Potrebbero piacerti anche
- Guillain Barre Syndrome A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandGuillain Barre Syndrome A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Guillain Barre SyndromDocumento10 pagineGuillain Barre SyndromMiirnaawatii YalidaaNessuna valutazione finora
- What Is GuillainDocumento4 pagineWhat Is GuillainHelda SeptivanyNessuna valutazione finora
- Immune System Weakness Paralysis: Guillain-Barré FactsDocumento6 pagineImmune System Weakness Paralysis: Guillain-Barré FactsYuliana MuharramiNessuna valutazione finora
- Aan ?event Print&disorder - Id 935: TreatmentDocumento3 pagineAan ?event Print&disorder - Id 935: TreatmentclaudiaNessuna valutazione finora
- Guillain Barre SyndromeDocumento13 pagineGuillain Barre Syndromenyx minaNessuna valutazione finora
- Guil LianDocumento18 pagineGuil LianPdianghunNessuna valutazione finora
- Guillain-Barre Syndrome (Cont.) : Smaller Medium LargerDocumento4 pagineGuillain-Barre Syndrome (Cont.) : Smaller Medium LargerRully Riyan DikaNessuna valutazione finora
- Guillain-Barré Syndrome: SymptomsDocumento2 pagineGuillain-Barré Syndrome: SymptomsRatu Alipate DaunibauNessuna valutazione finora
- What Is GuillainDocumento1 paginaWhat Is Guillainloveitornot28Nessuna valutazione finora
- Neuromuscular DiseasesDocumento85 pagineNeuromuscular DiseasesAaron James GrayNessuna valutazione finora
- Guillain-Barré Syndrome: Key FactsDocumento4 pagineGuillain-Barré Syndrome: Key FactsrikarikaNessuna valutazione finora
- Guillane Barre SyndromeDocumento8 pagineGuillane Barre SyndromeyasiraNessuna valutazione finora
- Guillain-Barré Syndrome: Dr. Angelo Smith M.D WHPLDocumento30 pagineGuillain-Barré Syndrome: Dr. Angelo Smith M.D WHPLLeshery SemiraNessuna valutazione finora
- Guillain Barre Syndrome: Molebatsi TheletsaneDocumento16 pagineGuillain Barre Syndrome: Molebatsi TheletsaneSri KombongNessuna valutazione finora
- Guillain-Barre Syndrome: Practice EssentialsDocumento18 pagineGuillain-Barre Syndrome: Practice EssentialsAna-Maria DuMiNessuna valutazione finora
- Guillain-Barre Syndrome: Practice EssentialsDocumento16 pagineGuillain-Barre Syndrome: Practice EssentialsUKMBasketNessuna valutazione finora
- Guillain-Barre Syndrome: InfectionsDocumento13 pagineGuillain-Barre Syndrome: InfectionsUzra ShujaatNessuna valutazione finora
- Guillain-Barre Syndrome: CausesDocumento6 pagineGuillain-Barre Syndrome: Causesanindadwianggra_8911Nessuna valutazione finora
- Guillain-Barre Syndrome: PrintDocumento8 pagineGuillain-Barre Syndrome: PrintAlfrien Ivanovich LarchsonNessuna valutazione finora
- Mounika G1Documento8 pagineMounika G1pandem soniyaNessuna valutazione finora
- Research On GuillainDocumento31 pagineResearch On GuillainsohriaameroldimaporoNessuna valutazione finora
- GB SyndromeDocumento17 pagineGB Syndromehajra StudentNessuna valutazione finora
- GB SyndromDocumento5 pagineGB Syndromavinash dhameriyaNessuna valutazione finora
- DivineDocumento3 pagineDivinemilamielNessuna valutazione finora
- Who Guillain Barre SyndromeDocumento3 pagineWho Guillain Barre SyndromeDevaricaNessuna valutazione finora
