Potrebbero piacerti anche
- Speech Impairment Eligibility FluencyDocumento51 pagineSpeech Impairment Eligibility FluencyRuhiyyih Devy0% (1)
- Classification of Speech Disorders: December 2019Documento21 pagineClassification of Speech Disorders: December 2019Kirti Gunjikar0% (2)
- SLP Student Intake Form Referral Consent Case HistoryDocumento3 pagineSLP Student Intake Form Referral Consent Case Historyapi-617678622Nessuna valutazione finora
- Understanding Childhood Apraxia: Super Duper Handy Handouts!Documento3 pagineUnderstanding Childhood Apraxia: Super Duper Handy Handouts!Staci NeustadtNessuna valutazione finora
- Child's Age Mastered Skills (Most Kids Can Do) Emerging Skills (Half of Kids Can Do) Advanced Skills (A Few Kids Can Do)Documento4 pagineChild's Age Mastered Skills (Most Kids Can Do) Emerging Skills (Half of Kids Can Do) Advanced Skills (A Few Kids Can Do)Bhuvana MudaliarNessuna valutazione finora
- Parents School Therapy Guide PDFDocumento18 pagineParents School Therapy Guide PDFMarta MartNessuna valutazione finora
- Functional Communication AssessmentDocumento1 paginaFunctional Communication AssessmentRoss AdamsNessuna valutazione finora
- Iep TemplateDocumento13 pagineIep Templateapi-301094873100% (1)
- Social DevelopmentDocumento14 pagineSocial DevelopmentSarah AndersonNessuna valutazione finora
- Receptive Expressive ChecklistDocumento2 pagineReceptive Expressive ChecklistMelissa SerranoNessuna valutazione finora
- What Works SLT Interventions For SLCNDocumento170 pagineWhat Works SLT Interventions For SLCNlionella12Nessuna valutazione finora
- Topic 3: Strategies For Supporting Children Language DevelopementDocumento18 pagineTopic 3: Strategies For Supporting Children Language DevelopementFAHMIEY BIN ABDULLAH (KB)Nessuna valutazione finora
- Functional Goals: See It in Action: ShariaDocumento19 pagineFunctional Goals: See It in Action: Shariameet76Nessuna valutazione finora
- Speech Therapy For Language-Based Learning DisabilitiesDocumento2 pagineSpeech Therapy For Language-Based Learning DisabilitiesBrainNessuna valutazione finora
- Strategies For Speech & Language DisordersDocumento55 pagineStrategies For Speech & Language DisordersStacey Ann Forbes100% (3)
- 8 Parent Tips For ArticulationDocumento8 pagine8 Parent Tips For Articulationapi-506001037100% (1)
- Witwer ST Developmental MilestonesDocumento2 pagineWitwer ST Developmental MilestonesErsya Muslih100% (1)
- Early Language Development: Learning ObjectivesDocumento17 pagineEarly Language Development: Learning Objectivesapi-311077175Nessuna valutazione finora
- Toddler Speech Therapy TipsDocumento1 paginaToddler Speech Therapy TipsElena LOgoNessuna valutazione finora
- Comprehensive Language DevelopmentDocumento6 pagineComprehensive Language Developmentpaola mae100% (2)
- Learning Disabilities: by Priya Mary Paulose 1 Year M.SC NursingDocumento51 pagineLearning Disabilities: by Priya Mary Paulose 1 Year M.SC NursingPriya Mary PauloseNessuna valutazione finora
- Increasing Speech SouIncreasing Speech Sound Production of Children With Autisnd Production of Children With AutismDocumento34 pagineIncreasing Speech SouIncreasing Speech Sound Production of Children With Autisnd Production of Children With AutismPrapanit PntNessuna valutazione finora
- Physical Development 0-3 Years:: 3-6 MonthsDocumento13 paginePhysical Development 0-3 Years:: 3-6 MonthsAnonymous l0VyrOPNessuna valutazione finora
- Apraxia Kids Fast FactsDocumento4 pagineApraxia Kids Fast FactsTamiris AlvesNessuna valutazione finora
- Supporting Students with Communication Disorders. A Collaborative Approach: A Resource for Speech-Language Pathologists, Parents and EducatorsDa EverandSupporting Students with Communication Disorders. A Collaborative Approach: A Resource for Speech-Language Pathologists, Parents and EducatorsNessuna valutazione finora
- 132 Sensory Diet 090212Documento2 pagine132 Sensory Diet 090212Sally Vesper100% (1)
