Hospital Prices: Who is the Real Victim?
Setting Defensible Prices
Written by
William O. Cleverley, PhD James O. Cleverley, MHA
Cleverley + Associates 438 e wilson bridge road, suite 200 Worthington, oh 43085 888-779-5663 info@cleverleyassociates.com
Hospital Prices: Who is the Real Victim?
Pricing Transparency
The dialogue surrounding hospital pricing transparency has done little to bring clarity to the issue for health consumers. In fact, the increased attention has led to added ambiguity at a time when greater understanding is required. Quite simply, hospital pricing is complex. The country seems headed for hospital-pricing disclosure. Take into consideration the following evidence: In March US Department of Health and Human Services secretary Mike Leavitt announced plans to post the prices it pays for common medical procedures. The effort has been linked to a White House initiative for increased publication of healthcare pricing and quality data. Representatives Daniel Lipinski (D-IL) and Bob Inglis (R-SC) introduced legislation last July under the heading of the Hospital Price Reporting and Disclosure Act. The bipartisan effort is currently being considered and, if enacted, would require hospitals to report pricing for their twenty-five most commonly performed inpatient and outpatient procedures as well as their fifty most frequently administered medications. Several states have already passed similar legislation, and several more are in the process. Certainly, the reality of pricing transparency is gaining momentum. While legislative efforts at the state and national levels have added logs to fire, other private groups have become involved as well.
2006 Cleverley + Associates
Hospital Prices: Who is the Real Victim?
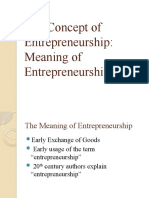
Figure 1. hospitalvictims.com/hv_hosp_main.asp?mpn=360180
Cleveland Clinic Hospital (Cleveland, OH) charges 373% times its costs. That is 301% times what Johns Hopkins charges!
On average, Cleveland Clinic Hospital charges 3.0 times what Johns Hopkins charges, ranked the finest hospital in America. Look at the price comparisons of Johns Hopkins versus Cleveland Clinic Hospital .
124% 373%
Compare Overall Compare Ancillary Services
JOHNS HOPKINS HOSPITAL: The reason for comparing to Johns Hopkins Hospital? It is one of the finest hospitals in America. If they don't overcharge, why should your hospital
Mark Up Cleveland Clinic Hospital vs. Johns Hopkins
Cleveland Clinic Hospital list prices are outrageous. On average Cleveland Clinic Hospital grants a 62% discount to people with insurance. How much of a discount did they give you?
If Johns Hopkins is the best hospital in America, why is this hospital so much more expensive?
A significant amount of the increased public attention to pricing is related to the web site, hospitalvictims.com shown above. A number of our clients have contacted us regarding this site, complaining about the validity of the data presented and the increased use of the web site by patients, payers, and other interested parties. Upon review of the web site, we discovered a number of very interesting points: 1. The web site is maintained by Fairness Foundation, Inc., a non-profit tax-exempt 501(C)3 organization. This organization was founded in 1998 to assist low-income children in getting access to better education and to assist the uninsured in getting good healthcare. 2. The Fairness Foundation, Inc., was founded by J. Patrick Rooney, who was the former chairman and chief executive office of Golden Rule Insurance Company.
2006 Cleverley + Associates
Hospital Prices: Who is the Real Victim?
Golden Rule is described in the web sites biography of Mr. Rooney as the largest insurer of individual health policies in the country. After leaving Golden Rule, Mr. Rooney acquired Medical Savings Insurance Company (MSIC), of which he is currently chairman and chief executive officer. MSIC sells health policies largely to individuals and small groups. These plans have large deductibles and promote the freedom-of-choice feature in their web sites promotional materials. MSIC contends that it pays all reasonable charges after the deductible is met. Many hospitals may be familiar with MSIC. Usually MSIC does not contract with hospitals and tenders payment on a basis different than charges. Usually, the payment is stated as reasonable because it is related to Medicare payments. 3. The web site states that patients may not have to pay charges. It advocates challenging the reasonableness of the bill under the federal Fair Debt Collection Practices Act. It further offers to provide a letter to be sent to the hospital or its collection agent. 4. Regarding the reasonableness of a hospitals charges, the sites authors explain, If you wish to dispute to the hospital the amount the hospital has charged you, it is important for you to know (a) what the hospitals costs are in relation to what the hospital normally charges; and (b) what Medicare would pay. This statement highlights much of the underlying logic behind the website material. The sites authors believe that the Medicare payment rate is a good beginning point for discussion with the hospital regarding payment and cite Dr. Gerard Anderson of Johns Hopkins Hospital, who has testified before Congress that Medicare plus 25% is more than reasonable. This, of course, bears a similarity to the payment rules that MSIC says it has adopted. 5. The real concern expressed about this web site by our clients is related to the data. The data points provided on the site include: Relationship of charges to cost Relationship of charges for the hospital to charges at Johns Hopkins Hospital Average discount given people with insurance Additional ancillary service-charge comparisons
2006 Cleverley + Associates
Hospital Prices: Who is the Real Victim?