- Guillain-Barre Syndrome Fact SheetDocumento7 pagineGuillain-Barre Syndrome Fact SheetsohriaameroldimaporoNessuna valutazione finora
- Guillian Baare Syndrome: Mr. Jeo Thomas 1 M.SC Nursing SconDocumento38 pagineGuillian Baare Syndrome: Mr. Jeo Thomas 1 M.SC Nursing SconJeo Thomas100% (1)
- Myotonic Dystrophy Is A Long Term Genetic Disorder That Affects Muscle FunctionDocumento3 pagineMyotonic Dystrophy Is A Long Term Genetic Disorder That Affects Muscle FunctionJared Tristan LewisNessuna valutazione finora
- Guillain-Barre Syndrome: Presented by DR - Ruma Dey Dept. of KayachikitsaDocumento33 pagineGuillain-Barre Syndrome: Presented by DR - Ruma Dey Dept. of KayachikitsaSushanta DasNessuna valutazione finora
- What Is Guillain-Barré Syndrome?Documento6 pagineWhat Is Guillain-Barré Syndrome?bella dwiNessuna valutazione finora
- Guillain-Barré Syndrome - WikipediaDocumento18 pagineGuillain-Barré Syndrome - WikipediaMuthu KumarNessuna valutazione finora
- Guillain-Barré Syndrome (GBS) : Prepared by Dr. Madiha Anees PT Asst. Prof/VP RCRS MS-PT, BS-PTDocumento26 pagineGuillain-Barré Syndrome (GBS) : Prepared by Dr. Madiha Anees PT Asst. Prof/VP RCRS MS-PT, BS-PTaneelala kanwal kanwalNessuna valutazione finora
- Guiilan Barre SyndromeDocumento19 pagineGuiilan Barre SyndromeDhayaneeDruAinsleyIINessuna valutazione finora
- Guillain-Barré Syndrome: Andrie Gunawan, MDDocumento17 pagineGuillain-Barré Syndrome: Andrie Gunawan, MDAgung TpNessuna valutazione finora
- What Is Guillain-Barré Syndrome?Documento6 pagineWhat Is Guillain-Barré Syndrome?Judy Ramos De GuzmanNessuna valutazione finora
- Guillain-Barre Syndrome Fact SheetDocumento8 pagineGuillain-Barre Syndrome Fact SheetJannah Marie A. DimaporoNessuna valutazione finora
- Chapter 607 - Guillain-Barré Syndrome: Clinical ManifestationsDocumento3 pagineChapter 607 - Guillain-Barré Syndrome: Clinical ManifestationsclaudiaNessuna valutazione finora
- Guillane - Barre SyndromeDocumento16 pagineGuillane - Barre SyndromeMarivic DianoNessuna valutazione finora
- Guillain Barre SyndromeDocumento38 pagineGuillain Barre SyndromePeterson Wachira HscNessuna valutazione finora
- Askep Pasien Yang Mengalami Guillain-Barré Syndrome: Maridi M. DirdjoDocumento14 pagineAskep Pasien Yang Mengalami Guillain-Barré Syndrome: Maridi M. DirdjoPalupi Setyo HapsariNessuna valutazione finora
- Koni GBSDocumento7 pagineKoni GBSWinda Lestari RajagukgukNessuna valutazione finora
- Symptoms: Products & ServicesDocumento5 pagineSymptoms: Products & ServicesVierynaNessuna valutazione finora
- Guillain-Barré Syndrome (GBS)Documento17 pagineGuillain-Barré Syndrome (GBS)Desima Tamara sinuratNessuna valutazione finora
- Guillain Barre SyndromeDocumento26 pagineGuillain Barre Syndromealma baterinaNessuna valutazione finora
- GBS Source 1Documento4 pagineGBS Source 1PJHG50% (2)
- Guillain-Barre Syndrome (GBS)Documento34 pagineGuillain-Barre Syndrome (GBS)api-19916399Nessuna valutazione finora
- Guillain Barre SyndromeDocumento20 pagineGuillain Barre SyndromeRamalakshmi LakshmiNessuna valutazione finora
