Potrebbero piacerti anche
- Southampton Music in The City 2014Documento1 paginaSouthampton Music in The City 2014Southern Daily EchoNessuna valutazione finora
- Winchester Hat Fair 2014 ProgrammeDocumento1 paginaWinchester Hat Fair 2014 ProgrammeSouthern Daily EchoNessuna valutazione finora
- South Coast Business Awards 2014 Ticket Booking FormDocumento1 paginaSouth Coast Business Awards 2014 Ticket Booking FormSouthern Daily EchoNessuna valutazione finora
- Winchester Hat Fair 2014 ProgrammeDocumento1 paginaWinchester Hat Fair 2014 ProgrammeSouthern Daily EchoNessuna valutazione finora
- Southampton Half MarathonDocumento1 paginaSouthampton Half MarathonSouthern Daily EchoNessuna valutazione finora
- Winchester Hat Fair 2014 ProgrammeDocumento1 paginaWinchester Hat Fair 2014 ProgrammeSouthern Daily EchoNessuna valutazione finora
- Open Letter From Southampton Connect Re Channel 4 Filming in Derby Road,...Documento3 pagineOpen Letter From Southampton Connect Re Channel 4 Filming in Derby Road,...Southern Daily EchoNessuna valutazione finora
- Scba 2014Documento1 paginaScba 2014Southern Daily EchoNessuna valutazione finora
- Flooding Advice For The PublicDocumento8 pagineFlooding Advice For The PublicRayDuffNessuna valutazione finora
- Southampton Film Festival Guide 2013Documento13 pagineSouthampton Film Festival Guide 2013Southern Daily EchoNessuna valutazione finora
- Scba 2014Documento1 paginaScba 2014Southern Daily EchoNessuna valutazione finora
- School League Tables 2013Documento6 pagineSchool League Tables 2013Southern Daily EchoNessuna valutazione finora
- CantellOfsted Report 2013Documento9 pagineCantellOfsted Report 2013Southern Daily EchoNessuna valutazione finora
- New Forest Half Marathon 2013 ResultsDocumento16 pagineNew Forest Half Marathon 2013 ResultsSouthern Daily EchoNessuna valutazione finora
- Winchester Hat Fair 2013Documento12 pagineWinchester Hat Fair 2013Southern Daily EchoNessuna valutazione finora
- Go! Rhino Photograph Competition PDFDocumento12 pagineGo! Rhino Photograph Competition PDFSouthern Daily EchoNessuna valutazione finora
- Go! Rhinos SouthamptonDocumento1 paginaGo! Rhinos SouthamptonSouthern Daily EchoNessuna valutazione finora
- Gannett Application FormDocumento7 pagineGannett Application FormSouthern Daily EchoNessuna valutazione finora
- Shirley Towers Firefigher Deaths ReportDocumento184 pagineShirley Towers Firefigher Deaths ReportSouthern Daily Echo100% (1)
- PSP Southampton Boat Show Magazine 2013 PDFDocumento80 paginePSP Southampton Boat Show Magazine 2013 PDFSouthern Daily EchoNessuna valutazione finora
- Bestival Map 2013Documento1 paginaBestival Map 2013Southern Daily EchoNessuna valutazione finora
- PC2752 Royal Princess Local Map HIRESDocumento1 paginaPC2752 Royal Princess Local Map HIRESSouthern Daily EchoNessuna valutazione finora
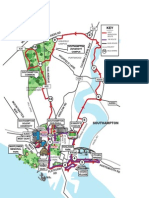
- Go! Rhinos Southampton MapDocumento1 paginaGo! Rhinos Southampton MapSouthern Daily EchoNessuna valutazione finora
- Report: Police Custody Suites in HampshireDocumento52 pagineReport: Police Custody Suites in HampshireIWCPOnlineNessuna valutazione finora
- LCATC Group Budget Amendment Final 110213Documento25 pagineLCATC Group Budget Amendment Final 110213Southern Daily EchoNessuna valutazione finora
- Tesco Retail Critique Test Valley Borough Council 15 January 2013 10994/04Documento36 pagineTesco Retail Critique Test Valley Borough Council 15 January 2013 10994/04Southern Daily EchoNessuna valutazione finora
- SC012020 3 PDFDocumento7 pagineSC012020 3 PDFSouthern Daily EchoNessuna valutazione finora
- Winchester Prison ReportDocumento145 pagineWinchester Prison ReportSouthern Daily EchoNessuna valutazione finora
- Lib Dem Group Budget Proposals 13th-Feb-2013 14.00 CouncilDocumento28 pagineLib Dem Group Budget Proposals 13th-Feb-2013 14.00 CouncilSouthern Daily EchoNessuna valutazione finora
