Potrebbero piacerti anche
- AppendectomyDocumento4 pagineAppendectomyKyre LandinginNessuna valutazione finora
- Jaundice Case StudyDocumento5 pagineJaundice Case StudyUday KumarNessuna valutazione finora
- NCP Acute PainDocumento1 paginaNCP Acute PainBianca Freya Porral100% (2)
- Case StudyDocumento20 pagineCase Studypadmja4purohitNessuna valutazione finora
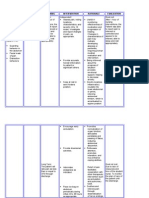
- Assessment Diagnosis Objectives Nursing Interventions Rationale Evaluation S STO After 45 DX: STO Goal FullyDocumento5 pagineAssessment Diagnosis Objectives Nursing Interventions Rationale Evaluation S STO After 45 DX: STO Goal FullyMar OrdanzaNessuna valutazione finora
- NSVD Patient Sleep IssuesDocumento3 pagineNSVD Patient Sleep IssuesAlma Gobaleza100% (1)
- Appendectomy NCPDocumento2 pagineAppendectomy NCPQueency Vanguardia0% (1)
- Student Nurses' Appendectomy Care PlanDocumento2 pagineStudent Nurses' Appendectomy Care PlanFernandez LeaNessuna valutazione finora
- AppendectomyDocumento2 pagineAppendectomyJoshua Triumfante De Vera IIINessuna valutazione finora
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocumento2 pagineAssessment Diagnosis Planning Intervention Rationale EvaluationRomeo Avecilla CabralNessuna valutazione finora
- NCP 28Documento9 pagineNCP 28Leanne Joie Lozano100% (1)
- 7 NCPDocumento7 pagine7 NCPVina EmpialesNessuna valutazione finora
- NCPDocumento11 pagineNCPJaziel Remo100% (1)
- NCP HemothoraxDocumento3 pagineNCP HemothoraxMichael John F. NatividadNessuna valutazione finora
- Assessmen T Nursing Diagno SIS Analysis AND Interpretat ION Planning Nursing Interventi ONS Rationale Evaluati ON Subjective: GoalDocumento5 pagineAssessmen T Nursing Diagno SIS Analysis AND Interpretat ION Planning Nursing Interventi ONS Rationale Evaluati ON Subjective: GoalKatherine_Chyr_9112Nessuna valutazione finora
- Nursing Management of CVA and NIDDMDocumento12 pagineNursing Management of CVA and NIDDMKaloy KamaoNessuna valutazione finora
- Assessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationDocumento3 pagineAssessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationCrissa AngelNessuna valutazione finora
- NCPDocumento5 pagineNCProxybabes100% (3)
- NURSING CARE PLANSDocumento9 pagineNURSING CARE PLANSAlfadz AsakilNessuna valutazione finora
- NCPDocumento10 pagineNCPMack Jhed AnarconNessuna valutazione finora
- Pain Care PlanDocumento18 paginePain Care Planjordanw0613Nessuna valutazione finora
- NCP Cholecystectomy RevisedDocumento7 pagineNCP Cholecystectomy RevisedMariquita Buenafe100% (4)
- Cholecystitis NCPDocumento4 pagineCholecystitis NCPdark-canales33% (3)
- IUFDDocumento13 pagineIUFDChristopher Lontoc0% (1)
- Control Post-Surgical Pain and Improve BreathingDocumento12 pagineControl Post-Surgical Pain and Improve BreathingMayraPagan-Carmenatty100% (1)
- Post-Op Pain Management Nursing Care PlanDocumento7 paginePost-Op Pain Management Nursing Care Planمالك مناصرةNessuna valutazione finora
- NCP - CruzDocumento2 pagineNCP - CruzAlvin CruzNessuna valutazione finora
- Acute Pain..Documento2 pagineAcute Pain..Melody Kaye MonsantoNessuna valutazione finora
- Askep Post Operatif: Kelompok 3Documento9 pagineAskep Post Operatif: Kelompok 3Rara Suci RhamadhanNessuna valutazione finora
- Acute Chest Pain ManagementDocumento2 pagineAcute Chest Pain ManagementErickson Caisido GarciaNessuna valutazione finora
- Simulated Care (Bajado)Documento6 pagineSimulated Care (Bajado)Ma. Ferimi Gleam BajadoNessuna valutazione finora
- Au NCPDocumento1 paginaAu NCPCarlo Medina MagnoNessuna valutazione finora