- Guillan Barre Syndrome FinalDocumento16 pagineGuillan Barre Syndrome FinalAswathy RCNessuna valutazione finora
- Guillain Barre SyndromeDocumento16 pagineGuillain Barre SyndromeAgnes NesiaNessuna valutazione finora
- Gullian Barry SyndromeDocumento19 pagineGullian Barry SyndromeSayeeda AreebaNessuna valutazione finora
- Guillain-Barré SyndromeDocumento21 pagineGuillain-Barré SyndromeZulkarnainBustamamNessuna valutazione finora
- Presentation On Guillain Barre Syndrome: Submitted To: Submitted byDocumento12 paginePresentation On Guillain Barre Syndrome: Submitted To: Submitted bypandem soniyaNessuna valutazione finora
- Guillain Barre SyndromeDocumento23 pagineGuillain Barre Syndromeleenie_goni100% (1)
- Script For PresentDocumento3 pagineScript For PresentTanya HoNessuna valutazione finora
- GBS FaqsDocumento2 pagineGBS Faqssurender_singh_43Nessuna valutazione finora
- Guillain Barre SyndromeDocumento16 pagineGuillain Barre SyndromeHira JabeenNessuna valutazione finora
- Guillain - Barre - SyndromeDocumento18 pagineGuillain - Barre - SyndromeRAMNessuna valutazione finora
- Pneumoniae), Vaccines (E.g., Rabies, Tetanus, and Influenza), Lymphoma, Surgery, and TraumaDocumento7 paginePneumoniae), Vaccines (E.g., Rabies, Tetanus, and Influenza), Lymphoma, Surgery, and TraumaKenn yahweexNessuna valutazione finora
- What Is Guillain-Barré Syndrome (GBS) ?: Navalta, John Paul V BSN 3-ADocumento4 pagineWhat Is Guillain-Barré Syndrome (GBS) ?: Navalta, John Paul V BSN 3-AJohn Paul NavaltaNessuna valutazione finora
- Physical Assessment: Bayogo, Mari Mel L. Bsn-3A Group 1Documento10 paginePhysical Assessment: Bayogo, Mari Mel L. Bsn-3A Group 1John Paul NavaltaNessuna valutazione finora
- Cholera: Vibrio Cholera/ Vibrio ComaDocumento5 pagineCholera: Vibrio Cholera/ Vibrio ComaJohn Paul NavaltaNessuna valutazione finora
- Harrington Rod Lugue Rod Bipolar Hip ProsthesisDocumento3 pagineHarrington Rod Lugue Rod Bipolar Hip ProsthesisJohn Paul NavaltaNessuna valutazione finora
- PoliomyelitisDocumento4 paginePoliomyelitisJohn Paul NavaltaNessuna valutazione finora
- Acinetobacter Baumannii Infections UpdateDocumento68 pagineAcinetobacter Baumannii Infections Updatetummalapalli venkateswara rao100% (2)
- WWW Namrata CoDocumento55 pagineWWW Namrata CoMunesh SherawatNessuna valutazione finora
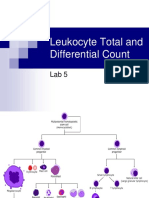
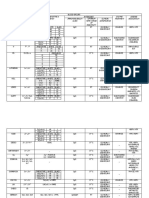
- Leukocyte Total and Differential CountDocumento37 pagineLeukocyte Total and Differential CountHend HamedNessuna valutazione finora
- Universal Tutorials - X CBSE: Mock Test E03: English: Term IIDocumento4 pagineUniversal Tutorials - X CBSE: Mock Test E03: English: Term IIJohn DoeNessuna valutazione finora
- UC Davis Koret Shelter Medicine Program - Feline Immunodeficiency (FIV) - 2013-04-11Documento3 pagineUC Davis Koret Shelter Medicine Program - Feline Immunodeficiency (FIV) - 2013-04-11Kitt KaosNessuna valutazione finora
- Doh ProgramsDocumento45 pagineDoh ProgramsVon Andre AposagaNessuna valutazione finora
