Potrebbero piacerti anche
- FamorcaDocumento137 pagineFamorcaStephanie Villanueva Advincula88% (32)
- 3 - Full Pulpotomy With Biodentine in Symptomatic Young Permanent Teeth With Carious Exposure PDFDocumento6 pagine3 - Full Pulpotomy With Biodentine in Symptomatic Young Permanent Teeth With Carious Exposure PDFAbdul Rahman AlmishhdanyNessuna valutazione finora
- Nursing Bullets 5Documento268 pagineNursing Bullets 5kate annNessuna valutazione finora
- Strickland PresentationDocumento1 paginaStrickland Presentationmariopi2495Nessuna valutazione finora
- Case 7 - Newborn With Respiratory DistressDocumento10 pagineCase 7 - Newborn With Respiratory DistressSue HuangNessuna valutazione finora
- Nursing the NeonateDa EverandNursing the NeonateMaggie MeeksNessuna valutazione finora
- Diseases of the Small Intestine in ChildhoodDa EverandDiseases of the Small Intestine in ChildhoodNessuna valutazione finora
- Respiratory Distress Management in NewbornDocumento5 pagineRespiratory Distress Management in Newbornagirl_9807100% (1)
- Division of Perinatology Department of Child Health Medical School University of Sumatera UtaraDocumento37 pagineDivision of Perinatology Department of Child Health Medical School University of Sumatera UtaraJosephine IrenaNessuna valutazione finora
- Gestational Age Related Problems of The Newborn: Carla Reinke, RN, MN, Arnp, CNMDocumento120 pagineGestational Age Related Problems of The Newborn: Carla Reinke, RN, MN, Arnp, CNMsulekhaanoobNessuna valutazione finora
- Keyes Neonatal Emergencies FinalDocumento108 pagineKeyes Neonatal Emergencies FinalthanyunNessuna valutazione finora
- Mechanical Ventilation of The Neonate Principles and StrategiesDocumento6 pagineMechanical Ventilation of The Neonate Principles and StrategiesKelly HoffmanNessuna valutazione finora
- Fetal Distress: Lin Qi de 2005.9.5Documento16 pagineFetal Distress: Lin Qi de 2005.9.5Rendy ChandraNessuna valutazione finora
- Neonatal Emergencies FinalDocumento90 pagineNeonatal Emergencies FinalDr Raseena VattamkandathilNessuna valutazione finora
- Neonates Maternal Drugs Which May Adversely Affect The Newborn BabyDocumento9 pagineNeonates Maternal Drugs Which May Adversely Affect The Newborn BabyAnonymousNessuna valutazione finora
- Neonatal SubgalealDocumento6 pagineNeonatal SubgalealIrenLayNessuna valutazione finora
- Neonatal PharmacologyDocumento61 pagineNeonatal PharmacologyAnaNessuna valutazione finora
- Neonatal SepsisDocumento20 pagineNeonatal SepsisJustine Nyangaresi100% (1)
- Follow-upoftheNICUPatient Medscape FormatDocumento65 pagineFollow-upoftheNICUPatient Medscape FormatJohn ParudaNessuna valutazione finora
- InTech-Neonatal Pneumonia PDFDocumento14 pagineInTech-Neonatal Pneumonia PDFClaudia PalominoNessuna valutazione finora
- Infection in NeonateDocumento28 pagineInfection in Neonateamel015Nessuna valutazione finora
- Case Study #1: HistoryDocumento39 pagineCase Study #1: Historyleonzon_ben442296Nessuna valutazione finora
- Infant and Young Child Feeding: Dr. Malik Shahnawaz AhmedDocumento71 pagineInfant and Young Child Feeding: Dr. Malik Shahnawaz AhmedRiyaz AhamedNessuna valutazione finora
- AARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry: 2013Documento10 pagineAARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry: 2013jvalenciagNessuna valutazione finora
