts and ideas is a normal response and is often indicative of a healthy mind. But there are some who finds communication as stressful stimuli, seeing it as a source of intimidation. For a patient with PTSD, this idea is aggravated to the extent that those who have regressed further in the disease would be socially incapable of talking with other persons. This of course, is detrimental to a person. One of the therapeutic approaches to a patient with PTSD is promoting eventual independence through addressing the functional needs of the client which are support, open communication and a sense of being gratified. This can be done through the love given by the person closest to her heart. The cluster of symptoms of PTSD extends to point where a patient may feel socially inhibited because of the fear and anxiety that mars her adaptation to the environment. This is a serious threat to the mental health of the client as it denies her companionship, support, and gratification that may otherwise prove beneficial to her health. In the statement given by the Key Informant implies that her capacity to associate with other people is invariably threatened by fear and anxiety. Mas gusto nun sa loob lang ng bahay. Natatakot kasi yun, after nung nangyari sa kaniya nung nasa abroad siya. (sighs). Nagbago ung ugali niya. (She favors staying indoors. She easily gets scared, after what happened to her abroad.) This fear and anxiety were imprinted on her when she was assaulted physically and mentally. This could also be associated with the clusters of symptoms
38 aquinas university of legazpi
of PSTD which is reoccurrence and avoidance. Since the participant was assaulted in a public place and at night, she developed an association with these events with anxiety and impending doom. This association would further on evolve into a complication which will manifest with the participant becoming extremely agitated at night and outdoors. Also, her fear for other people was escalated with her association of them with the unknown rapist. This could prove to be a serious delineation between her reality which includes everyone being a threat to her, and her needs like support and gratification, which can be provided by other people. The researcher noted that her sister doesnt allow her to venture outside the house if unnecessary. This would aggravate the condition of the participant because her exposure to the outside environment is very limited. This situation can be related to the social stigma PTSD carries. Being diagnosed with PTSD is like being diagnosed with Sexually Transmitted Illnesses; the patient is concerned of what other people may say of their illness. Though this stress may be self-induced, it only worsens the status of the participant because it builds more anxiety and fear, to the point that it would seriously harm the physical and mental functioning of the participant. In the Adaptation theory proposed by Sister Callista Roy, a persons health status is determined by the way the individual copes with the external and internal stressors like environmental or physical trauma. A patient who suffers PTSD has impaired coping strategies that severly undermine the capacity to adapt to the changing environment. This is also aggravated by the fact that anxiety and fear rule their lives. On a more positive scale, the researcher has noted that the participant has a deep and well-formed relationship with her sister. Awww, love ko si ate. Siya ung nagtanggap sa akin pagkauwi ko dito sa pilipinas. Pero noon, nung kakarating ko palang ditto. di ko pa alam kung ano ang gagawin ko. Di ko nun masyadong pinapansin si ate kasi parang nagiisa lang ako. . . Pero nung tumagal, siya na ung nagtanggap sakin. Kaya di ko kayang mawala siya. (Awww, I love my sister. She was the one who greeted me when I arrived here in the Philippines. But, just a few months of staying here, I still didnt know what I will do with my life. I felt so lonely, that I would sometimes not notice her. She still accepted me, and as time moved on, I learned to love her. I couldnt part ways with her.) This is very therapeutic to the participant as her needs of having emotional support, open communication and gratification can be provided. This could be utilized in the steps that would lead to the therapeutic health improvement of the participant as her needs are met. The emphasis on support and gratification is very large, because this would eventually enlighten the participant that she is not alone and that her greatest fears can be overcome with therapy and family support. Self-Preservation
Saludamay Vol. IV No.1 39
Self-preservation is an indicator of physical and mental health, as it entails the efforts a person must ensure to promote and maintain personal safety. It also assesses the persons optimal self-protection in terms of physical and mental welfare. This self-protection is eminent in all aspects of life, especially on the part of self-preservation. In the case of PTSD, safety is somewhat compromised as the participant is emotionally unstable, and that her actions are guided by fear and anxiety, a marker for self-inflicted harm. This would inevitably make the participant at risk for physical injuries that could have been prevented. In the statement given by the participant, hyperarousal, a cluster of symptoms in PTSD, can be visibly observed. As quote: Oo, ung time na . . . naghihiwa ako ng pinya, tapos parang may nakita akong dumaan sa bintana. Nagpanic ako nun, akala ko kung ano. Tapos yun, nasugatan ko ang daliri. (Yes, there was this time when I was slicing a pineapple, then I think I saw someone pass through the window. I panicked because I thought it was a stranger. And it was then that I cut my finger.) This statement is indicative of hyperarousal, wherein the participant becomes hypersensitive of the situation since she still associates it with the rape incident and also, from the imprinted fear of going outside the house. Her safety in this situation is compromised because her lack of focus in the activity resulted in the cutting of her finger. This lack of focus is very observable in those diagnosed with PTSD. This stemmed down from the fact that they keep reliving the traumatic incident in their head that activities of daily living are influenced by anxiety or fear. The participant is focused on her activities, but when presented with a situation that can be expressly related to the traumatic incident, she regresses to a lower pedestal of adaptation which is crying, becoming hysterical, or becoming silent and trembling with fear. It is this fear and anxiety that makes the participant incapacitated. Predisposing Events that led to the Development of Post Traumatic Stress Disorder Post-traumatic Stress Disorder is developmental, in the sense that a person must initially experience an event that involves witnessing, experiencing or being confronted with an event or events that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others (Field 2005). From here, the person becomes mentally incapacitated and his or her coping mechanisms fail to adapt to the situation, and eventually leads to the clusters of symptoms which include persistent re-experiencing of the traumatic event, persistent avoidance of stimuli associated with the traumatic event and numbing of general responsiveness, and lastly, persistent symptoms of increased arousal or hypervigillance (Field 2005). Throughout the immersion and by process of data-gathering, three themes were observed that directly support the predisposing events that led to the development of Post
40 aquinas university of legazpi
Traumatic Stress Disorder in the participant; these three themes are lack of social support, dysfunctional adaptation pattern and rape trauma. Lack of social support is evident in the participant since throughout her life, she was neglected by significant persons. The discussion on this would revolve around her childhood history. Dysfunctional adaptation pattern denotes how the participant adapted to her losses. The resolution, if impaired, would lead to dysfunctional adaptation later in life. Lastly, rape trauma became the pinnacle which pushed the participant to become antipathetic towards society. These experiences are very troubling to almost anyone who is raped, but due to the dysfunctional pattern and lack of social support, it escalated to become Post Traumatic Stress Disorder. Lack of Social Support Support provides a therapeutic backrest to all patients with Post Traumatic Stress Disorder. It alleviates the burden and fear that the participant has due to the traumatic event that plagued her life. It also gives an emotional let out in the form of significant persons providing a listening ear to the grievances of the sufferer. This let out would prevent the build up of unexpressed fear and anxiety that would further trouble the psyche of the person. Unfortunately, this support is deprived from the participant since throughout her life, it happens that one or more significant persons were missing; especially those persons needed for the resolution of her trials. The gravity of this factor is very eminent in persons suffering from PTSD since lack of support preempts feelings of loneliness and abandonment; one of the cornerstones in the development of PTSD. The participant was left with her feelings after the death of her younger brother. Her father was absent during the burial and her mother neglected to comfort her as she was also preoccupied with her grieving. A dysfunctional grieving was observed and it was due to poor resolution of the dilemma that ignited the development of PTSD. Dysfunctional Adaptation Pattern Impairment of adaptation in certain life situations predisposes a person to losses that can only be overcome with proper therapy. The participants loss was very significant in that her failure in the resolution process led to a dysfunctional adaptation. During the death of her younger brother, as well as the passing of her grandmother, coping was rather stressed and difficult. The participants lack of social support from her significant persons and the overwhelming traumas led to a dysfunctional grieving which was not addressed early in life. Emotional factors like being averse in the company of other people and not being able to meet the gratification and support that was badly needed, the participant fell to a worse state that made adapting to situations rather difficult. This maladaptive pattern heightened when the rape trauma incident occurred, jettisoning her to a level where her everyday ac-
Saludamay Vol. IV No.1 41