- Play Assessment With ScoringDocumento9 paginePlay Assessment With ScoringVijayNessuna valutazione finora
- Where To Begin and Where To GoDocumento25 pagineWhere To Begin and Where To GoLaurine Manana100% (1)
- Speech and Language Developmental ChecklistDocumento5 pagineSpeech and Language Developmental ChecklistBild Andhra PradeshNessuna valutazione finora
- NLA Scoring GuideDocumento5 pagineNLA Scoring GuideMaRiaNessuna valutazione finora
- Fact Sheet Childhood Apraxia of SpeechDocumento2 pagineFact Sheet Childhood Apraxia of SpeechAndini KartikasariNessuna valutazione finora
- Reading Books & Watching TV Playing & Drawing Bathing: How Can You Get Involved? How To Get Them InvolvedDocumento1 paginaReading Books & Watching TV Playing & Drawing Bathing: How Can You Get Involved? How To Get Them InvolvedSignup LettersNessuna valutazione finora
- Speech-Language Therapy For Autistic ChildrenDocumento4 pagineSpeech-Language Therapy For Autistic ChildrenRei YoshiharaNessuna valutazione finora
- Auditory Verbal Therapy Strategies BinderDocumento14 pagineAuditory Verbal Therapy Strategies Binderapi-582670604100% (1)
- Speech ComperhensionDocumento6 pagineSpeech ComperhensionAmal Xlalu DisalahkanNessuna valutazione finora
- 10 Language-Building Tips For Parents of Young Children Who Communicate Without Words (1) HanenCenterDocumento2 pagine10 Language-Building Tips For Parents of Young Children Who Communicate Without Words (1) HanenCenterShoNessuna valutazione finora
- Sharing Books With ToddlersDocumento3 pagineSharing Books With ToddlersStephanie García EscobarNessuna valutazione finora
- Hanen Tips EnglishDocumento6 pagineHanen Tips EnglishGökçe Gökçümen KocaNessuna valutazione finora
- Imaginative PlayDocumento2 pagineImaginative Playshabana waseemNessuna valutazione finora
- Infant ToddlerDocumento54 pagineInfant ToddlerefiadityaNessuna valutazione finora
- 3.8.12.4 Speech BackgroundDocumento7 pagine3.8.12.4 Speech BackgroundErsya MuslihNessuna valutazione finora
- Pediatric Feeding Disorder Consensus DefinitiDocumento23 paginePediatric Feeding Disorder Consensus DefinitiSilvina DurhandNessuna valutazione finora
- Speech and Language StudiesDocumento17 pagineSpeech and Language StudiesafrawrrNessuna valutazione finora
- Lesson 1 - CVC Words - Lesson PlanDocumento5 pagineLesson 1 - CVC Words - Lesson Planapi-549445196Nessuna valutazione finora
- Autism Preparation Kit For Teachers PreviewDocumento12 pagineAutism Preparation Kit For Teachers PreviewRoli RoliNessuna valutazione finora
- Texture ProgressionDocumento26 pagineTexture ProgressionnaomikapaunNessuna valutazione finora
- Time to Talk: What You Need to Know About Your Child's Speech and Language DevelopmentDa EverandTime to Talk: What You Need to Know About Your Child's Speech and Language DevelopmentValutazione: 5 su 5 stelle5/5 (3)
- Visualization PDFDocumento2 pagineVisualization PDFrobbin91Nessuna valutazione finora
- Occupational Therapists Prefer Combining PDFDocumento12 pagineOccupational Therapists Prefer Combining PDFSuperfixenNessuna valutazione finora
- Activities To Focus Attention On Listening and Spoken Language SkillsDocumento10 pagineActivities To Focus Attention On Listening and Spoken Language SkillsAeindray100% (2)
- The Early Years Communication Handbook: A practical guide to creating a communication friendly settingDa EverandThe Early Years Communication Handbook: A practical guide to creating a communication friendly settingNessuna valutazione finora
- 161 Basic ConceptsDocumento3 pagine161 Basic Conceptsilham ilahiNessuna valutazione finora
- The Late Talker: What to Do If Your Child Isn't Talking YetDa EverandThe Late Talker: What to Do If Your Child Isn't Talking YetValutazione: 4 su 5 stelle4/5 (4)
- Petrochemical Processes HandbookDocumento209 paginePetrochemical Processes HandbookAnoop Uchagawkar100% (6)