- Neonatal ResuscitationDocumento138 pagineNeonatal ResuscitationAbcdeNessuna valutazione finora
- Sepsis Neonatal: Bryan L Ohning, MD, PHD, Clinical Associate Professor of Pediatrics, MedicalDocumento43 pagineSepsis Neonatal: Bryan L Ohning, MD, PHD, Clinical Associate Professor of Pediatrics, Medicalapi-19492580Nessuna valutazione finora
- Perinatal Asphyxia: Walter Otieno Consultant PaediatricianDocumento25 paginePerinatal Asphyxia: Walter Otieno Consultant PaediatricianMalueth AnguiNessuna valutazione finora
- NRP 2011 SummaryDocumento6 pagineNRP 2011 Summaryvanstar7Nessuna valutazione finora
- Neonatal Resuscitation. Advances in Training and PracticeDocumento10 pagineNeonatal Resuscitation. Advances in Training and PracticeFer45Nessuna valutazione finora
- Retinopathy of Prematurity: Aao ReadingDocumento34 pagineRetinopathy of Prematurity: Aao ReadingUNHAS OphthalmologyNessuna valutazione finora
- Golden Hours Management of High Risk Newborns - 2019Documento10 pagineGolden Hours Management of High Risk Newborns - 2019Suryadi LimardiNessuna valutazione finora
- 05 Polycythemia in The NewbornDocumento11 pagine05 Polycythemia in The NewbornMorales Eli PediatraNessuna valutazione finora
- Respiratory DistressDocumento11 pagineRespiratory DistressHina MasoodNessuna valutazione finora
- 9, Procedure of PICCDocumento9 pagine9, Procedure of PICCputriseptinaNessuna valutazione finora
- Physical Growth and Development: Different Aspects and AssessmentDocumento60 paginePhysical Growth and Development: Different Aspects and AssessmentDipti RamiNessuna valutazione finora
- Neonatal PneumoniaDocumento16 pagineNeonatal Pneumoniaelyuchan100% (1)
- Congenital Anomalies of Ureter BladderDocumento17 pagineCongenital Anomalies of Ureter BladderAfiq SabriNessuna valutazione finora
- Neonatal Ventilation PDFDocumento29 pagineNeonatal Ventilation PDFIsabella HosanaNessuna valutazione finora
- Prevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati UpadhyayDocumento42 paginePrevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati Upadhyaypranaya mallNessuna valutazione finora
- Delayed Vs Immediate Umbilical Cord ClampingDocumento37 pagineDelayed Vs Immediate Umbilical Cord ClampingAndi DeviriyantiNessuna valutazione finora
- Non-Cyanotic Congenital Heart Disease-UpDate 4-22-53Documento136 pagineNon-Cyanotic Congenital Heart Disease-UpDate 4-22-53getnusNessuna valutazione finora
- Adjunctive Therapies in Bronchopulmonary Dysplasia, NeoReview 2017Documento9 pagineAdjunctive Therapies in Bronchopulmonary Dysplasia, NeoReview 2017Edrei Lopez CNessuna valutazione finora
- Ductus Arteriosus Dependent Congenital Heart Disease: Amjad Kouatli MD. FAAP. FACCDocumento28 pagineDuctus Arteriosus Dependent Congenital Heart Disease: Amjad Kouatli MD. FAAP. FACCKartik KumarasamyNessuna valutazione finora
- PREMATURITYDocumento27 paginePREMATURITYHamizi MD HanapiahNessuna valutazione finora
- Assessment and Management of High Risk Neonates DrLawHN PDFDocumento45 pagineAssessment and Management of High Risk Neonates DrLawHN PDFShiva KarthikeyanNessuna valutazione finora
- Neonatal Asphyxia FinalDocumento20 pagineNeonatal Asphyxia FinalAtawna AtefNessuna valutazione finora