tivities become dysfunctional if ever the trauma is relived inside her head. Rape Trauma According to the study conducted by Woods (2000), symptoms of Post-Traumatic Stress Disorder exist in women who were sexually abused or have been out of an abusive relationship. The traumas experienced by women during rape were inexplicable that development of PTSD is already eminent from the start. Merriam-Websters Medical Dictionary (2012) defined rape as an unlawful sexual activity carried out forcibly or under threat of injury against the will. This then falls under the category of a serious life-threatening event that incapacitates the persons will. The participant became a victim of rape while she was out of the country, and considering her history of mental instability, early signs of PTSD manifested that eventually troubled her life. This only worsened because of her lack of social support early in the trauma stage. In eventuality, the development of PTSD was indemnified in the participant as her life was put under severe stress and that her fear and anxiety were unexpressed and filled her life with horror. Coping Mechanism An adaptive coping mechanism usually entails a healthy functional mind. Various stratagems exist to provide us a wide variety of adaptive skills, all of which would suit the situations a person is at. Though the ability to utilize this mechanism is inherent to people, those who are mentally disabled find it more difficult to adapt. This is due to the onslaught of stressors that render the patient incapable of adapting to a changing environment. In most cases, those who fail to adapt with the environment become regressed and easily disturbed when a situation that can easily be handled comes to them. In the case of a patient with Post traumatic Stress Disorder, adaptation is compromised because of the fear and anxiety that envelop the persons coping skills. The traumatic event incapacitates the victims mental capacity to evaluate the situation and plan a course of action that would directly address it. So to say, a PTSD sufferer is incapacitated in areas involving decisions, affections, adaptations and cognitions. In the assessment done to the participant with PTSD, the researcher has noted that the participant engages herself with cross stitching and crocheting. Cross stitch is a type of needlework where different colored threads are woven using a needle in a tightly meshed sheet of cloth, to create pictures or patterns. Crochets are also a type of needlework which consists of interlocking of looped stitches that are formed with a single thread and a hooked needle. Sweaters, mittens, tablemats, and basically everything that could be used as covers, can be made from crochets. Both these needlework are classified as an art therapy and at the same time, an occupational therapy, and is considered to be a therapeutic exercise to
42 aquinas university of legazpi
the participant. According to the journal cited by International Art Therapy (2012), during the 20th century, art therapy was popular as a form of milieu therapy at psychiatric institutions and was an important influence on the development of art therapy in the United States. Milieu therapies focus on putting the patient in a therapeutic social setting that provides opportunities to develop self-confidence and interact with others in a positive way. This is why art therapy is preferred for PTSD patients since it involves rooting out the repressed memories and letting the patient discuss those feelings. In eventuality, cognitive behavioral therapy may be utilized to let the patient address the problem and eventually find solutions to it. According to Videbeck (2004), Occupational therapy focuses on the functional abilities of the client and ways to improve client functioning such as working with arts and crafts and focusing on psychomotor skills. This type of therapy organizes the cluttered thoughts of a mentally disabled person. In the case of a patient with PTSD, this therapy precipitates the use of psychomotor coordination, which entails diversion and momentary suppression of the traumatic thoughts of the client. This would prove beneficial because as the therapy progresses, the participant is encouraged to focus on activities at the present, rather than dwell in the traumatic thoughts of the past. Eventually, these coping strategies would help the participant in lessening the gravity of the signs and symptoms of PTSD. With proper counseling and continual support, it is possible that the participant would be relieved of Post Traumatic Stress Disorder. Nursing Care to a PTSD client The locus of nursing care in a client with PTSD is promoting and maintaining an effective relationship to address the needs like emotional support, open communication and gratification. Specific nursing practices that provide support, safety, and comfort to the patient help in decreasing psychological anxiety, stress, and helplessness. Another issue that needs addressing is her relational status with the community. Since PTSD incapacitates the persons response to the environment, the nurse should provide activities that would progressively help the client adapt to the outside environment. In effect, the care of PTSD clients is long termed and progressive in nature to better accomplish a therapeutic response.As this would be long term goals, nursing interventions would be most efficient if it could be used while the patient is in the acute phase. Nevertheless, its efficacy can also be observed in the chronic and delayed chronic stages. First nursing care to be done to the participant is to empathize with the patients feelings in a positive and accepting manner. Empathy is the core of building a therapeutic relationship with a patient. It is a process of putting oneself in the same situation as that of
Saludamay Vol. IV No.1 43
the client. Though you do not necessarily experience the situation of the client, the way you offer yourself by listening and sensing the importance of the situation gives you the feeling of what the client is experiencing at that moment. By letting the client share her feelings without judgment and the nurse continually providing her presence as a listener, trust and rapport is developed, and this positively influences client outcomes. Clients tend to feel better about themselves and more understood when the nurse is emphatic (Kunyk & Olson, 2001) In a patient with PTSD, empathy would prove very significant because it will address the needs of emotional support, communication and gratification. This could be the primary step in building a therapeutic regimen for the participant. Discuss with patient perceptions of depersonalization or fear. Depersonalization is described by the feeling of being disconnected to oneself when having a panic attack. In the cases of PTSD, fear overruns their daily functioning, and this escalates into serious complications like withdrawal, emotional numbing, and even suicide. A common assumption is that it is more harmful to question people about PTSD, than to ignore it. Nothing could be further from the truth. Untreated PTSD becomes more ingrained and less responsive to treatment (ODell 2007). It can also lead to failed personal relationships, career problems, substance abuse (self-medication), depression and even extreme acts such as suicide or homicide (ODell 2007). Once an individual manifests chronic PTSD adaptation problems, evidence shows these problems remain chronic for life (Prigerson, Maciejewski, and Rosenheck 2001). The symptoms are also resistant to treatment that works for acute PTSD (Schnurr et al. 2003) The problem though with discussing PTSD with the participant is that it triggers past memories that would make the patient regress, but still, the goal of therapy is to bring out the PTSD symptoms into the open so that the participant may become aware and ask questions about it and plan for goals to alleviate the symptom. Provide incremental exposure to social environments and support useful coping strategies. Since the participant is easily affected by the social environment, gradual exposure with consideration to anxiety level would give eventual repression of the fear. This is a type of desensitization therapy wherein gradual exposure to stressors and evaluation of clients response is made to grossly conclude if participants reaction is overt anxiety and to transform it to an adaptive mechanism. Coping strategies include exercise, increased or decreased sleep patterns, seeking information, journal writing, relaxation exercises, reading books or magazines, prayer, social support, and discussion of feelings. Also, walking 20 minutes three times per week, yoga, soothing music and progressive relaxation are other activities that increase coping responses. These techniques provide patients with a sense of control and decrease their emotional reactivity. Another Nursing care is to focus on the patient as a whole. Focusing on the patient as a
44 aquinas university of legazpi
whole provides a more holistic approach in addressing the needed care. It would encompass physical and mental health aspects, and would include relational or social, emotional and spiritual health aspects that would greatly propel the client into a functional person. Assist patient in coping with temporary changes such as bruising. Since the client is at risk for self-injury because her actions are influenced by anxiety, the nurse should address this self-harm before addressing the root cause. This can be done by cushioning the client while sleeping, since nightmares causes excessive movement and possible self-harm. Demonstrate a positive, nonjudgmental attitude. Considering that a PTSD client exhibits aversion to society, it would help in the establishment of trust and rapport if a nurse develops an unbiased approach to the client. This helps the client feel able to open up and talk about personal matters, and as discussed earlier, will help in addressing the clients needs for open communication and gratification. Provide consistent emotional support and nonthreatening information. Majority of those who develops PTSD lacks social support or have shunned themselves from the society completely because of the fear. This problem is addressed primarily by the nurse through providing continual support like being present when needed by the client, having therapeutic conversations that allow the client to explore her emotions, providing necessary information to the client regarding her disease and her options for therapy, and helping to map out possible goals that would make the client a sociable and functional person. Encourage involvement in self-care. Motivation on the part of self-care is necessary as it necessitates the client to be responsible for personal health. In the topics discussed earlier, personal health is an indicator of good and adaptive mental health. This includes the approaches a client may undertake to promote and maintain a functioning body. The nurse encourages the client by allowing her to initially address her need to accomplish self-hygiene. From this need, the nurse may work on letting the client find a solution to this need, and that is performing self-hygiene. This process may be lengthy since the participant must act independently to provide a more therapeutic outcome than having her listen to the direction or urgings of the nurse. Lastly, consider that nonverbal behavior conveys more important messages than verbal messages; the impact of facial expression is greatest, followed by the impact of vocal expression, and finally the impact of words. Considering that one-third of the meaning you want to convey to your client is expressed in words, while two-thirds is expressed nonverbally, it is imperative that the nurse should be acutely aware of the message he is sending to the client so as not to convey inappropriate or misguided meaning. In a client with PTSD, this skill would be very important as this would influence clients outcome regarding the establishment of open communication. Recommendations
Saludamay Vol. IV No.1 45
A study and in-depth exploration of a person with Post Traumatic Stress Disorder requires ample time for considering the variety of data that will be used in the research. As such, it is of great importance that the researcher should always consider the time of the participant because we can never impose. To further enhance this study, the research recommends the use of Gordons Functional Assessment in the study of activities of daily living as it would cover all aspects of health in a mentally ill patient. Also, further study in the various therapies specific to PTSD client is imperative as nursing care will be based on such. Another factor that might be considered for this research is orientation on therapeutic communication and the theory of its application. Being a nurse, one cannot escape communicating with patients, especially if the patient is mentally ill. It is then imperative that the nurse must have a concrete knowledge in therapeutic communication and how it is applied in its appropriate setting.