- Dermatosis ErythrosquamousDocumento16 pagineDermatosis ErythrosquamousVicky Ilda ViantiniNessuna valutazione finora
- Child With Non Blanching RashDocumento6 pagineChild With Non Blanching Rashtanya mathewNessuna valutazione finora
- Polio DR Suzanne Humphries Clear SlidesDocumento57 paginePolio DR Suzanne Humphries Clear Slidesvaccinationcouncil100% (21)
- Blood Groups Assignment AaaDocumento3 pagineBlood Groups Assignment AaaLoro JDNessuna valutazione finora
- Immunology-Lab-Worksheet-Student 3-6Documento4 pagineImmunology-Lab-Worksheet-Student 3-6api-290100812Nessuna valutazione finora
- 2 Radss Easy Manual PDFDocumento7 pagine2 Radss Easy Manual PDFKarl Robert AdorNessuna valutazione finora
- AbscessDocumento4 pagineAbscessShivBalakChauhanNessuna valutazione finora
- DHIS PHC Facility Monthly Report FormDocumento4 pagineDHIS PHC Facility Monthly Report FormUmair SaleemNessuna valutazione finora
- Fine-Needle Aspiration Cytology in The Diagnosis of Tuberculous LesionsDocumento9 pagineFine-Needle Aspiration Cytology in The Diagnosis of Tuberculous Lesionsmohamaed abbasNessuna valutazione finora
- Lectura IIDocumento5 pagineLectura IIMendoza GeralNessuna valutazione finora
- School Based Immunization Form Grade 1Documento1 paginaSchool Based Immunization Form Grade 1maristellaNessuna valutazione finora
- Pathology SGD 4: Diseases-Of-The-Immune-System: Group-4Documento23 paginePathology SGD 4: Diseases-Of-The-Immune-System: Group-4Kalpana JenaNessuna valutazione finora
- Nursing Care Plan of The NewbornDocumento4 pagineNursing Care Plan of The Newbornbowki namoNessuna valutazione finora
- Intro 7Documento2 pagineIntro 7QUIZANA, Ceazairenee P.Nessuna valutazione finora
- Immunohema & Transfusion MedDocumento62 pagineImmunohema & Transfusion MedMark Joseph Felicitas CuntapayNessuna valutazione finora
- Parasitology Guide QuestionDocumento2 pagineParasitology Guide QuestionRoll BiNessuna valutazione finora
- Nursing Care PlanDocumento17 pagineNursing Care Planjohnlyn bongotNessuna valutazione finora
- S35 - Anil Kumar Pandey (J.K. Pathology) Near V Mart, Gandhi Ground, BADAUN243601 9058494498 / 8755328670Documento6 pagineS35 - Anil Kumar Pandey (J.K. Pathology) Near V Mart, Gandhi Ground, BADAUN243601 9058494498 / 8755328670Satyabhan SinghNessuna valutazione finora
- Blood Transfusion Policy 6.3Documento90 pagineBlood Transfusion Policy 6.3raNessuna valutazione finora
- Vet Diagnostix Products ListDocumento4 pagineVet Diagnostix Products ListrcllanoscNessuna valutazione finora
- Nobel Prize Laurates in Immunology Presentation List FINALDocumento3 pagineNobel Prize Laurates in Immunology Presentation List FINALzeyneptoros13Nessuna valutazione finora
- Inflammation and HealingDocumento30 pagineInflammation and HealingKoustubh JoshiNessuna valutazione finora
- Malaria 1Documento24 pagineMalaria 1Jamuna PatelNessuna valutazione finora
- Vector Borne Diseases: Presentator: Atikah Najla RodhiahDocumento15 pagineVector Borne Diseases: Presentator: Atikah Najla RodhiahTengku Mossadeq Al QornyNessuna valutazione finora