- Approach To Sick NeonateDocumento47 pagineApproach To Sick NeonateblitheleevsNessuna valutazione finora
- NRP ppt1Documento29 pagineNRP ppt1sumana BanerjeeNessuna valutazione finora
- Sepsis Management of Neonates With Suspected or Proven Early-Onset BacterialDocumento12 pagineSepsis Management of Neonates With Suspected or Proven Early-Onset BacterialAldo CancellaraNessuna valutazione finora
- Prematurity: DR - Azhar Hamza AlsaqyDocumento18 paginePrematurity: DR - Azhar Hamza AlsaqyChro MANessuna valutazione finora
- Neonatal JaundiceDocumento72 pagineNeonatal JaundiceThya HakimNessuna valutazione finora
- An Approach To Respiratory Distress in NewbornDocumento52 pagineAn Approach To Respiratory Distress in NewbornWira Febrisandi IrsanNessuna valutazione finora
- Theraputic Agent in NeonateDocumento7 pagineTheraputic Agent in Neonateد. محمد فريد الغنامNessuna valutazione finora
- Sickle Cell Anemia PowerpointDocumento29 pagineSickle Cell Anemia Powerpointapi-263353704100% (1)
- Low Birth Weight Baby and HyalineDocumento42 pagineLow Birth Weight Baby and Hyalineakhmad rizky subkiNessuna valutazione finora
- Enteral Feeding of The High Risk NewbornDocumento56 pagineEnteral Feeding of The High Risk NewbornSri SoelistijawatiNessuna valutazione finora
- Bleeding in A NeonateDocumento36 pagineBleeding in A NeonateDrBibek AgarwalNessuna valutazione finora
- Anemia of PrematurityDocumento14 pagineAnemia of PrematurityMariel HuamancayoNessuna valutazione finora
- A Neonate With Acute Kidney Injury: Case PresentationDocumento4 pagineA Neonate With Acute Kidney Injury: Case PresentationSahil DhamijaNessuna valutazione finora
- Respiratory Distress Syndrome: Islamic University Nursing CollegeDocumento21 pagineRespiratory Distress Syndrome: Islamic University Nursing Collegeyaumil agisnaNessuna valutazione finora
- Infants Diabetic MothersDocumento17 pagineInfants Diabetic MothersJaya PrabhaNessuna valutazione finora
- Disseminated Intravascular CoagulationDocumento16 pagineDisseminated Intravascular CoagulationDocRNNessuna valutazione finora
- Birth InjuriesDocumento11 pagineBirth Injuriesdapurna86Nessuna valutazione finora
- Citizens Charter: The Office of The Travancore-Cochin Medical CouncilsDocumento5 pagineCitizens Charter: The Office of The Travancore-Cochin Medical CouncilsabhivnairNessuna valutazione finora
- An Overview of The European Diploma of Anaesthesia and Intensive Care and of Other Important Initiatives of The European Society of AnaesthesiologyDocumento8 pagineAn Overview of The European Diploma of Anaesthesia and Intensive Care and of Other Important Initiatives of The European Society of AnaesthesiologyabhivnairNessuna valutazione finora
- Failure To Thrive Malnutrition Pediatric Outpatient Setting PDFDocumento11 pagineFailure To Thrive Malnutrition Pediatric Outpatient Setting PDFabhivnairNessuna valutazione finora
- AIIMS ProtocolsDocumento5 pagineAIIMS ProtocolsabhivnairNessuna valutazione finora
- LymphadenopathyDocumento2 pagineLymphadenopathyabhivnairNessuna valutazione finora
- Hypoglycemia in The Newborn: AIIMS-NICU Protocols 2010Documento13 pagineHypoglycemia in The Newborn: AIIMS-NICU Protocols 2010abhivnairNessuna valutazione finora