REFERENCES American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders: DSM-IV. Washington, DC: American Psychiatric Association Andreasen, N.C. Acute and delayed posttraumatic stress disorders: a history and some issues.A merican Journal of Psychiatry 161 August 2004:1321-1323. Biology of PTSD (2008). Woodland Park, CO: PTSD Support Services http://www.ptsdsupport. net/ Carreta, C., Jaroszynski, A., Rankin, M., (2008).Nursing Care of Posttraumatic Stress Disorder after Anesthesia Awareness. Plastic Surgical Nursing (Volume 28) Dixon, R. (2008). PTSD Type Symptoms and CGSC Class 08-01, A Study of Field Grade Officers and Implications for the Future. Published Masteral Thesis. Domrose, C. (2008). Patients and RNs face Unprecedented Stress. Nurse Week. 30 Field, Tim. (2005). Stress injury to health trauma, PTSD. Oxfordshire, UK: The Field Foundation. http://www.bullyonline.org/stress/ptsd.htm
46 aquinas university of legazpi
Mental Health News.(2007) Prevalence and Correlates of Post Traumatic Stress Disorder and Chronic Severe Pain in Psychiatric Outpatients. ODell, Richard E. (2007). Do I have PTSD? Richmond, VA: The PTSD Help Network. http:// www.ptsdhelp.net/index.html Tull, Matthew. (2007). Who gets PTSD? New York, NY: About.com. October 31 http://ptsd. about.com/od/prevalence/a/prevalence.htm Videbeck, Shiela L, (2004), Psychiatric and Mental Health, 2nd Edition, pg. 223-224, 290 Weathers, Frank W., Brett T. Litz, Debra S. Herman, Jennifer A. Huska, and Terrence M. Keane, 1993. The PTSD checklist (PCL): reliability, validity, and diagnostic utility. Paper presented at the Annual Meeting of International Society for Traumatic Stress Studies. San Antonio, TX. http://www.pdhealth.mil/library/downloads/PCL sychometrics.doc,
Saludamay Vol. IV No.1 47
SPIRITUALITY: IMPLICATION TO THE END-OF-LIFE CARE OF ELDERLY PATIENTS IN HARONG KAN SAGRADA FAMILIA
Cherry Joy F. Flores Jennybelle F. Go Christine Joan V. Luzuriaga
Introduction Spirituality has been defined in numerous ways. These include: a belief in a power operating in the universe that is greater than oneself; a sense of interconnectedness with all living creature; and an awareness of the purpose and meaning of life the development of personal, absolute values. Spiritual care is actually best delivered the same way as other types of care are rendered, by communicating the health team and involving the family of the client. Spiritual care is rather less materialistic in interventions designed to develop, promote and support the provision of spirituality (Goudarzi, 2004). This study promoted benefits to the recipient of care and distinguished the implications of spirituality in the end of life care to the elderly residents in Harong kan Sagrada Familia. The study used qualitative research method. It was able to find answer about spiritual implication. The profiles of the respondents include: age, gender, religion, and educational attainment. This study also determined the different spiritual values and practices along with their personal, familial and cultural aspect. Implications of profile were also made. Coping strategies that can be proposed to enhance spirituality are included in this study. This study will provide a rationale, why spiritual nursing care should be included in the care of the clients and consider it as an important matter in the field of nursing. Statement of the Problem 1. What is the profile of the participants in terms of: a. age b. Gender c. Religion d. Educational attainment 2. What spiritual values and practices are performed by elderly along a. personal
48 aquinas university of legazpi
b. familial c. cultural 3. What are the factors that affect the spiritual values and practices of the participants along the personal, familial, and cultural aspects? 4. What coping strategies may be proposed to enhance the spirituality of the elderly during the End of Life Stage? Conceptual Framework The theories of Madeleine Leininger and Jean Watson were used in this study to establish appreciative concepts of spirituality as a form of advantageous end of life care and on how different influences build up the spirituality of certain individuals. These theories also helped in further understanding of the big implications of spirituality in cultivation and preservation of human and spiritual being. According to Madeleine Leiningers Sunrise model under Cultural Care Diversity and Universality Theory, there are assumptions concerning care: culture care values, beliefs and practices are influenced by and tend to be embedded in the worldview, language, philosophical, religion (spirituality), kinship, social, political, legal, educational, economic technological, ethnohistorical and environmental contexts of cultures. These given factors result to an inclusive holistic lifeways of people since culture influences their way of thinking so as to choose between accepting and denying certain and natural limitations of life like as on the end of life stage. Jean Watsons Human Caring Theory shows ten caritas process which possess greater spiritual dimensions and an evident rendering of love and caring to the clients. She has enlisted the instillation of faith- hope; this enables the client to go to the deeper belief system and subjective life world. This shows that if modern science has nothing further to offer to person, the nurse can continue to use faith- hope to provide a sense of well-being through beliefs which are meaningful to the individual. Next is the cultivation of sensitivity to ones self and others, the focus of this is to nurture the spiritual practices, to encourage self growth and self- actualization and to go beyond ego self to reach a deeper spiritual connection to promote comfort and healing process. Another caritas process is the provision for a supportive, protective, and/or corrective mental, physical, societal and spiritual environment, which depicts about creating healing environment at all levels (physical as well as non-physical), subtle environment of energy and consciousness, whereby wholeness, beauty, comfort, dignity, and peace are potentiated. She also have included the assistance with gratification of human needs that assists with the basic needs, with an intentional caring consciousness, administering human care essentials which potentiate alignment of mind body spirit and unity of being in all aspects of care, tending to both embodied spirit and evolving spiritual emergence. Lastly, allowance for existential- phenomenological- spiritual forces; this leads to the opening and attending to spiritual- mysterious and existential dimensions of ones own life- death; soul care for self and the one- being- cared for. This theory focused
Saludamay Vol. IV No.1 49
on the possible strategies that could enhance the spirituality of the elderly residents in Harong Kan Sagrada Familia. Methodology This study used a qualitative research approach. The qualitative research used the data gathering and data analysis. The data included the rigid assessment of participants. Who were the residents of Harong Kan Sagrada Familia, Bogtong, Legazpi City. The main focus were the elderly participants with an age bracket of 65 and above and still in the proper cognitive functions. The information from the participants was the main basis of analysis and interpretations. Interviews from the key informants who are the nurses of each participant were also conducted. Articles from the internet, journals and books served as supplements of the study. The gathered data had been clustered, categorized and thematized. In addition it had been examined for generalization and further recommendations. Gathered data had been the major premises that validated the implications of spirituality to the elderly clients as a form of end of life care. Interpretations and Implications: After processing the data of this study, the following discussions were made to analyze, interpret and make implications. Profile: Spiritual Values and Practices PERSONAL - GOD ABOVE ALL THINGS The participants were all individuals with age from 65 to 69. They differ in their educational background yet what is common to them is their wisdom. All of them practice a profession in their own right. They differ in their educational attainment, yet they all believe that God is the center of their lives. They are all service - oriented individuals and so they do spend time in service to others. These participants consider God as the most important thing in their lives by this time. They say that God moves their lives, through different ways. The spirituality by which they have acquired this time plays a major role in their development as an individual. To the elderly participants, God moves in different ways and inspires one to be spiritually healthy. As the doctor of philosophy said, My faith was boosted. He is the light of the way. He is my comforter. As I pray I find peace. Such perspective is very important to the participants in the preservation of their health be it physical, mental, spiritual or emotional. The fifth participant is a nun. At 65, she has retained the goodness in her, and as manifested in the interview she has retained her love for the people and her passion to serve others.
50 aquinas university of legazpi
Her view of spirituality is as vivid as her vision of life. It is wide and broad. She is indeed a loving nun. Her age did not affect her vision and love for service and her love for God. Spirituality works in their life. It is in God that they turn to at their age of 60s. FAMILIAL - IN UNITY THERE IS STRENGTH The families of all the participants are all intact. They all have close family ties. The family is together in one belief or devotion. Together they pray and practice their spirituality as one. This research found out that each one in the family performs a specific responsibility which enables the participant to do his functional role in life. In effect, the individual was able to perform his duties and responsibilities well and finds fulfillment in all his activities. The family plays an integral part in the well being of every individual. If the family is supportive in all of ones activities, then the person involved will feel that his life is complete. There is no hindrance to whatever he or she would wish to achieve even at the late part of his life. At this point, the respondent considers unity and strong faith in God as a factor in shaping ones identity as a spiritual being. What is more important for them is to serve the people and to serve God. When the family is united in their profession of faith, there is obedience and support for each other, everyone attends holy hours, and the family becomes a strong foundation of ones well-being. This research found out that strong family ties count so much in ones search for spirituality. Community - Respect for ones belief Cultural Influences among the participants is not so much felt. In a barangay where the three participants came from, varied religious organizations exist yet there is no conflict arising from among them. The people are one or united with each other in spite of the fact that they belong to different religious groups. There is respect for each other. On the other hand, as for the member of the Knights of Columbus, it is noted that his organization is within the religious group where he belongs. In effect, it is an added way for him in the exercise of his spirituality. It is one way to thank God for the second life He has given him. Participant 5 though she is just in the convent, it has also been a big help for her to be happy and to feel that she is not alone. It made her nearer to God. It was also an implementation of her desire in life, to serve God and people. Influences also endowed her strength to continue her devotion to God but then ever since she already has the feeling and dedication to serve God. This research then found out that the effect of the community in the fulfillment of ones spirituality is big. Though the effect is not to compete with anybody, nor to boost ones religion but rather to show unity and camaraderie among the distinct groups. Within an
Saludamay Vol. IV No.1 51
organization, ones spirituality is strengthened and among and in between groups, respect for ones spirituality resides. Factors that Affect Spiritual Values and Practices According to the data gathered, the factor that strikes their spiritual practices and values in terms of personal aspects were illness/disease and emotional problems. Elderly clients were usually affected by the illness or disease that they have suffered from, they can either see it in two sides, they may interpret it as a form of punishment or affirmative one. Somehow this factor affects some elderly leading to a failure of performing some of their spiritual practices and obligation to their respective works. On the other hand, as they go through, it served as a medium to focus on their spiritual self and engage with God. Some elderly thoroughly directed themselves to attachment with God though they suffered from such illness or diseases. Illnesses are not problems, but merely symptoms or symbols of the real problem. The real problem is spiritual and results from an imbalance in ones thinking, attitudes and feelings. Disease can teach the lessons to learn. Awareness of this and work toward dealing with those lessons, that work can raise to a higher state of being than before. Disease is often necessary to teach a lesson. It can only be truly healed when that lesson is learned. That willingness to heal comes from the soul. Most often, healing occurs when an individual is ready, and willing, to make some major changes in his or her life. The achievement of balance and harmony on one level automatically requires and affects balance and harmony in the others. We must pay attention without judgment to all areas of our lives when we are in a state of imbalance. Our bodies are merely temporary instruments to be used for the fulfillment of the purposes of our Higher Self. Being aware of this is the first step toward paying attention to the messages our bodies are sending us. This is the essence of holistic healing (Rogers, 2003). There were two participants that were affected by their emotional problems; one participant had been widowed and the other one had been left by her husband. Since they were emotionally disturbed, their inner self had been diverted to the problems for a long time and their connection with God, environment and people had been neglected. The decision to end a relationship and death of a husband can be traumatic, chaotic, and filled with contradictory emotions. Usually directions get awry. These elderly were in the despair stage. According to Eriksons Psychosocial Developmental Stage, at the age of 65 and above the elderly clients see the opposite disposition, failure in life and feeling of waste. Participants thought about the dogmatism that theyve experienced and questions the Higher Power why those things happened to them. They have forgotten how to understand the inner meaning of illness, pain and suffering. All mental, emotional and physical manifestations of problems are the result of a metaphysical (spiritual) cause -- the hidden meaning of illness. Older adults may turn to spirituality and religion when they meet difficult life changing events and experience personal losses. Their reaction to these events and losses may cause distress, temporary or chronic psychological conditions.
