Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
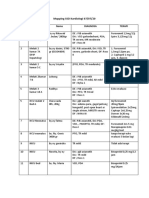
- Mapping SSD Kardiologi 07Documento2 pagineMapping SSD Kardiologi 07Arie FalahNessuna valutazione finora
- Mapping SSD Kardiologi 03Documento2 pagineMapping SSD Kardiologi 03Arie FalahNessuna valutazione finora
- 11659152Documento26 pagine11659152Arie FalahNessuna valutazione finora
- Password 11-11-11Documento1 paginaPassword 11-11-11Arie FalahNessuna valutazione finora
- Book 1Documento3 pagineBook 1Arie FalahNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Notes, MetalsDocumento7 pagineNotes, MetalsindaiNessuna valutazione finora
- Geometry of N-BenzylideneanilineDocumento5 pagineGeometry of N-BenzylideneanilineTheo DianiarikaNessuna valutazione finora
- Celltac MEK 6500Documento3 pagineCelltac MEK 6500RiduanNessuna valutazione finora
- Study of Behavior of Bacterial ConcreteDocumento20 pagineStudy of Behavior of Bacterial ConcreteGodwin KopelliNessuna valutazione finora
- 1 SMDocumento10 pagine1 SMAnindita GaluhNessuna valutazione finora
- Case Study LenovoDocumento10 pagineCase Study LenovoGOHAR GHAFFARNessuna valutazione finora
- Pure Vegeterian: Kousika (CaterersDocumento2 paginePure Vegeterian: Kousika (CaterersShylender NagaNessuna valutazione finora
- Full Carrino Plaza Brochure and Application (General)Documento8 pagineFull Carrino Plaza Brochure and Application (General)tanis581Nessuna valutazione finora
- Medical Nutrition Therapy For DiabetesDocumento27 pagineMedical Nutrition Therapy For Diabetesdr.Uci BaharNessuna valutazione finora
- Cariprazine PDFDocumento162 pagineCariprazine PDFige zaharaNessuna valutazione finora
- Krispy Kreme Doughnut Recipe - Immaculate BitesDocumento2 pagineKrispy Kreme Doughnut Recipe - Immaculate Bitesdaisydrops6Nessuna valutazione finora
- Guimbungan, Core Competency Module 1 - Part 3 PDFDocumento11 pagineGuimbungan, Core Competency Module 1 - Part 3 PDFSharlyne K. GuimbunganNessuna valutazione finora
- NASA ISS Expedition 2 Press KitDocumento27 pagineNASA ISS Expedition 2 Press KitOrion2015Nessuna valutazione finora
- Prepper MealsDocumento22 paginePrepper MealsmeineanmeldungenNessuna valutazione finora
- Qualitative Tests Organic NotesDocumento5 pagineQualitative Tests Organic NotesAdorned. pearlNessuna valutazione finora
- Governance StructureDocumento1 paginaGovernance StructureJoydip MukhopadhyayNessuna valutazione finora
- IS 4049-Part-IDocumento5 pagineIS 4049-Part-ISrinivas KadivetiNessuna valutazione finora
- 2016 Uptown Parksuites D3 PDFDocumento54 pagine2016 Uptown Parksuites D3 PDFArafat Domado100% (1)
- The Aging Brain: Course GuidebookDocumento126 pagineThe Aging Brain: Course GuidebookIsabel Cristina Jaramillo100% (2)
- RIASEC Personality TestDocumento2 pagineRIASEC Personality TestSarah Jane NomoNessuna valutazione finora
- Preservative MaterialsDocumento2 paginePreservative MaterialsmtcengineeringNessuna valutazione finora
- Usp 1078 Good Manufacturing Practices For Bulk Pharmaceutical Excipients PDFDocumento13 pagineUsp 1078 Good Manufacturing Practices For Bulk Pharmaceutical Excipients PDFMayson BaliNessuna valutazione finora
- Natu Es Dsmepa 1ST - 2ND QuarterDocumento38 pagineNatu Es Dsmepa 1ST - 2ND QuarterSenen AtienzaNessuna valutazione finora
- Defects Lamellar TearingDocumento6 pagineDefects Lamellar Tearingguru_terexNessuna valutazione finora
- 1Manuscript-BSN-3y2-1A-CEDILLO-222 11111Documento32 pagine1Manuscript-BSN-3y2-1A-CEDILLO-222 11111SHARMAINE ANNE POLICIOSNessuna valutazione finora
- We Find The Way: Shipping InstructionsDocumento10 pagineWe Find The Way: Shipping InstructionsLuke WangNessuna valutazione finora
- Policy Schedule Personal Accident Insurance Policy: (Plan 5)Documento2 paginePolicy Schedule Personal Accident Insurance Policy: (Plan 5)Rana BiswasNessuna valutazione finora
- The Development of Attachment in Separated and Divorced FamiliesDocumento33 pagineThe Development of Attachment in Separated and Divorced FamiliesInigo BorromeoNessuna valutazione finora
- Janssen Vaccine Phase3 Against Coronavirus (Covid-19)Documento184 pagineJanssen Vaccine Phase3 Against Coronavirus (Covid-19)UzletiszemNessuna valutazione finora