- Case Study 01.2.17.00599 IntervensionDocumento3 pagineCase Study 01.2.17.00599 IntervensionBorn OfdeathNessuna valutazione finora
- Preop & Postop Nursing InterventionsDocumento8 paginePreop & Postop Nursing InterventionsLizethNessuna valutazione finora
- Cva NCPDocumento2 pagineCva NCPAkima Mulok0% (1)
- Me Nursing Care Plan in AppendicitisDocumento2 pagineMe Nursing Care Plan in AppendicitiskathrynmarielNessuna valutazione finora
- Super Final NCPDocumento16 pagineSuper Final NCPNessaly Jane PrestoNessuna valutazione finora
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation IndependentDocumento4 pagineAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation IndependentJoseph Rodney de LeonNessuna valutazione finora
- NCP CholeDocumento8 pagineNCP CholeAndrewAlvinTemploNessuna valutazione finora
- Clinical Prep 2Documento9 pagineClinical Prep 2Colin FraleyNessuna valutazione finora
- NCP Inc.Documento2 pagineNCP Inc.Franklin A. Salaum III100% (1)
- Nursing Care Plan FinalDocumento4 pagineNursing Care Plan FinalSheana TmplNessuna valutazione finora
- Nursing Care PlanDocumento9 pagineNursing Care PlanjmichaelaNessuna valutazione finora
- NCP CholangitisDocumento4 pagineNCP CholangitisJanica C. BayauaNessuna valutazione finora
- NCPDocumento7 pagineNCPCamille Evan YmasaNessuna valutazione finora
- R.O. Appendicitis.: Nursing Care Plan (NCP)Documento2 pagineR.O. Appendicitis.: Nursing Care Plan (NCP)Karen Joy ItoNessuna valutazione finora
- PROTOCOL FOR BED TO CHAIR AMBULATIONDocumento14 paginePROTOCOL FOR BED TO CHAIR AMBULATIONMuhammad asif samiNessuna valutazione finora
- Simulated Care (Bajado)Documento6 pagineSimulated Care (Bajado)Ma. Ferimi Gleam BajadoNessuna valutazione finora
- Nursing care plan for pain managementDocumento4 pagineNursing care plan for pain managementSugar Capule - ManuelNessuna valutazione finora
- NCP TonsilitisDocumento11 pagineNCP TonsilitisGra Cie50% (6)
- Process of Healthcare For Hip-Surgery PatientsDocumento6 pagineProcess of Healthcare For Hip-Surgery PatientsJosipaIvaMarićNessuna valutazione finora
- NCP Pain - ArthroDocumento6 pagineNCP Pain - ArthroKDnurseboyNessuna valutazione finora
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANODa EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONessuna valutazione finora
- Differentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)Da EverandDifferentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)Nessuna valutazione finora
- Local Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)Da EverandLocal Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)Nessuna valutazione finora
- Holistic Home Remedies for Acute Low Back Pain: Incorporating Stretching and the McKenzie MethodDa EverandHolistic Home Remedies for Acute Low Back Pain: Incorporating Stretching and the McKenzie MethodNessuna valutazione finora
- If they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.Da EverandIf they could talk about walking again: Canine Cruciate Surgery Rehabilitation Program: A 10 week detailed program of specific approaches, exercises, massage, and restoring balance to get the best results after your pet has undergone surgery for cruciate ligament repair. Tracking sheets for each week.Nessuna valutazione finora
- 21st Century Thinking About Leadership & Management - Balsarza, KrishnaDocumento3 pagine21st Century Thinking About Leadership & Management - Balsarza, KrishnaKrishna BalsarzaNessuna valutazione finora
- CANCERPPNSGDocumento79 pagineCANCERPPNSGKrishna BalsarzaNessuna valutazione finora
- KBBDocumento71 pagineKBBKrishna BalsarzaNessuna valutazione finora