- Fernando Fonseca Teacher PortfolioDocumento24 pagineFernando Fonseca Teacher PortfolioferfonsegonNessuna valutazione finora
- Get Ready To Read Screening ToolDocumento6 pagineGet Ready To Read Screening ToolmvmbappleNessuna valutazione finora
- Meeting Special Needs: A practical guide to support children with Speech, Language and Communication Needs (SLCN)Da EverandMeeting Special Needs: A practical guide to support children with Speech, Language and Communication Needs (SLCN)Nessuna valutazione finora
- 7 Easy Tips for Preparing Your Child for Success in School Through Play: The Baby Care Book Bundle, #1Da Everand7 Easy Tips for Preparing Your Child for Success in School Through Play: The Baby Care Book Bundle, #1Nessuna valutazione finora
- Developing Speaking SkillsDocumento7 pagineDeveloping Speaking SkillsEdén Verde Educación Con Salud0% (1)
- Day 1 EcosystemDocumento4 pagineDay 1 EcosystemGecel Tepace50% (2)
- Get Your Child Talking - Now ! Speaking with Words: A Guide and E-Workbook to Teach Autistic and Nonverbal Children to TalkDa EverandGet Your Child Talking - Now ! Speaking with Words: A Guide and E-Workbook to Teach Autistic and Nonverbal Children to TalkNessuna valutazione finora
- L2-Stat. Prob - Distinguishing Between Discrete and Continuous Random VariableDocumento7 pagineL2-Stat. Prob - Distinguishing Between Discrete and Continuous Random VariableRene Mulleta DueñasNessuna valutazione finora
- 100 Years Werner HeisenbergDocumento308 pagine100 Years Werner Heisenbergmvmbapple100% (3)
- 1 - Imp - The-Speech-and-Language-EvaluationDocumento5 pagine1 - Imp - The-Speech-and-Language-EvaluationMuskaan KhannaNessuna valutazione finora
- VC VC VC VC: Click On Your Question:cDocumento10 pagineVC VC VC VC: Click On Your Question:cNurul IqasNessuna valutazione finora
- Name: - Date: - Person CompletingDocumento2 pagineName: - Date: - Person CompletingmvmbappleNessuna valutazione finora
- The Autistic AdultDocumento42 pagineThe Autistic Adultmvmbapple0% (1)
- Rain, Rain, Go Away, Come Again Another Day, Little Johnny Wants To PlayDocumento1 paginaRain, Rain, Go Away, Come Again Another Day, Little Johnny Wants To Playmvmbapple0% (1)
- Time LearningDocumento3 pagineTime LearningmvmbappleNessuna valutazione finora
- Kids SafetyDocumento11 pagineKids SafetythirdrockNessuna valutazione finora
- Creating Early Learning PassportDocumento2 pagineCreating Early Learning PassportmvmbappleNessuna valutazione finora
- Classroom InstructionDocumento2 pagineClassroom InstructionmvmbappleNessuna valutazione finora
- Mrs Cats New HatDocumento3 pagineMrs Cats New HatmvmbappleNessuna valutazione finora
- Integrating Technology in CurriculumDocumento3 pagineIntegrating Technology in CurriculummvmbappleNessuna valutazione finora
- Tools For Monitoring Langguage SkillsDocumento16 pagineTools For Monitoring Langguage SkillsmvmbappleNessuna valutazione finora
- Books and MaterialsDocumento5 pagineBooks and MaterialsmvmbappleNessuna valutazione finora
- PDocumento3 paginePErika IlaganNessuna valutazione finora
- Happy Birthday, Mr. Lincoln!: Answer The Questions About Abraham LincolnDocumento1 paginaHappy Birthday, Mr. Lincoln!: Answer The Questions About Abraham LincolnmvmbappleNessuna valutazione finora
- Flash CardDocumento6 pagineFlash CardmvmbappleNessuna valutazione finora
- Tutor Teaching Tips 3Documento12 pagineTutor Teaching Tips 3mvmbappleNessuna valutazione finora
- Instruction On Manipulative On DiskDocumento12 pagineInstruction On Manipulative On DiskmvmbappleNessuna valutazione finora
- Different ShapesDocumento5 pagineDifferent ShapesmvmbappleNessuna valutazione finora
- PDF Created With Fineprint Pdffactory Trial VersionDocumento6 paginePDF Created With Fineprint Pdffactory Trial VersionmvmbappleNessuna valutazione finora
- Lesson in MoneyDocumento2 pagineLesson in MoneymvmbappleNessuna valutazione finora