52 aquinas university of legazpi
The data found out that the support of the family aggravates the spiritual self and enthusiasm in engaging in spiritual practices and pursue them to still go through the journey of life. All families have culturally influenced patterns of responsibility to meet the care needs of older family members. Family members are participants in informal social support networks (places where the elder prefer to live and where his/her health and social needs are best met) (Andrews and Boyle, 2003). The effect of family support to elderly clients is that whatever the family practice and value, elderly individuals follow and aid them to continue what they have already started. Usually the spirituality of family members are congruent to their elderly members. What is common in the responses of the participants was the formal support they receive to continue their connection with God and the spiritual self. Elderly clients of this research engaged into religious groups in their locale. Almost all of them serve their respective church or kapilya. Traditions and culture that arise from the community they live in greatly affect how they act and behave. They engage in organizations in their community in order to fulfill the best quality of life they are striving for. In relation to this, the wisdom and integrity acquired through attending mass every Sunday, offering service to the church and at the same time valuing it as a profession. Through their presence in some religious affiliations, respect was the first one to gain and the eagerness of each elderly client to pursue their relationship with God. Individuals may experience both spirituality and religion very privately within themselves (internally), and/or through social interaction with persons and organizations in an external way. Spirituality is about our existence, relationships with us, others and the universe. It is something we experience and requires abstract thinking and will. Spiritual development provides us with insight and understanding of ourselves and others (Twycross, 2001). Nature of Spiritual Values and Practices performed From the responses given by the participants the following elicits the nature of spiritual values and practices they performed. a. Ang makapaglingkod sa Diyos at ang maging isang epektibong katekista. To serve God and to be an effective catechist. b. Ang makapagsilbi sa Diyos at sa mga bata. And that is to serve and the children. The children are the faces of the Lord. Being service oriented, is one nature of mans spirituality. They have that desire to help other, to tech, to assist. This is one nature of spirituality as gathered from the responses of the participants. c. Hindi nila ako pinabayaan. Pag nakikita nila akong malungkot kinakausap nila ako. Sila rin ang naghikayat sa akin na tanggapin ko ang pagka day care worker sa aming
Saludamay Vol. IV No.1 53
Barangay. Yes they did not abandon her. Whenever shes sad they talk to her. They encouraged her to be a day care worker. d. Opo. Magkakasama po kaming nagsisimba at sinasamahan nila akong palagi. Yes, they always attend mass together and they are always with her. Manifestations of support are also very important which shows that majority of the practices are family-oriented. Participants especially on the lowest ebb of their lives cling on to their loved ones. They find strength in the signs and acts of comfort from their friends and family. Spiritual values shown by the participants are by nature acquired through families. It is usually handed down from one generation to another. Spirituality is an inheritance from parents or from the ancestors. e. Meron po. Pero magkaiba man ang aming relihiyon ay Diyos din ang centro ng kanilang buhay. Sa ganon po ay walang alitan sa alinmang sekta sa aming Barangay. Yes there is. They differ in religion but they both believe that God is the center of there life. There is no conflict between groups in there barangay. Meron po ng ibang religious groups sa lugar namin. Hindi po ako at ang aking pamilya pumapasok sa simbahan nila. Pero nakikisalamuha po kami sa mga taong may ibang relihiyon. Meron pang iba na hindi kami kasama pero iginagalang namin ang kanilang paniniwala. This means that, there are other religious groups in the community. They do not go to their church but they respect them in their profession of faith.
f.
Finally, the nature of the spirituality of the participants interviewed is not selfish in nature but humanitarian and respects the freedom of others. Types of Spiritual Values and Practices Performed Here are the responses of the participants that show the types of spiritual values and practices performed. From these responses the variety of Spiritual Values and practices performed by the participants are found. 1. The Spiritual Values and practices that are done religiously. They are performed or done often and usually at regular intervals of time. As a participant said, sa araw-araw, una sa lahat ako ay nanalangin sa diyos. Tuwing Linggo, ako ay palaging nagsisimba. Sa ganon ay payapa ang aking kalooban. Every day I pray. Every Sunday I attend mass. With that I find peace. 2. The Spiritual Values and Practices that are acquired and strengthened by an experience. As when asked if God is one of the controlling forces in finding ones inner harmony to find the sense of value in life, then one participant said: Very much. He gives me mysecond life. 3. The Spiritual Values and practices that are anchored on Trust. These were manifested when the participant said, Magtiwala sa Panginoon. Ang lahat ng hirap at ginhawa sa ating
54 aquinas university of legazpi
buhay ay ialay natin sa kaniya. Trust in God. Offer all the joys and the difficulties in life to him. Another instance was when the other participant said, Siya ang tanglaw ng ating daan. Siya ang takbuhan ng mga naaapi. Sa aking mga pagpapanalangin ay aking naramdaman ang kapayapaan. 4. He is the light of the way. He is her comforter. As she prays she finds peace. In this regard, whatever is the type of spirituality performed by the participant is his choice. What is important is it will give him/her fulfillment and a sense of belonging. Effects of Spiritual Values and Practices The participants of this research are all positive in saying that the effect of these spiritual values and practices are great. As one of the participants say, he started his strong engagement to church activities. I am so thankful for my second life, he said. On another instance, he said Yes. I dont feel that Im lame. All that I think of is to serve God through his people. This means that the effect of Spirituality to the elderly is that it gives them the feeling of security. With God as the center of ones life then you wont feel lame. Even in misfortunes like an accident, if you are strong in your faith then one wont get lost. One would survive and continue to hang on to his strong engagement to God, the giver of life, the light and strength of the sick and the lonely and the guide (gabay) of all the afflicted. In another interview, another participant said:. Ang matapat na samahan ng mga tao sa aming Barangay sa ano pa man siyang sekta o relihiyon napapabilang ay nakatulong sa akin para pahalagahan ko rin ang aking nakagisnang relihiyon. Walang diskriminasyon sa aming barangay. Unity of the people in our barangay helps me to value my religion. There is no discrimination in our place. In the conduct of catechesis, the catechist said that as she teaches she feels the surge of joy or the happiness in her system. In her work what is important is not the stipend but rather the thought of sharing to the people especially to the children what she knows and what she needs to teach. By serving others, she already felt that she too is serving God. The elderly participants of this research gather strength from their prayers and also from their families. In many cases, spirituality was inherited. Such was simply handed down to them by their parents. Their religion existed before they were born. One said,Ito po ay namana ko na sa mga magulang ko. Kinagisnan ko na ito. I inherited this belief from my parents. This is my religion since birth and so I will live with it. Coping Strategies At age of 65 and above, it is now inevitable that people would feel sick, weak or lonely. These coping strategies helped the participants of this research to cope with the problems they encountered. Pag akoy nagkakasakit,meron sa aming grupo ng tinatawag na pagpapahid ng
Saludamay Vol. IV No.1 55
langis. Pupunta ako sa kapilya at kamiy mananalangin. Maraming beses na akong napagaling ng pagpapahid ng langis. At yon ay dahil sa paniniwala o lakas ng ispirituality. When I get sick, there is a practice in our church called pagpapahid ng langis. For many times this type of healing cured me. The coping strategy used in this case is spiritual healing. At another situation, the participant believes that it is important for the other members of the family to know what is going on. So she makes her physical condition always known to her children and to her grandchildren. They are always by her side to support her both spiritually and financially. Her coping strategy is as simple as openness and the feeling of security clinging on to the Lord with her family by her side. To the other participant, when conflict on schedules arises, then she will opt to do church activities. In case of illness, pray over is cure. Thats the spiritual healing that they usually do even for sick people. The strength of prayer heals the sick. The other coping strategy adopted by the fourth participant is strong engagement with God. Live a prayerful life. For the fifth participant though she had in the convent, prayers were the foundations of her Spiritual Practices. Recommendations To further enhance this study, The Nurses, Health Care Providers, Physical Therapist in Harong Kan Sagrada Familia may conduct spiritual orientation on how to go through the stage of old age and be able to empathize with the elderly during the winter season of their life. Instill faith and hope to the elderly patients through beliefs which are meaningful to them. In all aspects of care there may be provision of accommodating, counteractive and spiritual environment through exploration of the elders spiritual forces that contribute to their physical and nonphysical healing. Put the elderly religiously into a situation where they could speak pray, and share in order to have a feeling of completeness and achievement. Encourage the elderly to verbalize their fear of death and help them accept death as a completion of life. Let them realize the deep sense and meaning throughout their life. Also take into account the spiritual background of the elderly patients in order to endow the appropriate spiritual care needs. In creating the plan of care to elderly residents, they should involve the family members or friends throughout the stages of planning and discussing care needs if the client permits. Maintain and sustain their self in the very situations that compromise them. So that individuals can be free to do their spiritual work if they choose. To the elderly participants in Harong Kan Sagrada Familia they should be encouraged to be a part of a group where together they could profess their spirituality freely. Engage in family hours and continue their phenomenological extension of their Spiritual Practices and Beliefs that represent their Spirituality.
