Potrebbero piacerti anche
- A Comparative Study of Text Comprehension in IELTS Reading Exam Using GPT-3Documento8 pagineA Comparative Study of Text Comprehension in IELTS Reading Exam Using GPT-3Anonymous Gl4IRRjzNNessuna valutazione finora
- From Clicks To Security: Investigating Continuous Authentication Via Mouse DynamicsDocumento16 pagineFrom Clicks To Security: Investigating Continuous Authentication Via Mouse DynamicsAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Papers - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Papers - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Papers - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Papers - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- IoT Security: Penetration Testing of White-Label Cloud-Based IoT Camera Compromising Personal Data PrivacyDocumento12 pagineIoT Security: Penetration Testing of White-Label Cloud-Based IoT Camera Compromising Personal Data PrivacyAnonymous Gl4IRRjzNNessuna valutazione finora
- Variations in Outcome For The Same Map Reduce Transitive Closure Algorithm Implemented On Different Hadoop PlatformsDocumento8 pagineVariations in Outcome For The Same Map Reduce Transitive Closure Algorithm Implemented On Different Hadoop PlatformsAnonymous Gl4IRRjzNNessuna valutazione finora
- Comparison of Rendering Processes On 3D ModelDocumento10 pagineComparison of Rendering Processes On 3D ModelAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- XML Encryption and Signature For Securing Web ServicesDocumento14 pagineXML Encryption and Signature For Securing Web ServicesAnonymous Gl4IRRjzNNessuna valutazione finora
- Determining Business Intelligence Usage SuccessDocumento23 pagineDetermining Business Intelligence Usage SuccessAnonymous Gl4IRRjzNNessuna valutazione finora
- Machine Learning in Early Genetic Detection of Multiple Sclerosis Disease: A SurveyDocumento18 pagineMachine Learning in Early Genetic Detection of Multiple Sclerosis Disease: A SurveyAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Wi-Fi Data Analysis Based On Machine LearningDocumento9 pagineWi-Fi Data Analysis Based On Machine LearningAnonymous Gl4IRRjzNNessuna valutazione finora
- A New Approach For Ranking Shadowed Fuzzy Numbers and Its ApplicationDocumento16 pagineA New Approach For Ranking Shadowed Fuzzy Numbers and Its ApplicationAnonymous Gl4IRRjzNNessuna valutazione finora
- Secure Arcade: A Gamified Defense Against Cyber AttacksDocumento17 pagineSecure Arcade: A Gamified Defense Against Cyber AttacksAnonymous Gl4IRRjzNNessuna valutazione finora
- Analysing Chatgpt's Potential Through The Lens of Creating Research PapersDocumento17 pagineAnalysing Chatgpt's Potential Through The Lens of Creating Research PapersAnonymous Gl4IRRjzNNessuna valutazione finora
- Detection of Structured Query Language Injection Attacks Using Machine Learning TechniquesDocumento14 pagineDetection of Structured Query Language Injection Attacks Using Machine Learning TechniquesAnonymous Gl4IRRjzNNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 4 Managerial EconomicsDocumento8 pagine4 Managerial EconomicsBoSs GamingNessuna valutazione finora
- Supplement 1 - Interim View of An Interpreter's Guide For eTOM and ITIL Practitioners PDFDocumento54 pagineSupplement 1 - Interim View of An Interpreter's Guide For eTOM and ITIL Practitioners PDFShantamNessuna valutazione finora
- Tutorial 3 - SolutionsDocumento11 pagineTutorial 3 - SolutionsLijing CheNessuna valutazione finora
- Resume - Sanchit GoyalDocumento1 paginaResume - Sanchit GoyaltompaulmarottickalNessuna valutazione finora
- Rps Digital MarketingDocumento7 pagineRps Digital Marketingsetiawanputraharianto99Nessuna valutazione finora
- Kanenus College: PART I: - Write True If The Statement Is Correct Unless Write FalseDocumento2 pagineKanenus College: PART I: - Write True If The Statement Is Correct Unless Write Falseteferi GetachewNessuna valutazione finora
- Dmgt206 Production and Operations ManagementDocumento302 pagineDmgt206 Production and Operations ManagementFerisal Firmansyah100% (1)
- Hardox400 PDFDocumento2 pagineHardox400 PDFZairullah El-AzharNessuna valutazione finora
- Gillette - SWOT AnalysisDocumento7 pagineGillette - SWOT AnalysisM HarikrishnanNessuna valutazione finora
- ASsignemts SCIDocumento25 pagineASsignemts SCIPedro PelaezNessuna valutazione finora
- The Production CycleDocumento2 pagineThe Production CycleAmara PrabasariNessuna valutazione finora
- Amazon Fulfillment ProcessDocumento1 paginaAmazon Fulfillment ProcessRAHUL RNAIRNessuna valutazione finora
- Unit 2 - Classification of Production SystemDocumento20 pagineUnit 2 - Classification of Production SystemUrwashiNessuna valutazione finora
- GomoryDocumento40 pagineGomoryguidelliNessuna valutazione finora
- Business Process OutsourcingDocumento74 pagineBusiness Process OutsourcingmajhiajitNessuna valutazione finora
- Ch183 Process Cost Systemsdocx PDF FreeDocumento52 pagineCh183 Process Cost Systemsdocx PDF FreeROLANDO II EVANGELISTANessuna valutazione finora
- Report On Surf ExcelDocumento26 pagineReport On Surf ExcelSaad NazeerNessuna valutazione finora
- Warehouse Management System: Complex Processes - Easily OperatedDocumento12 pagineWarehouse Management System: Complex Processes - Easily OperatedAdib FauzanNessuna valutazione finora
- Research For Mater Bussiness AdmnistrationDocumento57 pagineResearch For Mater Bussiness AdmnistrationTadesse KetemaNessuna valutazione finora
- MSP ProceduresDocumento18 pagineMSP ProcedurestarunNessuna valutazione finora
- Administering Planning ModulesDocumento197 pagineAdministering Planning ModulesRasel moreNessuna valutazione finora
- Module 5 Introduction To Display AdvertisingDocumento41 pagineModule 5 Introduction To Display AdvertisingVMPNessuna valutazione finora
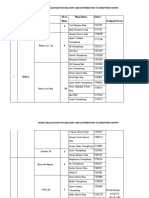
- SL No Super - Zone Zone No of Shops Shops Names Contact Designated Focals 2Documento15 pagineSL No Super - Zone Zone No of Shops Shops Names Contact Designated Focals 2r.dorji237Nessuna valutazione finora
- Ooad Unit 5Documento50 pagineOoad Unit 5Charveer “CHARVEERTV” tvNessuna valutazione finora
- Fit-Gap Analysis - OverviewDocumento8 pagineFit-Gap Analysis - Overviewsoorya6969Nessuna valutazione finora
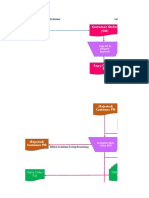
- Flow Chart Revenue CycleDocumento24 pagineFlow Chart Revenue Cycleimari PPM100% (1)
- Mughal SteelDocumento73 pagineMughal Steelوقاص بھٹیNessuna valutazione finora
- SWOT Analysis of Ferns N Petals: StrengthsDocumento4 pagineSWOT Analysis of Ferns N Petals: StrengthsNitesh KumarNessuna valutazione finora
- Reflection Paper FinalDocumento6 pagineReflection Paper FinalTrisha ZarenoNessuna valutazione finora