- Coroner's Recommendations After Firefighter DeathsDocumento4 pagineCoroner's Recommendations After Firefighter DeathsSouthern Daily EchoNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Complex Regional Pain Syndrome Concise Guidance 1Documento6 pagineComplex Regional Pain Syndrome Concise Guidance 1roooNessuna valutazione finora
- 473 eDocumento9 pagine473 eAzmi FarhadiNessuna valutazione finora
- 08 - Geriatric Dentistry A ReviewDocumento4 pagine08 - Geriatric Dentistry A ReviewbkprosthoNessuna valutazione finora
- Executive SummaryPOWER PIONTDocumento12 pagineExecutive SummaryPOWER PIONTXha LomerioNessuna valutazione finora
- Lupus NephritisDocumento15 pagineLupus NephritisVilza maharaniNessuna valutazione finora
- Nurs FPX 4050 Assessment 4 Final Care Coordination PlanDocumento6 pagineNurs FPX 4050 Assessment 4 Final Care Coordination Planfarwaamjad771Nessuna valutazione finora
- DSM 5 Autism Spectrum Disorder Fact SheetDocumento2 pagineDSM 5 Autism Spectrum Disorder Fact SheetMario MendozaNessuna valutazione finora
- Counselling-GATHER ApproachDocumento23 pagineCounselling-GATHER ApproachAnilkumar JaraliNessuna valutazione finora
- 2014 Burn Patient Management - Clinical Practice GuidelinesDocumento70 pagine2014 Burn Patient Management - Clinical Practice Guidelinesd dNessuna valutazione finora
- Felix Guattari - Molecular Revolution - Psychiatry and PoliticsDocumento156 pagineFelix Guattari - Molecular Revolution - Psychiatry and PoliticsPatrick StaryNessuna valutazione finora
- Bomba MedtronicDocumento40 pagineBomba MedtronicrafaelplNessuna valutazione finora
- The Psychological AspectsDocumento7 pagineThe Psychological AspectsInvisible_TouchNessuna valutazione finora
- AFCC Powerpoint 2017 Pruter Powerpoint CC DR ChildressDocumento8 pagineAFCC Powerpoint 2017 Pruter Powerpoint CC DR Childressa.petersritNessuna valutazione finora
- Materi Sjs LoratadineDocumento8 pagineMateri Sjs LoratadineLala Rahma Qodriyan SofiakmiNessuna valutazione finora
- Pyelonephritis 1 Running Head: PYELONEPHRITISDocumento4 paginePyelonephritis 1 Running Head: PYELONEPHRITISENessuna valutazione finora
- Pysche OSCE - EPSE ExaminationDocumento1 paginaPysche OSCE - EPSE ExaminationAmber WangNessuna valutazione finora
- Adam B. Galla: Independent Consultant (July 2016) ManniondanielsDocumento4 pagineAdam B. Galla: Independent Consultant (July 2016) ManniondanielsAnonymous G4aIQ7aHNessuna valutazione finora
- Open Reduction and Internal Fixation of The.17Documento2 pagineOpen Reduction and Internal Fixation of The.17Rakesh KumarNessuna valutazione finora
- Medi 95 E2881Documento5 pagineMedi 95 E2881Betari YoscarNessuna valutazione finora
- Confidentiality - A Case ScenarioDocumento4 pagineConfidentiality - A Case ScenarioimmaNessuna valutazione finora
- Black Book CalgaryDocumento386 pagineBlack Book CalgaryJackNessuna valutazione finora
- Bourdin, D. (2003) - La Pensée Clinique Clinical Thinking André GreenDocumento4 pagineBourdin, D. (2003) - La Pensée Clinique Clinical Thinking André GreenofanimenochNessuna valutazione finora
- Eng PDFDocumento220 pagineEng PDFyunNessuna valutazione finora
- R115Patients PDFDocumento14 pagineR115Patients PDFcarneoliaNessuna valutazione finora
- Guidelines For The Establishment of Appropriate Beyond Use Dating of Sterile Compounded AdmixturesDocumento50 pagineGuidelines For The Establishment of Appropriate Beyond Use Dating of Sterile Compounded AdmixturesDea NandaNessuna valutazione finora
- Training Our Minds in CFT - 1Documento5 pagineTraining Our Minds in CFT - 1Anita CassNessuna valutazione finora
- Outcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)Documento7 pagineOutcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)William ChandlerNessuna valutazione finora
- Paternal Postnatal Psychiatric - IllnessesDocumento202 paginePaternal Postnatal Psychiatric - IllnessesBalasubrahmanya K. R.Nessuna valutazione finora
- Nutrient BasicsDocumento33 pagineNutrient Basicsapi-344976556Nessuna valutazione finora
- Documentation Assignments: Mental Health Case: George PaloDocumento3 pagineDocumentation Assignments: Mental Health Case: George PaloPattie100% (1)