Potrebbero piacerti anche
- Jurnal RespirologiDocumento8 pagineJurnal RespirologiMaya SafaatNessuna valutazione finora
- Jurnal GiziDocumento11 pagineJurnal GiziMaya SafaatNessuna valutazione finora
- Jurnal NeurologiDocumento10 pagineJurnal NeurologiMaya SafaatNessuna valutazione finora
- Cystic HygromaDocumento2 pagineCystic HygromaMaya SafaatNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Pediatric TopicsDocumento1 paginaPediatric Topicsabod aloneziNessuna valutazione finora
- 3 - High Energy Formulas For Faltering GrowthDocumento1 pagina3 - High Energy Formulas For Faltering GrowthHarleyMaggyNessuna valutazione finora
- Preschool Health Assessment FormDocumento2 paginePreschool Health Assessment FormSammi GuptaNessuna valutazione finora
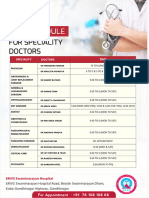
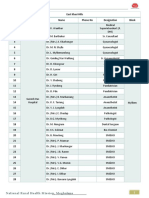
- OPD-Schedule - For SMVS Hospital GandhinagarDocumento2 pagineOPD-Schedule - For SMVS Hospital GandhinagarqoluqaNessuna valutazione finora
- 002 - CPR CommitteeDocumento2 pagine002 - CPR Committeeshehab elsayedNessuna valutazione finora
- It's Time To Reevaluate The Apgar ScoreDocumento2 pagineIt's Time To Reevaluate The Apgar ScoreCandy RevolloNessuna valutazione finora
- Doctors EkhDocumento5 pagineDoctors EkhhippopotamasNessuna valutazione finora
- ROLE of OT in NICUDocumento11 pagineROLE of OT in NICUDeepanshi TyagiNessuna valutazione finora
- High Flow Heated Respiratory Humidifier: HFNC Applicable DepartmentsDocumento2 pagineHigh Flow Heated Respiratory Humidifier: HFNC Applicable DepartmentsAngelina ZhouNessuna valutazione finora
- MedSphere'22 BrochureDocumento17 pagineMedSphere'22 BrochureSuma 123Nessuna valutazione finora
- NURS4060 - AshleyVigne - Assessment 4 - Attempt1Documento7 pagineNURS4060 - AshleyVigne - Assessment 4 - Attempt1ashleyNessuna valutazione finora
- Monarch - Networth - Capital - Initiates - Coverage - On - Rainbow - Children's MedicareDocumento14 pagineMonarch - Networth - Capital - Initiates - Coverage - On - Rainbow - Children's MedicareSriram RanganathanNessuna valutazione finora
- Symphonic 2023Documento6 pagineSymphonic 2023Muthya Aulina FahriyanNessuna valutazione finora
- Full Download Book Breastfeeding A Guide For The Medical Professional PDFDocumento41 pagineFull Download Book Breastfeeding A Guide For The Medical Professional PDFgeorge.pittman905100% (14)
- Lorma Colleges Patient Health History Related Learning ExperienceDocumento2 pagineLorma Colleges Patient Health History Related Learning Experienceivy annNessuna valutazione finora
- Resume Fall 2022 PDFDocumento2 pagineResume Fall 2022 PDFapi-663012445Nessuna valutazione finora
- List of Newly Accredited All Specialties Programs Academic Year: 2020-2021 United StatesDocumento15 pagineList of Newly Accredited All Specialties Programs Academic Year: 2020-2021 United StatesN BNessuna valutazione finora
- List of Equipment and Supplies For Pediatric Units.Documento11 pagineList of Equipment and Supplies For Pediatric Units.vruttika parmar0% (1)
- Telangana Ehs HospitalsDocumento9 pagineTelangana Ehs HospitalsAkbar MohammedNessuna valutazione finora
- KMC For Premature Babies: Esearch RticleDocumento6 pagineKMC For Premature Babies: Esearch RticleSapna thakurNessuna valutazione finora
- List of Nursing BooksDocumento11 pagineList of Nursing BooksChakrapani Chaturvedi100% (1)
- Physicians 07312023Documento1.011 paginePhysicians 07312023Alvin Xtian NucumNessuna valutazione finora
- Task 7,8&9Documento11 pagineTask 7,8&9joyrena ochondraNessuna valutazione finora
- Robotic Assistive Technology Augmenting Dementia Care Technology Design and Preliminary AcceptabilityDocumento5 pagineRobotic Assistive Technology Augmenting Dementia Care Technology Design and Preliminary AcceptabilityHerald Scholarly Open AccessNessuna valutazione finora
- Master Content ListDocumento418 pagineMaster Content ListCristian CalinNessuna valutazione finora
- The Validity of The Pediatric Assessment TriangleDocumento5 pagineThe Validity of The Pediatric Assessment Trianglebaiq putri auliaNessuna valutazione finora
- Haataja 2003Documento1 paginaHaataja 2003Andrea PederziniNessuna valutazione finora
- UNIT I - Modern Concepts & Trends of Child Health CareDocumento19 pagineUNIT I - Modern Concepts & Trends of Child Health CarevigneshNessuna valutazione finora
- Hospital Department and Profesion: Ns. Dwi Nur Rahmantika Puji S M.KepDocumento14 pagineHospital Department and Profesion: Ns. Dwi Nur Rahmantika Puji S M.KepDwi Nur SafitriNessuna valutazione finora
- MCN Skills 2021 Procedure ChecklistDocumento3 pagineMCN Skills 2021 Procedure ChecklistNashebah A. BatuganNessuna valutazione finora