Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- _AmVetPub_August2016Documento20 pagine_AmVetPub_August2016NoSpamNessuna valutazione finora
- Impaired Gas Exchange PneumoniaDocumento2 pagineImpaired Gas Exchange PneumoniaShanice BedecirNessuna valutazione finora
- Cohort Study Hansana PDFDocumento28 pagineCohort Study Hansana PDFTukai KulkarniNessuna valutazione finora
- ParQ Plus Jan 2023Documento6 pagineParQ Plus Jan 2023troy montarilNessuna valutazione finora
- Coronavirus (COVID-19) Testing - Statistics and Research - Our World in DataDocumento89 pagineCoronavirus (COVID-19) Testing - Statistics and Research - Our World in Datahah266611Nessuna valutazione finora
- Hltinf001 Student Workbook (Word) (c3) .v1.1Documento61 pagineHltinf001 Student Workbook (Word) (c3) .v1.1Saima Rashid67% (6)
- Malignant Struma OvariiDocumento4 pagineMalignant Struma Ovariixwahyu 108Nessuna valutazione finora
- Bicol University College of Nursing Protozoans ComparisonDocumento3 pagineBicol University College of Nursing Protozoans ComparisonAbegail ListancoNessuna valutazione finora
- Material, Vincent M. (MDRTB Case Presentation)Documento39 pagineMaterial, Vincent M. (MDRTB Case Presentation)vincent materialNessuna valutazione finora
- 0 Stroke Rehabilitation by Richard Wilson and Preeti Raghavan 2019 PDFDocumento295 pagine0 Stroke Rehabilitation by Richard Wilson and Preeti Raghavan 2019 PDFDiana MesquitaNessuna valutazione finora
- Morning Report: November 7, 2019Documento27 pagineMorning Report: November 7, 2019Fadilah Amalia HusnaNessuna valutazione finora
- Uzma Khan - Jlu05907 (IA-1)Documento5 pagineUzma Khan - Jlu05907 (IA-1)Uzma KhanNessuna valutazione finora
- Types of Seizures: LIBAO, Kevin L. BSN-2HDocumento3 pagineTypes of Seizures: LIBAO, Kevin L. BSN-2HKevin100% (1)
- Common Beliefs About The Causes of DiseasesDocumento7 pagineCommon Beliefs About The Causes of DiseasesSarah Jane GresoNessuna valutazione finora
- Polymyalgia Rheumatic Symptoms Diagnosis and TreatmentDocumento2 paginePolymyalgia Rheumatic Symptoms Diagnosis and TreatmentHas SimNessuna valutazione finora
- COPD Exacerbation Management Primary CareDocumento1 paginaCOPD Exacerbation Management Primary Caremufidah mawaddahNessuna valutazione finora
- Jurnal Triangle SpiderDocumento17 pagineJurnal Triangle SpiderZuhdi Mahendra KotoNessuna valutazione finora
- Diprogenta Cream/Ointment for Inflammatory DermatosesDocumento2 pagineDiprogenta Cream/Ointment for Inflammatory DermatosesWalter Macasiano GravadorNessuna valutazione finora
- JaundiceDocumento36 pagineJaundiceNasser SalahNessuna valutazione finora
- Viral and Bacterial Infections of The SkinDocumento200 pagineViral and Bacterial Infections of The SkinKarla Jane100% (1)
- Vascular DementiaDocumento7 pagineVascular DementiaAAshish singh BhadoriyaNessuna valutazione finora
- Clinical Aspects of PneumothoraxDocumento3 pagineClinical Aspects of PneumothoraxelisabethNessuna valutazione finora
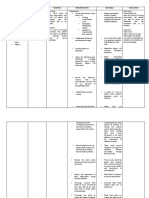
- Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetDocumento3 pagineAssessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Short Term: Independent: Short Term: Goal Partially MetPrincess Mildred AbdonNessuna valutazione finora
- Chinese-Medical Terminology 13021Documento5 pagineChinese-Medical Terminology 13021YS NateNessuna valutazione finora
- Framework For A Safe, Efficient, and Equitable Return To SchoolDocumento33 pagineFramework For A Safe, Efficient, and Equitable Return To Schoolapi-380810458Nessuna valutazione finora
- Antibiotic Guidelines For Adults 2018 PDFDocumento58 pagineAntibiotic Guidelines For Adults 2018 PDFAhmad RizqiNessuna valutazione finora
- Dr. Rinrin Maharani's Curriculum Vitae and Initial Management for Acute StrokeDocumento16 pagineDr. Rinrin Maharani's Curriculum Vitae and Initial Management for Acute StrokeAyu WahyuniNessuna valutazione finora
- Initial Patient Assessment in OpdDocumento4 pagineInitial Patient Assessment in OpdLokender Goyal100% (1)
- Snake Bite First AidDocumento6 pagineSnake Bite First Aidmelchor bangaoilNessuna valutazione finora
- Acute Pharyngitis: EpidemiologyDocumento21 pagineAcute Pharyngitis: EpidemiologyNadia Puspita OktavianiNessuna valutazione finora