56 aquinas university of legazpi
REFERENCES De Guzman (2009) Spirituality in Nursing: Filipino Elderlys Concept of Distance from and Involvement with God, Retrieved fromwww.tadfoline.com Dover and Bacon (2001) Communication in Nursing 2004 Mendoza (2001) GERIATRIC HEALTHCARE CENTER FOR FILIPINO.Retried from www. cydf821philipines.com/files/CDYDFI. Geriatric Healthcare Center_for_Filipinos_5.pdf Molinatti Joseph (2004) The significant of Spirituality in the Elderly. Retrieved from www.bookpump.com National Consensus Panel Report.Improving the Quality of Spirituality Care 2009. Retrieved from www.sdiwori.org Nelstrop (2008). The Spirituality Care of Older People: Do we know what good practice is? The Wisdom of Age: Caring for those in the 4th Age Retrieved fromhttp://www.rcc.ac.uk/ downloads/simeonreportl.pdf Puchalski (2001).The role of spirituality in the health care. Retrieved from www.ncbi.nih.gov/ pmc/articles130500 Riley, J.B. (2004). Communication in Nursing.Mosby Incorporation. Retrieved from http:// www.elsevier.com Sangesh (2010). Spirituality and personal development Retrieved from www.articlesbase.com/ motivational-articles/spirituality-and-personal-development-2935771.html Tschudin, V. (2003) Ethics in Nursing. Elsevier Science Limited. Villas(n.d.) from Carolyn E. Dominguez THE CARING HOLY FACE REHABILITATION CENTER FOR MENTAL HEALTH: AB ASSESSMENT.2006 College of Nursing in Ontario (1999), Culturally Sensitive Care Retrieved fromhttp://www.cno. org/Global/docs/prac/41040_CulturallySens.pdf
Saludamay Vol. IV No.1 57
KNOWLEDGE LEVEL ON SEXUALLY TRANSMITTED INFECTION OF NURSING STUDENTS IN AQUINAS UNIVERSITY OF LEGAZPI
Adria P. Fulgar Jayvee Renz O. Martinez Marnelli C. Marquez
Abstract
The study identified the knowledge level of nursing students of Aquinas University of Legazpi on sexually transmitted infections. It aimed to assess what the students already knew and what they did not know about STIs. Specifically, it sought to answer the following problems: 1.What is the profile of respondents in terms of: A.) Age, B.) Gender, C.) Civil Status, D.) Religion, and E.) Year Level? 2. What is the knowledge level of the respondents with regards to sexually transmitted infection (STI) specifically on: A.) Etiology, B.) Transmission, C.) Prevention of infection, D.) Medical Management, E.) Nursing Interventions? 3. What factors affect the knowledge level of respondents on STI? 4. What are the measures that may be proposed to enhance the knowledge of the respondents on STI? Based on the data, the following findings were obtained: 1.) As to the demographic profile on age, there were 85 or 65.89% student nurses age ranged from 16-19 while on the other hand, there were 2 or 1.55% of them were aged 28-31. On gender, student nurses were comprised of 99 or 76.74% of females and 30 0r 23.26% males. On religion, most of the student nurses with a frequency of 113 and a percentage of 87.60 were Roman Catholics while least of them with a frequency of 1 and a percentage of 0.78 were Islam, Iglesia ni Cristo and Baptist. On year level, there were 20 or 15.50% respondents in second year, 42 or 32.56% in third year and 67 or 51.94% in fourth year.
58 aquinas university of legazpi
Table 1. Demographic Profile
Student Nurses f 85 37 5 2 129 30 99 129 113 2 9 1 1 1 2 129 20 42 67 129 % 65.89 28.68 3.88 1.55 100 23.26 76.74 100 87.60 1.55 6.98 0.78 0.78 0.78 1.55 100 15.50 32.56 51.94 100
Indicators Age 16-19 20-23 24-27 28-31 Total Gender Male Female Total Religion Roman Catholic Seventh Day Adventist Born Again Iglesia ni Cristo Baptist Islam Protestant Total Year Level 2 3 4 Total
For table 2, Nursing students from levels 2, 3 and 4 had different knowledge level on the etiology, transmission, prevention, medical management and nursing intervention. There were 94.57% student nurses who knew that herpes simplex was one of the causes that could be found in STIs. They also knew, with a percentage of 89.92%, that gonorrhea, caused by Nisseriagonorrhea, was a sexually transmitted disease involving infection of the columnar and transitional epithelium. There were about 85.27% of student nurses who knew that cold sore or fever blister was an infection of the face or mouth caused by herpes simplex. On the other hand, 60.47% of student nurses did not know that Nisseriagonorrhea could be killed by ordinary disinfectant. In
Saludamay Vol. IV No.1 59
addition, there were some of them with a percentage of 31.78 did not know that the etiologic agent of HIV was HTLV-3 or retrovirus. Lastly, there were 30.23% student nurses who did not know that Treponemapallidum was the causative agent of syphilis. Table 2 Knowledge Level of Student Nurses on Etiology of Sexually Transmitted Infections
Yes f 122 % 94.57 f 7 No % 5.43 f Total %
Indicators 1. Do you know that herpes simplex is one of the causes that can be found in sexually transmitted infection? 2. Do you know that cold sore or fever blister is an infection of the face or mouth, caused by herpers simplex virus? 3. Is Chlamydia a viral infection that causes STI? 4. Do you know that gonorrhea is a sexually transmitted disease involving infection of columnar and transitional epithelium by Nisseria gonorrhea? 5. Treponema pallidum is the etiologic agent for syphilis? 6. Do you know that HIV is caused by HTLV3/ retrovirus? 7. Do you know that genital wart is caused by human papilloma virus? 8. Do you know that treponema pallidum, is the one that causes syphilis, which can pass through placenta and infect the developing fetus? 9. Do you know that Neisseria gonorrheae can be killed by ordinary disinfectant? 10. Do you know that the causative agent of Chlamydial infection (Chlamydia trachomatis) can usually cause and result to urethritis in male and cervicitis in female?
110 99
85.27 76.74
19 30
14.73 23.26
116
89.92
13
10.08
90 88 107
69.77 68.22 82.95
39 41 22
30.23 31.78 17.05 129 100
99
76.74
30
23.26
51
39.53
78
60.47
88
68.22
31
24.03
For Table 2.1 sexually transmitted in-Infection can be transmitted through different means. Most of the students with a percentage of 96.12 knew that AIDS could be transmitted through blood transfusion and as well as transplacental. In addition, 95.35% of them knew that having sexual activity from same gender that had one of the said STIs could increase the risk of transmission. With the same percentage, they also knew that fluids and secretions from an infected
60 aquinas university of legazpi
partner could facilitate transmission of infection to another partner. There were 90.70% of student nurses who knew that sexual contact included more than just sexual intercourse (vaginal and anal). On the contrary, there were 41.09% of student nurses who did not know that kissing had lesser risk in acquiring STI. Some of them, with a percentage of 22.48%, did not know that a person infected orally with herpes simplex could transmit the infection by kissing and sharing utensils. Students from levels 2, 3 and 4 with a percentage of 21.71% did not know that Gonorrhe can be contracted sexually and from public or shared toilet seats. Table 2.1 Knowledge Level of Student Nurses on Transmission of STIs
Yes f 100 101 76 117 % 77.52 78.29 58.91 90.70 f 29 28 53 12 No % 22.48 21.71 41.09 9.30 f Total %
Indicators 1. A person infected orally with herpes simplex can transmit the infection by kissing and sharing kitchen utensils. 2. Is gonorrhea can be contracted sexually and from public or shared toilet seats? 3. Kissing has a lesser risk in acquiring STI? 4. Do you know that sexual contact includes more than just sexual intercourse (vaginal and anal) 5. Is having sexual activity from same gender that has one of the said STIs can increase the risk of transmission? 6. Do you know that fluids and secretions from an infected partner can facilitate transmission of infection to another partner? 7. Does oral sex cause STIs? 8. Do you know that conjunctivitis, otitis media and pneumonia may develop to children born to mothers with Chlamydia infection passed through birth canal? 9. Do you know that AIDS can be transmitted through blood transfusion and as well as transplacental? 10. Do you know that AIDS can be transmitted by breastfeeding?
123
95.35
4.65 129 100
123 114 104
95.35 88.37 80.62
6 15 25
4.65 11.63 19.38
124 102
96.12 79.07
5 27
3.88 20.93
For table 2.2shows how sexually transmitted infection can be prevented in different ways. Most of the student nurses with a percentage of 98.45 knew that STI could be prevented. With a percentage of 96.12%, they knew that regular check-up could be a helpful way in preventing a
Saludamay Vol. IV No.1 61
person from acquiring such infection and their complications. In addition, they also knew that information dissemination on the said infection was one way of preventing it. Despite the different ways to teach preventions to the student nurses, they still had some concepts about prevention that they did not know. Some of the student nurses, with a percentage of 49.61 did not know that using a spermicide could help prevents STI. There was 46.51% of who did not know that sexual abstinence until marriage was the only 100% effective means of STI prevention. Lastly, 24.03% of the student nurses did not know that abstinence was the best way to prevent STI. Table 2.2 Knowledge Level of Student Nurses on Prevention of Sexually Transmitted Infection
Yes f 127 114 111 65 69 113 113 98 123 124 % 98.45 88.37 86.05 50.39 53.49 87.60 87.60 75.97 95.35 96.12 f 2 15 18 64 60 16 16 31 6 5 No % 1.55 11.63 13.95 49.61 46.51 12.40 12.40 24.03 4.65 3.88 129 100 f Total %
Indicators 1. Can STI be prevented? 2. Do you know how to prevent STI? 3. Do condoms prevent STI? 4. Should you use a spermicide to help prevent STI? 5. Does sexual abstinence until marriage is the only 100% effective means of STI prevention? 6. Condoms do not fully prevent the spread of AIDS? 7. In order to best protect oneself and the partner from STIs, the used condom and its contents should be assumed to be infectious? 8. Do you know that abstinence is the best way to prevent STI? 9. Information dissemination on the said infections is one way of preventing it? 10. Is regular check up a helpful way in preventing a person from acquiring such infections and their complications?