- Top 10 Herbal Medicines for Common AilmentsDocumento8 pagineTop 10 Herbal Medicines for Common AilmentsKrishna BalsarzaNessuna valutazione finora
- Cerebrovascular Disease Case StudyDocumento9 pagineCerebrovascular Disease Case StudyKrishna BalsarzaNessuna valutazione finora
- TFNDocumento15 pagineTFNKrishna Balsarza100% (2)
- The 10 Most Common Emergency DrugsDocumento28 pagineThe 10 Most Common Emergency DrugsKrishna BalsarzaNessuna valutazione finora
- A Varicocele Is A Widening of The Veins Along The Cord That Holds Up A ManDocumento4 pagineA Varicocele Is A Widening of The Veins Along The Cord That Holds Up A ManKrishna BalsarzaNessuna valutazione finora
- Angina CpaDocumento52 pagineAngina CpaKrishna BalsarzaNessuna valutazione finora
- School Health Exam Summary of Grade 1-Dahlia: Abnormal Findings FrequencyDocumento1 paginaSchool Health Exam Summary of Grade 1-Dahlia: Abnormal Findings FrequencyKrishna BalsarzaNessuna valutazione finora
- Genward CPDocumento44 pagineGenward CPKrishna BalsarzaNessuna valutazione finora
- Prayer of ThanksgivingDocumento10 paginePrayer of ThanksgivingKrishna Balsarza100% (1)
- Berdel Report CHNDocumento10 pagineBerdel Report CHNKrishna BalsarzaNessuna valutazione finora
- Prevent HIV/AIDS: Abstain, Be Faithful, Use CondomsDocumento1 paginaPrevent HIV/AIDS: Abstain, Be Faithful, Use CondomsKrishna BalsarzaNessuna valutazione finora
- Experiences and Level of Satisfaction of The Patients in The Emergency DepartmentDocumento4 pagineExperiences and Level of Satisfaction of The Patients in The Emergency DepartmentKrishna BalsarzaNessuna valutazione finora
- PsycheDocumento4 paginePsycheKrishna BalsarzaNessuna valutazione finora
- 107 BESgfhDocumento14 pagine107 BESgfhKrishna BalsarzaNessuna valutazione finora
- Cagayan de Oro AIDS Council: "In Solidarity"Documento1 paginaCagayan de Oro AIDS Council: "In Solidarity"Krishna BalsarzaNessuna valutazione finora
- How To Conduct An InterviewDocumento5 pagineHow To Conduct An InterviewKrishna BalsarzaNessuna valutazione finora
- 11 BreastaDocumento22 pagine11 BreastaKrishna BalsarzaNessuna valutazione finora
- Actual NCP FinalDocumento9 pagineActual NCP FinalKrishna BalsarzaNessuna valutazione finora
- Balsarza, Krishna B. (N107a Quiz) October 4, 2013thDocumento17 pagineBalsarza, Krishna B. (N107a Quiz) October 4, 2013thKrishna BalsarzaNessuna valutazione finora
- DRUG STUDY DETAILS FOR CEFLEXIN, MULTIVITAMINS, AND FOLIC ACIDDocumento7 pagineDRUG STUDY DETAILS FOR CEFLEXIN, MULTIVITAMINS, AND FOLIC ACIDKrishna BalsarzaNessuna valutazione finora
- 2k11 Case Study JudDocumento24 pagine2k11 Case Study JudKrishna BalsarzaNessuna valutazione finora
- Personality DisorderDocumento48 paginePersonality DisorderKrishna BalsarzaNessuna valutazione finora
- Liceo de Cagayan UniversityDocumento23 pagineLiceo de Cagayan UniversityKrishna BalsarzaNessuna valutazione finora
- Mood Disord Ers: DO, RN, MA NDocumento39 pagineMood Disord Ers: DO, RN, MA NKrishna BalsarzaNessuna valutazione finora
- Step-By-Step Guide To Essay WritingDocumento14 pagineStep-By-Step Guide To Essay WritingKelpie Alejandria De OzNessuna valutazione finora
- Device Exp 2 Student ManualDocumento4 pagineDevice Exp 2 Student Manualgg ezNessuna valutazione finora
- FSW School of Education Lesson Plan Template: E1aa06cb3dd19a3efbc0/x73134?path JavascriptDocumento7 pagineFSW School of Education Lesson Plan Template: E1aa06cb3dd19a3efbc0/x73134?path Javascriptapi-594410643Nessuna valutazione finora
- Developing An Instructional Plan in ArtDocumento12 pagineDeveloping An Instructional Plan in ArtEunice FernandezNessuna valutazione finora