- Blood Transfusion Protocols PDFDocumento5 pagineBlood Transfusion Protocols PDFabhivnairNessuna valutazione finora
- NUR 210 Syllabus and Outline - Summer 2021Documento15 pagineNUR 210 Syllabus and Outline - Summer 2021Penny TratiaNessuna valutazione finora
- Pe103-Course-Guide-And-Module-Sem. 2022-2023Documento55 paginePe103-Course-Guide-And-Module-Sem. 2022-2023Thomas Danjo ManulatNessuna valutazione finora
- IDS - Tuberculosis (Dr. Sy)Documento5 pagineIDS - Tuberculosis (Dr. Sy)Renrenz PayumoNessuna valutazione finora
- 162 319 1 SMDocumento8 pagine162 319 1 SMAsniar RNessuna valutazione finora
- Family Care PlanDocumento3 pagineFamily Care PlanAngie MandeoyaNessuna valutazione finora
- Business Prospect and ProposalDocumento3 pagineBusiness Prospect and ProposalSUBHANKAR GHOSHNessuna valutazione finora
- DR Sandeep Dewan Webinar InvitationDocumento3 pagineDR Sandeep Dewan Webinar InvitationShehbaz ThakurNessuna valutazione finora
- Undangan Seminar Internasional 2021-DikonversiDocumento4 pagineUndangan Seminar Internasional 2021-DikonversiJandi PermadiNessuna valutazione finora
- Bowel Management Following Spinal Cord InjuryDocumento24 pagineBowel Management Following Spinal Cord InjuryBogdan PuscalauNessuna valutazione finora
- Critical Care-Sepsis Case StudyDocumento25 pagineCritical Care-Sepsis Case Studyapi-378305067Nessuna valutazione finora
- What Is Clinical Psychology?: DefinitionsDocumento15 pagineWhat Is Clinical Psychology?: DefinitionsJay Mark CabreraNessuna valutazione finora
- International Profiles of Health Care Systems Dec2020Documento228 pagineInternational Profiles of Health Care Systems Dec2020GODWIN MAYSON LIWANAGNessuna valutazione finora
- Healthcare Fraud in CanadaDocumento28 pagineHealthcare Fraud in CanadaMartin McTaggartNessuna valutazione finora
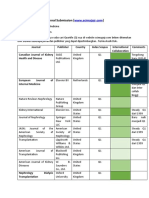
- Journal SubmissionDocumento3 pagineJournal SubmissionMaruhum Bonar MarbunNessuna valutazione finora
- Reading New E2 PDFDocumento50 pagineReading New E2 PDFMary Jis100% (1)
- Athlete's FootDocumento8 pagineAthlete's Footsneh1509Nessuna valutazione finora
- March 2013 Board of Nursing NoticesDocumento528 pagineMarch 2013 Board of Nursing NoticesJames LindonNessuna valutazione finora
- Society of Radiographers - PDFDocumento9 pagineSociety of Radiographers - PDFOsama AhmedNessuna valutazione finora
- Stress Testing of Drug SubstancesDocumento29 pagineStress Testing of Drug SubstancesMr. HIMANSHU PALIWALNessuna valutazione finora
- Inc Tnai IcnDocumento7 pagineInc Tnai IcnDeena MelvinNessuna valutazione finora
- NATIONAL INSURANCE - National Parivar Mediclaim PolicyDocumento31 pagineNATIONAL INSURANCE - National Parivar Mediclaim PolicyStigan IndiaNessuna valutazione finora
- ResumeDocumento1 paginaResumeapi-353709440Nessuna valutazione finora
- Jurnal KesehatanDocumento17 pagineJurnal KesehatanDiani Rista SariNessuna valutazione finora
- Semmelweis University Brochure ENGDocumento5 pagineSemmelweis University Brochure ENGZita Nemet SeresNessuna valutazione finora
- Assesement of KapDocumento50 pagineAssesement of Kapggdawit80% (5)
- Summative Test in Arts & Health 8 (3rd Grading)Documento4 pagineSummative Test in Arts & Health 8 (3rd Grading)MARIA CRISTINA TEMAJONessuna valutazione finora