For table 2.3 shows the different medical managements which could be used to diagnose STIs. Majority of the student nurses with a percentage of 97.67 knew that diagnostic tests were more useful for assessing prevalence when the test results were specific for active infection. This was followed by 93.80% of the student nurses who knew that other STIs require a blood test or sample of any unusual fluid (such as abnormal discharge from vagina or the penis for gonorrhea or Chlamydia) to be analysed in a lab to help establish a diagnosis. There were 86.82% of student nurses who knew that some STIs, such as genital herpes
62 aquinas university of legazpi
and HIV (which leads to AIDS) could not be cured and could only be controlled with medication. There were some concepts about medical management that student nurses did not know. There were about 44.96% of student nurses who did not know that inoculation of specimen on Thayer-Martin medium was the diagnostic exam for females infected with gonorrhea. In addition to this, there were 25.58% of student nurses who did not know that the drugs of choice for pregnant women infected with gonorrhea were ceftriaxone plus erythromycin. About 24.03% of them did not know that males infected with gonorrhea had a different diagnostic exam compared to females, which was gram-staining. Table 2.3 Knowledge Level of Student Nurses on Medical Management of Sexually Transmitted Infection
Indicators 1. Do you know that diagnostic tests are more useful for assessing prevalence when the test results are specific for active infection? 2. Do you know that other STIs require a blood test or a sample of any unusual fluid (such as abnormal discharge from vagina or the penis for gonorrhea or Chlamydia) to be analyzed in a lab to help establish a diagnosis. 3. Some STIs, such as genital herpes and HIV (which leads to AIDS), cannot be cured, and can only be controlled with medications? 4. Do you know that Vaccines against HPV and hepatitis B is available and effective? 5. Is fluid or tissue sample included in the STI screening? 6. Do you know that western blot is the confirmatory diagnostic testfor HIV/AIDS? 7. Do you know that the drugs of choice for pregnant women infected with gonorrhea are ceftriaxone plus erythromycin? 8. Do you know that oral anti-viral drugs such as acyclovir, famciclovir or valacyclovir are the treatments for herpes simplex? 9. Do you know that inoculation of specimen on Thayer-Martin medium is the diagnostic exam for females infected with gonorrhea? 10. Do you know that males infected with gonorrhea have a different diagnostic exam compared to females, which is gram staining? Yes f 126 % 97.67 f 3 No % 2.33 f Total %
121
93.80
6.20
112 111 110 102 96
86.82 86.05 85.27 79.07 74.42
17 18 19 27 33
13.18 129 13.95 14.73 20.93 25.58 100
103
79.84
26
20.16
71
55.04
58
44.96
98
75.97
31
24.03
Saludamay Vol. IV No.1 63
Table 2.4 Knowledge Level of Student Nurses on Nursing Intervention of Sexually Transmitted Infection
Indicators 1. Education and counseling of persons at risk on ways to avoid STIs through changes in sexual behaviors is one of the five major categories of the prevention and control of the infections? 2. Does health education an effective way of imparting knowledge regarding the risk and prevention of STI? 3. Do you know that advising infected person to do abstinence from sexual intercourse, until treatment has been completed, can be a clinical intervention? 4. Does an infected person need to learn the mode of transmission, complications, and the risk for other STIs? 5. Do you think it can help to advise the infected person to keep his/her infection secret and dont report to public health department? 6. Promoting programs of the government and non-government groups that aims to the prevention of STI is one of the roles of a nurse? 7. Encouraging and distributing the use of condoms can prevent the spread of the said infections? 8. Encouraging vaccination against STI is one intervention that can be done by every health care personnel? 9. Do you know that one of the essential nursing interventions for STI like herpes simplex is hand washing? 10. Report all cases of syphilis to local public health authorities and referthe patient and his sexual partner for HIV testing. Yes f % f No % f Total %
116
89.92
11
8.53
114
88.37
15
11.63
108
83.72
21
16.28 129 100
114
88.37
15
11.63
79
61.24
50
38.76
112
86.82
17
13.18
112
86.82
17
13.18
117
90.70
12
9.30
105
81.40
24
18.60
111
86.05
18
13.95
Table2.4. shows that nursing interventions were also important in treating STIs. One of the nursing interventions that 90.70% of the student nurses knew was encouraging vaccination against STI that could be done by every health care personnel. There were also 89.92% of student nurses who knew that education and counselling of persons at risk on
64 aquinas university of legazpi
ways to avoid STIs through changes in sexual behaviours was one ofthe five major categories of the prevention and control of the infection. There were also 88.37% of the student nurses who knew that health education an effective way of imparting knowledge regarding the risk and prevention of STI. Same percentage of student nurses knew that infected persons need to learn the mode of transmission, complication and the risk for other STIs. Some of them, with a percentage of 38.76 knew that advising the infected person to keep his or her infection secret and not to report to public health department could not help the existing problem. On the contrary, few of them, with a percentage of 18.60 did not know that one of the essential nursing interventions for STI like herpes simplex was hand washing. There were also 16.28% of student nurses who did not know that advising the infected person to do abstinence from sexual intercourse until treatment has been completed could be a clinical intervention. Table3 Factors Affecting Knowledge Level on STIs
Factors Affecting Knowledge Level 1. Lack of knowledge regarding on the seriousness of the health threat of STI. 2. Lack of interest and curiousness on the topic since never been experience sexual intercourse and never been sexually active. 3. Do not have enough time to take the topic/issue seriously due to other. 4. The subject was never been discussed in the lecture. 5. Parental guidance and culture influences. 6. Influences of media like television and internet. 7. Educational background 8. Peer influences 83 39 85 90 73 90 6 8 5 2.5 7 2.5 f 92 87 Rank 1 4
For Table 3, factors affecting knowledge level of student nurses from level 2, 3 and 4 were ranked and from the greatest to least factor that could affect the level of understanding of the students regarding STI. The primary factor which most of the students believed to affect knowledge level on STI was lack of knowledge regarding on the seriousness of the health threat of STI. Second on the rank were influences of media like television and internet and peer influences. This was followed by lack of interest and curiousness on the topic since they never have experienced sexual intercourse and never been sexually active
Saludamay Vol. IV No.1 65
was one of the factors. Next were parental guidance and culture influences. Then, the sixth factor was not having enough time to take the topic/issue seriously due to other reasons. Ranked seventh was educational background. Last in the rank was the subject was never been discussed in the lecture. Proposed Measures Based on observations and findings, proposed measures to solve the existing problems were identified and enumerated. 1. Make pamphlets, flyers or brochures regarding STIs and distribute them to fellow student nurses. 2. Create a group or organization in the college which will promote programs against STIs and which will provide information or counselling about it. 3. Impart to the clinical instructors the insufficiencies on the knowledge of the students on STIs. 4. Conduct a mini seminar and an open-forum and make the student nurses as the primary participants. 5. Share the findings of the study to fellow student nurses, for them to become aware and to elicit their cooperation to solve the identified problems. 6. Include in the bulletin board of the college trivia about STIs. 7. Make slogan on promoting its prevention. Recommendations Based on the foregoing findings and conclusions, the following recommendations are formulated: 4BSN: 1. As part of the requirements in their subject in leadership and management, the 4th year students could conduct a seminar focusing on STIs. Through this, they could enrich their knowledge about the infection and could enlighten their minds about some misconceptions by having an open-forum with the speaker after discussing the topics. 2. Clinical Instructors should explain further and delve deeper into the topic for the students to learn not only the STIs but also their prevention, transmission, complications and nursing interventions for the venereal diseases. 3. Since most of the fourth year students spend their time in the clinical area for their duty days and completion of cases, they can have a small discussion in their group. This could be facilitated by their clinical instructors to know what the students already knew and supply their deficiency about the topics. 4. It should be cleared to them that abstinence is still the best in the prevention of teen-
66 aquinas university of legazpi
age pregnancy and in transmission of STIs. 3BSN: 1. Clinical instructors should have a thorough discussion of STIs not only inside the room but also in the clinical area especially when they encountered person infected with the disease. 2. To enhance their knowledge, clinical instructors should give the students activities such as case studies and journal readings about STIs. To check their knowledge, clinical instructors should read the students output and address whatever concerns they have encountered as they checked the content of the writings of the students. 3. It should be clarified to them that abstinence until marriage is the most effective means not only in prevention of teenage pregnancy but also in the transmission of STIs. 2BSN: 1. Since this topic was not yet covered by their subjects or it could be one of the topics but was not fully discussed, clinical instructors should supply the inadequacies of the students not only inside the room but also in the clinical area. They should also encourage the students to attend more seminars and discussions about the topics on STIs to enhance their knowledge. 2. Part of gaining knowledge was research and reporting. Clinical instructors could assign a topic about STIs for every student in the class to research about and to impart knowledge to others through reporting or trivia sharing as one part of their discussions which may be related to STI and which are under their curriculum. 3. Most of the students from second year were given a chance to have a duty in the community especially in the health center of every barangay where they can utilize the materials such as brochures, pamphlets, audio-visuals and also observe the patients infected with STI who consulted in the social hygiene unit. For levels 2-4: 1. In coordination with the office of College of Nursing and Health Sciences, the college student council should conduct an annual seminar regarding STI to be able to supplement their knowledge on the said topic. 2. College of Nursing guidance counsellors should encourage the student to approach them and raise their concerns on STIs. 3. Clinical Instructors should explain further the topics on STIs, to learn the prevention, transmission, complications and nursing interventions of the venereal diseases. 4. The community should also be involved in imparting knowledge on STIs. The health centers should conduct lectures on the topic not only to the adults but also to adolescents
Saludamay Vol. IV No.1 67
and young adults so that they will have idea about STIs. 5. Parents of every family should guide their children in watching television and surfing the net so that any sensitive issues regarding sex and the diseases that can be acquired could be explained by them in a simple and comprehensible manner. 6. Giving flyers and pamphlets are also ways to address the lack of knowledge on STIs of nursing students. 7. Involvement of clinics not just in the vicinity of the schools but also outside the schools could also help in imparting knowledge and clarifying misconceptions through brochures, pamphlets, journals and also health teachings of the health care personnel to clients. Areas for Further Study 1. Attitude of Student Nurses in Caring of Patients Infected with Sexually Transmitted Infection in Aquinas University Hospital. 2. A Study on the Competency of Clinical Instructors of Aquinas University in Teaching Sexually Transmitted Infections to Student Nurses. 3. Effectiveness of Nursing Interventions of Aquinian Student Nurses in Patients Infected with Sexually Transmitted Infection in Aquinas University of Legazpi.