- Roles of Reading SpecialistDocumento5 pagineRoles of Reading SpecialistmvmbappleNessuna valutazione finora
- Word CardDocumento1 paginaWord CardmvmbappleNessuna valutazione finora
- Aft ToolkitDocumento92 pagineAft ToolkitNatalia RiquelmeNessuna valutazione finora
- Reading Indicators CecklistDocumento4 pagineReading Indicators CecklistmvmbappleNessuna valutazione finora
- Essential Elements in Literacy InstructionsDocumento3 pagineEssential Elements in Literacy InstructionsmvmbappleNessuna valutazione finora
- Literacy DevelopmentDocumento4 pagineLiteracy DevelopmentmvmbappleNessuna valutazione finora
- Young Adoloscent LiteracyDocumento3 pagineYoung Adoloscent LiteracymvmbappleNessuna valutazione finora
- Pneumonic InstructionDocumento10 paginePneumonic InstructionmvmbappleNessuna valutazione finora
- Smart+Planet+1 LessonProgramme LOMCE 2015 EngDocumento281 pagineSmart+Planet+1 LessonProgramme LOMCE 2015 Engperis1404Nessuna valutazione finora
- Classroom Management PlanDocumento2 pagineClassroom Management Planapi-307027477Nessuna valutazione finora
- Various Types of TestDocumento2 pagineVarious Types of Testszcha chaNessuna valutazione finora
- Mengenali Fungsi Logika "And" Melalui Pemrograman Perceptron Dengan MatlabDocumento8 pagineMengenali Fungsi Logika "And" Melalui Pemrograman Perceptron Dengan MatlabGeofanggaNessuna valutazione finora
- ACP Lesson Plan TemplateDocumento3 pagineACP Lesson Plan Templateapi-316651663Nessuna valutazione finora
- Mathematics - Demo Number 2Documento3 pagineMathematics - Demo Number 2Hiezel G LandichoNessuna valutazione finora
- Essay BeasiswaDocumento3 pagineEssay BeasiswaBENNY WAHYUDINessuna valutazione finora
- RPH Bi Year 6 - 25th Jan 2022Documento2 pagineRPH Bi Year 6 - 25th Jan 2022malarNessuna valutazione finora
- Creating EPortfolio As A Technology ToolDocumento56 pagineCreating EPortfolio As A Technology ToolTrisha CenitaNessuna valutazione finora
- Cecilia A. CastilloDocumento2 pagineCecilia A. CastilloEr IcNessuna valutazione finora
- Apprenticeship and Exploration of The Perfroming Arts (Theater)Documento5 pagineApprenticeship and Exploration of The Perfroming Arts (Theater)jay jayNessuna valutazione finora
- Walter Reviwer 1prof Ed 2Documento13 pagineWalter Reviwer 1prof Ed 2riza cabugnaoNessuna valutazione finora
- Dynamic Social Studies Lesson (Real)Documento3 pagineDynamic Social Studies Lesson (Real)api-282757658Nessuna valutazione finora
- How Can You Enhance The State of Quality Teachers in The Philippines?Documento3 pagineHow Can You Enhance The State of Quality Teachers in The Philippines?Darlene Dacanay DavidNessuna valutazione finora
- Davangere University: Institute of Management StudiesDocumento5 pagineDavangere University: Institute of Management StudiesVenki GajaNessuna valutazione finora
- SGC Governance Council Action PlanDocumento5 pagineSGC Governance Council Action PlanMAILYN PREMARIONNessuna valutazione finora
- Term 2 Civics and Citizenship Unit PlanDocumento6 pagineTerm 2 Civics and Citizenship Unit Planapi-354656077Nessuna valutazione finora
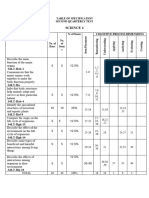
- Tos Science 4Documento2 pagineTos Science 4Val AtienzaNessuna valutazione finora
- Course Syllabus Life and Works of Dr. Jose Rizal Course DescriptionDocumento7 pagineCourse Syllabus Life and Works of Dr. Jose Rizal Course Descriptionjonalyn obinaNessuna valutazione finora
- Objectives-WPS OfficeDocumento4 pagineObjectives-WPS Officefrance cruzNessuna valutazione finora
- Integer Lesson PlanDocumento2 pagineInteger Lesson PlanWilliam BaileyNessuna valutazione finora
- Cot - DLP - English 2 by Teacher Jelyn M. HabanaDocumento2 pagineCot - DLP - English 2 by Teacher Jelyn M. HabanaMiljun Lacbayo100% (2)
- Epsy 2130 Fall 2015 SyllabusDocumento5 pagineEpsy 2130 Fall 2015 Syllabusapi-283935863Nessuna valutazione finora
- Lesson Plan Unit 5 - ReadingDocumento3 pagineLesson Plan Unit 5 - ReadingChánh Nguyễn Hoàng TrungNessuna valutazione finora