- Art 1780280905 PDFDocumento8 pagineArt 1780280905 PDFIesna NaNessuna valutazione finora
- Opportunity, Not Threat: Crypto AssetsDocumento9 pagineOpportunity, Not Threat: Crypto AssetsTrophy NcNessuna valutazione finora
- Inline check sieve removes foreign matterDocumento2 pagineInline check sieve removes foreign matterGreere Oana-NicoletaNessuna valutazione finora
- 2 - How To Create Business ValueDocumento16 pagine2 - How To Create Business ValueSorin GabrielNessuna valutazione finora
- 740LIDocumento13 pagine740LIm FaisalNessuna valutazione finora
- Oyo Rooms-Case StudyDocumento13 pagineOyo Rooms-Case StudySHAMIK SHETTY50% (4)
- Corporate Account: Department of Commerce Doctor Harisingh Gour Vishwavidyalaya (A Central University) SAGAR (M.P.)Documento6 pagineCorporate Account: Department of Commerce Doctor Harisingh Gour Vishwavidyalaya (A Central University) SAGAR (M.P.)Aditya JainNessuna valutazione finora
- Comal ISD ReportDocumento26 pagineComal ISD ReportMariah MedinaNessuna valutazione finora
- Operational Risk Roll-OutDocumento17 pagineOperational Risk Roll-OutLee WerrellNessuna valutazione finora
- The Neteru Gods Goddesses of The Grand EnneadDocumento16 pagineThe Neteru Gods Goddesses of The Grand EnneadKirk Teasley100% (1)
- Will You Be There? Song ActivitiesDocumento3 pagineWill You Be There? Song ActivitieszelindaaNessuna valutazione finora
- Should Animals Be Banned From Circuses.Documento2 pagineShould Animals Be Banned From Circuses.Minh Nguyệt TrịnhNessuna valutazione finora
- College Wise Form Fillup Approved Status 2019Documento4 pagineCollege Wise Form Fillup Approved Status 2019Dinesh PradhanNessuna valutazione finora
- Independent Study of Middletown Police DepartmentDocumento96 pagineIndependent Study of Middletown Police DepartmentBarbara MillerNessuna valutazione finora
- Apple NotesDocumento3 pagineApple NotesKrishna Mohan ChennareddyNessuna valutazione finora
- PHEI Yield Curve: Daily Fair Price & Yield Indonesia Government Securities November 2, 2020Documento3 paginePHEI Yield Curve: Daily Fair Price & Yield Indonesia Government Securities November 2, 2020Nope Nope NopeNessuna valutazione finora
- A Review On Translation Strategies of Little Prince' by Ahmad Shamlou and Abolhasan NajafiDocumento9 pagineA Review On Translation Strategies of Little Prince' by Ahmad Shamlou and Abolhasan Najafiinfo3814Nessuna valutazione finora
- Get 1. Verb Gets, Getting Past Got Past Participle Got, GottenDocumento2 pagineGet 1. Verb Gets, Getting Past Got Past Participle Got, GottenOlga KardashNessuna valutazione finora
- MiQ Programmatic Media Intern RoleDocumento4 pagineMiQ Programmatic Media Intern Role124 SHAIL SINGHNessuna valutazione finora
- Factors Affecting English Speaking Skills of StudentsDocumento18 pagineFactors Affecting English Speaking Skills of StudentsRona Jane MirandaNessuna valutazione finora
- Toolkit:ALLCLEAR - SKYbrary Aviation SafetyDocumento3 pagineToolkit:ALLCLEAR - SKYbrary Aviation Safetybhartisingh0812Nessuna valutazione finora
- Popular Painters & Other Visionaries. Museo Del BarrioDocumento18 paginePopular Painters & Other Visionaries. Museo Del BarrioRenato MenezesNessuna valutazione finora
- Excel Keyboard Shortcuts MasterclassDocumento18 pagineExcel Keyboard Shortcuts MasterclassluinksNessuna valutazione finora
- DLL - Science 6 - Q3 - W3Documento6 pagineDLL - Science 6 - Q3 - W3AnatasukiNessuna valutazione finora
- 1 - Nature and Dev - Intl LawDocumento20 pagine1 - Nature and Dev - Intl Lawaditya singhNessuna valutazione finora
- The Awesome Life Force 1984Documento8 pagineThe Awesome Life Force 1984Roman PetersonNessuna valutazione finora