68 aquinas university of legazpi
STRESSORS IN THE WORKPLACE, THEIR EFFECTS TO THE FACULTY MEMBERS OF AQUINAS UNIVERSITY OF LEGAZPI
Catherine R. Vargas, RN, MAN
Abstract
Work-related stress is said to be experienced when the demands from the work environment exceed the employees ability to cope with or control them (European Agency, 2000). In the teaching profession, stress is recognized as the number one health problem among teachers. It is described as the experience by a teacher of unpleasant, negative emotions, such as anger, anxiety, tension, frustration or depression, resulting from some aspect of their work as a teacher. Studies have consistently concluded that teaching is one of the most stressful occupations, and that a significant number of teachers, perhaps even a majority, are affected by work-related stress. It has been acknowledged that managing stress in the workplace is a collective effort of the individual and the organization. More so, nursing plays an immense role in assisting individuals to cope with stress and maintain or achieve wellness. This study was conducted with the primary aim of advancing recognition of teacher stress in Aquinas University. Such awareness shall be the key step in promoting a working environment that supports wellness among the faculty members by addressing stress at the individual and organizational levels. Specifically, the study strived to answer the following questions: 1) What stressors are encountered by the faculty members of Aquinas University of Legazpi in the workplace?, 2) What are the effects of these stressors along physiological and psychological aspects and job performance of the faculty members?, 3) What individual strategies can be recommended to cope with these stressors?, and 4) What administrative support can be offered to the faculty member who encountered
Saludamay Vol. IV No.1 69
stressors?. From the findings of the study, the researcher recommended a stress management action-plan per college which outlined nursing interventions. This study utilized a descriptive-survey type of research, using a questionnaire to explore the sources of stress in the workplace along demands, management, support, role and control, working conditions and relationships; the effects of stress in terms of the physiological and psychological aspects and job performance of the respondents; the individual coping strategies and the recommended administrative support to manage encountered stress. The researcher conducted interviews to gather their actual experiences per stressor. A total of 98 faculty members served as respondents. They are teaching in the different colleges of Aquinas University of Legazpi for the Second Semester of SY 2009-2010, with at least 21 units or 24 teaching hours per week on either full-time or part-time status. Statistical treatment included frequency distribution, percentage, and weighted mean. The salient findings of the study were: 1) Sources of stress in the workplace along job demands included working on school matters in the evening or on weekends, handling too many lectures, demands and requirements in graduate studies, unreasonable deadlines and time pressures which were too often imposed and too many after school meetings. Along management, stressors were unfair practices of managers, lack of effective leader in the department, managers who could not effectively handle conflicts, a demanding and bossy immediate supervisor and fast turn over of administrator in the department. Along support, these were poor pay, lack of benefits, lack of support on faculty development, worries about job security and lack of mentors. Along role and control, stressors were new roles were required without appropriate training, required to teach outside areas of competence and training, lack of consultation in the school and lack of participation in decision-making. Along working conditions, the respondents identified far classroom locations, poor classroom ventilation, lack of facilities, too big class sizes, excessive noise levels in the working environment and poor lighting conditions as sources of stress. Along relationships, the students lack of motivation, students misbehavior in the classroom and students lack of respect for teachers were the stressors. 2) Faculty members manifested
70 aquinas university of legazpi
stress physiologically by often experiencing fatigue/body weakness; and psychologically by often experiencing anxiety and irritability. Accordingly, stress affected job performance as shown by poor performance and productivity though only seldom in occurrence. 3) Individual coping strategies suggested were attending stress awareness programs, discussing concerns with management, time management and priority setting, prayer, discussing concerns with co-workers, taking a day off, humor, sleep and music therapy. 4) To assist faculty members who were encountering stress, administrative support such as wellness programs, in-service trainings, stress awareness sessions and improving organizational communication were recommended. In response to the findings of the study, a stress management action-plan was designed to address the sources and effects of stress with the definitive goal of promoting wellness among the faculty members. The action-plan highlighted nursing interventions for identified effects of stress. Some of the recommended nursing interventions included encouraging healthy lifestyle (proper nutrition, adequate rest and sleep, regular exercise), assisting in relaxation techniques, positive visualization, allowing verbalization of feelings, encouraging expanding support system and advising seeking professional help when needed among others. The following conclusions were derived: 1) The faculty members of Aquinas University of Legazpi for the Second Semester of SY 2009-2010 encountered several stressors in the University along the six key areas. In general, the different colleges of the University experienced similar sources of stress, though there were some stressors that were distinct to a certain college. The College of Business Administration (BA) appeared to be the college with the most number of issues and concerns in terms of the six key areas. 2) Stress of faculty members was manifested physiologically and psychologically. It also affected job performance. The colleges showed differences in manifestations of stress as well as the frequency of such manifestations with BA showing the most and frequent manifestations. 3) A critical factor in managing occupational stress was the use of individual coping strategies. Faculty members of the University recommended varied strategies in managing stress. Most likely, these recommendations were the strategies of the faculty members in effectively managing occupational stress. 4) The administration plays a significant role in stress management. The faculty members certainly required the
Saludamay Vol. IV No.1 71
support of the administration in managing encountered stress in the workplace. In the light of the findings and conclusions, the researcher recommends the following: At the individual level, faculty members should play an active role in managing stress by indulging in health promotional activities, undergoing regular physical and psychological examinations and having individual coping strategies for stress management, among others. At the organizational level, 1) University Administrators, specifically the Deans and the Human Resource Management Office (HRMO) to consider the findings of this study and accept that stress is an organizational issue which should be tackled. Main emphasis should be on reducing or eliminating hazards and not solely on stress management courses or training. 2) The HRMO should consider establishing an organizationally supported stress management program that would also include provisions for in-service trainings and wellness programs as recommended by the respondents as well as provision for occupational health services and counseling services for those who feel stressed, and 3) Employee unions should have a better understanding and an increased capacity in tackling stress in the University along with the other stakeholders. At the professional nurse level, their responsibility would encompass stress management initiatives at the individual and organizational levels. At the heart of this role is assisting faculty members to manage stress throughout the three levels of prevention namely: 1) Primary prevention, 2) Secondary prevention, and 3) Tertiary prevention. Nursing roles in stress management at the individual levels can best focus on promoting primary prevention through health education centered on leading a healthy lifestyle. Nursing role at the secondary and tertiary prevention is to help individuals achieve wellness and optimal level of functioning. At the center of organizational partnership in stress management comes the critical participation of the College of Nursing and Health Sciences in carrying out proactive stress management initiatives for the benefit of the faculty members including the entire workforce of the University.
72 aquinas university of legazpi
PHENOMENOLOGY OF MALE SAME-SEX PRACTICES AND THEIR IMPLICATIONS ON HEALTH
Robert J. Jamisola, RN, MAN
Abstract
The Philippines as a predominantly Christian country treats gays or the third sex, liberally. Gays in the Philippines are highly tolerated amidst the machismo culture. Its a paradox between two realities making it hard for an observer to say if Filipino society really accepts or still rejects having gays in the family. There are numbers of same-sex practices associated with homosexual men or in general, categorized as Men Who Have Sex with Men (MSM). For many, such practices are way beyond expected norms and place MSM at risk for contracting myriad of diseases that can be contagious and infectious, and, such practices are deemed immoral and unethical. With the main objective of delving into the phenomenon of same-sex practices and theirimplications on health, this study sought answers to the following questions: 1) What are Men Who Have Sex with Mens notions of self and identity? 2) What practices are considered homosexual in nature? 3) What are the implications on the health of those who have same-sex practices along the following dimensions: a) physical b) emotional-cognitive c) social-cultural and d) spiritual? And 4) What health care model may be recommended to Men Who Have Sex with Men? This study was a phenomenology type of qualitative research. It made use of a guidequestion tool for the interview process for the purpose of capturing the lived same-sexexperiences and practices of the participants and the meanings things have in their experiences. It also has a purpose of delving into the reactions, feelings and insights of the participants who
Saludamay Vol. IV No.1 73
represent three major fields of health, education and business and who are all residing in Albay. Based on the data gathered, the study has the following salient findings: 1) Men WhoHave Sex with Mens (MSMs) early childhood experiences gave them the notion and feeling of somewhat different. The development of ones personality and identity was shaped by various factors, most important was the family. 2) Common practices that were homosexual in nature include oral intercourse, mutual oral intercourse or 69, anal intercourse, and rimming. On some occasions, MSM also engaged in fondling, kissing, necking, petting, and licking. These practices were considered sine quibus non among them. MSM may have a steady partner or a chance encounter partner only. 3) There were wide arrays of implications of same-sex practices on health. 3.a) Implications on physical health could be devastating from simple fissures and lacerations to contracting sexually transmitted infection and parasitic infection most especially if a homosexual is involved with multiple sex partners. Safe-sex considerations are routinely integrated into sexual practices but in a way that leaves a room for considerable risk factors. 3.b) Implications on emotional-cognitive health included depression that may lead to suicidal tendencies and self-inflicted pain. 3.c) Harassment, discriminations, and stereotyping were the implications on social-cultural health as homosexuality is not widely accepted although its existence is never negated. 3.d) Spiritual health was enhanced through a homosexuals strong belief in Supreme Being and integrated their religion within the context of their sexuality. 4) The resiliency of an individual to handle adversities varied depending upon their coping mechanism. Addressing the health needs of MSM to become resilient was not yet developed in the past and a health care model for them, the Jamisola MSM Health Resilient Model is recommended. Based on the findings the following conclusions were derived: 1) Men Who Have Sex with Men (MSM) had different notions about their selves and identity from being discreet, to acknowledging themselves completely as a woman, and to being openly gay. 2) Same-sex practices associated with homosexuals primarily included oral intercourse, mutual oral intercourse or 69, anal intercourse, rimming, fondling, kissing, necking, petting, and licking. 3) Implications of same-sex practices on physical health included potential risks for acquiring a wide array of STIs, sore
74 aquinas university of legazpi
throat, anal lacerations and fissures, and acquiring parasitic infection from bowel. Along emotional-cognitive health, depression ranks the most common among MSMs in a homosexual relationship. Complimentary relationship between a man and a woman was not satisfied by same-sex relationship. Along social-cultural health, calling of names or stereotyping such as bakla was the most common among MSM, and along spiritual health, the need to divulge and confess arise among homosexuals to integrate spirituality with their sexuality. 4) Adversities in life were common to all but may present a different perspective among homosexuals. A health model for homosexual is extremely important, most especially to those who were considered promiscuous in same-sex practices. The focus of the health model should encompass the dimensions of health namely physical, emotional-cognitive, social-cultural and spiritual. In the light of the findings of the study, the following are recommended: 1) The Department of Health should consider the findings of the study and acknowledge the needs of homosexual members of the society, to support and formulate a program specially intended for MSMs, promiscuous in their homosexual encounters, practices and relationships. 2) Health practitioners and health-related professionals should ensure the delivery of services for MSMs, acknowledging their health needs and situation with wider understanding. Awareness on the implications of same-sex practices should lay down the foundation in formulating health activities and health education and information campaign materials. 3) Concept on homosexuality, gender sensitivity, and sexual orientation should become one of the thrust of a schools guidance program. Guidance program should incorporate therapeutic interventions for these homosexuals who are in a state of fear of coming-out. 4) The political parties and law makers who are within the social conservative political spectrum must recognize homosexual rights, and provide full support for self-help groups and organizations for lesbians, gays and transgenders (LGBT) with thrusts toward human rights and equality. 5) The family as major socializing agent should be made part of the schools sex education program. 6) Provisions for annual gathering of members of LGBT in the Philippines should be done to enhance the extent of awareness on major issues concerning homosexuality and related practices. 7) Understanding the situation of homosexual members of the church as part of community of faith is integral in strengthening their relationship with God.
Saludamay Vol. IV No.1 75
76 aquinas university of legazpi
Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Self-Guided EMDR Therapy Workbook Healing From Anxiety, Anger, Stress, Depression, PTSD Emotional Trauma (Katherine Andler)Documento54 pagineSelf-Guided EMDR Therapy Workbook Healing From Anxiety, Anger, Stress, Depression, PTSD Emotional Trauma (Katherine Andler)Danielle W100% (7)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Dementia Treatment EssayDocumento8 pagineDementia Treatment EssayJay100% (1)
- Encyclopedia of Dinosaurs and Prehistoric LifeDocumento378 pagineEncyclopedia of Dinosaurs and Prehistoric LifeJ Alberto Lucas75% (12)
- 2013 Syllabus Legal and Judicial EthicsDocumento5 pagine2013 Syllabus Legal and Judicial EthicsKathleen Catubay SamsonNessuna valutazione finora
- Dost 2017Documento29 pagineDost 2017crisjavaNessuna valutazione finora
- No101 17 IP PhilippinesDocumento5 pagineNo101 17 IP PhilippinesAlosNessuna valutazione finora
- RPN Qualitative Presentation 2.11.20Documento34 pagineRPN Qualitative Presentation 2.11.20crisjavaNessuna valutazione finora
- P2226 BAR - Agenda For WebDocumento8 pagineP2226 BAR - Agenda For WebcrisjavaNessuna valutazione finora
- Divestive SystemDocumento69 pagineDivestive SystemCristina Mihaela BasalicNessuna valutazione finora
- Special Penal LawsffffffssDocumento195 pagineSpecial Penal LawsffffffsscrisjavaNessuna valutazione finora
- Vol 17 P 1Documento28 pagineVol 17 P 1crisjavaNessuna valutazione finora
- Vol 17 P 1Documento28 pagineVol 17 P 1crisjavaNessuna valutazione finora
- Yorac Law Firm Announcement - UPDocumento1 paginaYorac Law Firm Announcement - UPcrisjavaNessuna valutazione finora
- Yorac Law Firm Announcement - UPDocumento1 paginaYorac Law Firm Announcement - UPcrisjavaNessuna valutazione finora
- Wipo Smes Kul 06 WWW 68913Documento55 pagineWipo Smes Kul 06 WWW 68913Ankit SinghNessuna valutazione finora
- UP 2011 Crim TipsDocumento3 pagineUP 2011 Crim TipscrisjavaNessuna valutazione finora
- ActionDocumento95 pagineActionNasrudinSuaibNessuna valutazione finora
- Medallion Vs TexasDocumento4 pagineMedallion Vs TexasSuiNessuna valutazione finora
- Team2 - Rizal's Life in Paris and GermanyDocumento26 pagineTeam2 - Rizal's Life in Paris and GermanycrisjavaNessuna valutazione finora
- Illegal Logging Us-DojDocumento58 pagineIllegal Logging Us-DojcrisjavaNessuna valutazione finora
- Module 3Documento1 paginaModule 3crisjavaNessuna valutazione finora
- Re-Orientation Seminar On Policies and Updates From CHEd, PRC and BUDocumento5 pagineRe-Orientation Seminar On Policies and Updates From CHEd, PRC and BUcrisjavaNessuna valutazione finora
- Role of PHE ReportDocumento22 pagineRole of PHE ReportcrisjavaNessuna valutazione finora
- Vol 17 P 1Documento28 pagineVol 17 P 1crisjavaNessuna valutazione finora
- Philippine Law and Society ReviewDocumento164 paginePhilippine Law and Society ReviewSen CabahugNessuna valutazione finora
- Module 3Documento1 paginaModule 3crisjavaNessuna valutazione finora
- CBCP AddressDocumento1 paginaCBCP AddresscrisjavaNessuna valutazione finora
- Vol 17 P 1Documento28 pagineVol 17 P 1crisjavaNessuna valutazione finora
- L L S L: Abor AW AND Ocial EgislationDocumento8 pagineL L S L: Abor AW AND Ocial EgislationMarie CecileNessuna valutazione finora
- Sampling OUDocumento47 pagineSampling OUcrisjavaNessuna valutazione finora
- Mercantile Law 2013 October Bar ExamsDocumento17 pagineMercantile Law 2013 October Bar ExamsNeil RiveraNessuna valutazione finora
- Faculty Marked Assignment No. 4: MM 214 Corporate Planning and Project ManagementDocumento2 pagineFaculty Marked Assignment No. 4: MM 214 Corporate Planning and Project ManagementcrisjavaNessuna valutazione finora
- Depression Anxiety Stress Scales DASS3481Documento1 paginaDepression Anxiety Stress Scales DASS3481Huda NoorNessuna valutazione finora
- Case Study Mental Health StudentDocumento5 pagineCase Study Mental Health StudentmeNessuna valutazione finora
- Evaluation InstrumentsDocumento2 pagineEvaluation InstrumentsAnonymous 1HGqtl7Nessuna valutazione finora
- The Effect of DBT On AutismDocumento11 pagineThe Effect of DBT On AutismJinny DavisNessuna valutazione finora
- The Psychiatric Comorbidity of Epilepsy PDFDocumento14 pagineThe Psychiatric Comorbidity of Epilepsy PDFTanjung E SumekarNessuna valutazione finora
- MAYSI2 AdminstrationReferral Protocol ManualFinal2014Documento20 pagineMAYSI2 AdminstrationReferral Protocol ManualFinal20147 MNT100% (1)
- Rapid Mood Screener (RMS) : Abbvie MedicalDocumento2 pagineRapid Mood Screener (RMS) : Abbvie MedicalebadhNessuna valutazione finora
- Research Proposal s2Documento2 pagineResearch Proposal s2api-451543560Nessuna valutazione finora
- Disorders: By: Nur Hanisah Binti ZainorenDocumento53 pagineDisorders: By: Nur Hanisah Binti ZainorenJœnríčk AzueloNessuna valutazione finora
- Stalking Behaviors in Students With Autism Spectrum DisorderDocumento12 pagineStalking Behaviors in Students With Autism Spectrum Disorderapi-385079933Nessuna valutazione finora
- Generalized Anxiety Disorder: Clinical Practice Guidelines Management of Anxiety DisordersDocumento6 pagineGeneralized Anxiety Disorder: Clinical Practice Guidelines Management of Anxiety DisordersDaciana DumitrescuNessuna valutazione finora
- Sanchez Sam Per 2009Documento13 pagineSanchez Sam Per 2009ClaudiaGárateHenríquezNessuna valutazione finora
- Placebo Response in Depression: A Perspective For Clinical PracticeDocumento2 paginePlacebo Response in Depression: A Perspective For Clinical PracticeashfaqamarNessuna valutazione finora
- 4.reviewed 2018-ADHD IAP TOT On NDD National Guidelines ModuleDocumento56 pagine4.reviewed 2018-ADHD IAP TOT On NDD National Guidelines Modulekawaljit000Nessuna valutazione finora
- Schizoid Personality DisorderDocumento4 pagineSchizoid Personality DisorderRajeev ValunjkarNessuna valutazione finora
- Negative Punishment and Its EffectsDocumento2 pagineNegative Punishment and Its EffectsSea BPNessuna valutazione finora
- Brief CBT: Gladys S. Canillo, LPT, RPM, RpsyDocumento28 pagineBrief CBT: Gladys S. Canillo, LPT, RPM, Rpsygladys canilloNessuna valutazione finora
- PA y Depresión en Nepal 2017Documento8 paginePA y Depresión en Nepal 2017Alfredo PérezNessuna valutazione finora
- Challenges Related To Educational Interpreting For Students Who Are Deaf With DisabilitiesDocumento12 pagineChallenges Related To Educational Interpreting For Students Who Are Deaf With DisabilitiesVictor Rivera100% (1)
- Psychosis and NeurosisDocumento4 paginePsychosis and NeurosisYashwanth VbNessuna valutazione finora
- Thesis Statement Anxiety DisorderDocumento8 pagineThesis Statement Anxiety Disorderanneryssanchezpaterson100% (2)
- Suicide Factors: UNSAFE or SAFER?: Risk Factors Protective FactorsDocumento2 pagineSuicide Factors: UNSAFE or SAFER?: Risk Factors Protective FactorsLaura CristinaNessuna valutazione finora
- Worry Models - ReviewDocumento14 pagineWorry Models - ReviewSibealNessuna valutazione finora
- AripripazoleDocumento13 pagineAripripazoleOneng IfayaniNessuna valutazione finora
- PPDGJ 3 PDFDocumento279 paginePPDGJ 3 PDFtri ummiNessuna valutazione finora
- Group 8. Eating DisordersDocumento3 pagineGroup 8. Eating Disordersanon_619050222Nessuna valutazione finora
- The Early Identification of Autism: The Checklist For Autism in Toddlers (CHAT)Documento25 pagineThe Early Identification of Autism: The Checklist For Autism in Toddlers (CHAT)feregodocNessuna valutazione finora
- Rational Emotive Behavioral Therapy: Josemon P.George V Mba (PT)Documento27 pagineRational Emotive Behavioral Therapy: Josemon P.George V Mba (PT)Josemon George ParanilamNessuna valutazione finora