Validity
The data presented in the hospitalvictims.com web site should be reviewed for its accuracy. We believe the primary data used are filed Medicare Cost Reports. Figure 1 presents the actual page printed for the Cleveland Clinic on April 12, 2006. We chose the Cleveland Clinic because, like John Hopkins, the Cleveland Clinic is routinely ranked one of the top five US hospitals: they both have wage indexes close to 1.00, they are similar in size, and both are major teaching hospitals. With this backdrop, let us review the numbers reported and the logic behind them. 1. Website claim: The Cleveland Clinic charges 373% times its costs. Validity: The Cleveland Clinics 2004 Medicare Cost Report shows total gross patient revenue of $3,425,289,832 and total expenses of $918,725,605 from Worksheet G. This yields a mark-up of 3.73, or 373%. 2. Website claim: Charges at Cleveland Clinic are 301% what Johns Hopkins charges. Validity: This statistic is very misleading and simply is not true. The 301% is derived (we believe) by multiplying the Cleveland Clinics costs ($918,725,605) by the average mark-up at Johns Hopkins (1.24) to yield what total charges would have been at the Cleveland Clinic if Johns Hopkins mark-up were used ($1,139,219,750). While this computation may yield a 301% multiple, it is a long way from proving actual charges for identical case-treatment categories are 301% higher at the Cleveland Clinic. The table below shows costs, charges, and payment for Medicare patients in 2004 for the Cleveland Clinic and Johns Hopkins. One set of values is for all Medicare inpatient cases on a case-mix-adjusted basis, and the other set is for the highest volume Medicare DRG (# 127 heart failure & shock) Johns Hopkins $12,292 9,601 11,358 $12,384 9,568 10,726 Cleveland Clinic $18,717 6,279 6,402 $20,180 7,149 6,511
Average charge (CMI adj) Average cost (CMI adj) Average payment (CMI adj) DRG 127 charge (CMI adj) DRG 127 cost (CMI adj) DRG 127 payment (CMI adj)
All US $15,241 6,267 5,667 $15,357 6,701 5,502
The data above show charges at the Cleveland Clinic are not 301% of charges at Johns Hopkins; on average, they are 152%. That 152% is still large, but it is a far cry from 301%. It is also interesting to compare costs. Johns Hopkins is not a low-cost provider. It is 53% above the Cleveland Clinic. Why, then, can charges at Johns Hopkins be so low when costs are so high? The answer relates to Medicare payment in Maryland. Medicare pays 94% of charges in this rate-regulated state, as does Medicaid. Furthermore, other payers in Maryland pay either 98% or 100% of charges. Is it any wonder charges are so low in Maryland in general and at Johns Hopkins in particular? Johns Hopkins is clearly receiving significantly larger payments for its Medicare and Medicaid patients than are other US hospitals. Because of these larger payments, charges can be significantly lower. In short, Johns Hopkins is receiving a subsidy from the US taxpayer that other hospitals do not receive.
3. Website claim: On average, Cleveland Clinic grants a 62% discount to people with
insurance.
2006 Cleverley + Associates
Hospital Prices: Who is the Real Victim?
Validity: The 62% figure cited in the web site is the ratio of deductions to gross patient revenue reported in Worksheet G of the Medicare Cost Report. The number includes discounts to both Medicaid and Medicare patients, which are clearly not commercial insurance programs. While discounts to commercial insurance patients are high, they are usually substantially less than Medicaid and Medicare allowances. By citing this statistic, the inference being made is that individuals or insurance firms without contracts should get hospital discounts that will be better than most commercial insurance firms, who have negotiated a hospital contract, receive.
The Real Problem
There is no question regarding the relative relationship of hospital charges to cost. Everyone recognizes that hospitals have very high mark-ups. The problem, however, is not hospital prices but rather payment rates by major third-party payers. The table below provides a simple example to illustrate an issue that is painfully obvious to most hospital executives. In our example, the hospital has 100 patients who each incur costs of $100 per treatment episode (total costs of $10,000). The hospital also requires a 4% margin ($400) to provide for working capital and capital-replacement needs. Revenue Medicare (50 patients at $92.50) Medicaid (13 patients at $75.00) Uninsured (5 patients at $5.00) Total revenue before commercial Cost and required profit Amount required from 32 commercial patients Amount required per case $4,625 975 25 $5,625 $10,400 $4,775 $149.22
The payment rate for Medicare ($92.50) is the MedPAC estimated Medicare amount in 2004 for non-teaching hospitals (Table 2A-6, March 2006 Report to the Congress Medicare Payment Policy). The distribution of patients is similar to the revenue composition of US acute-care hospitals in 2004. The table shows that if all commercial patients paid 100% of charges, the mark-up would be 149.22%. The reality for most hospitals is that a small portion actually pay at that rate. Assume that of the 32 commercial patients, 28 pay at levels that are approximately 125% of cost, given existing negotiated contracts (total payment of $3,500). MedPAC reported the private payer payment-to-cost ratio was approximately 1.25 in 2003 (Figure 2A-10). This now leaves $1,275 to be paid by the remaining four patients, or $318.75 per case. Charges or prices in our example are 318.75% of cost, but the hospital has a modest 4% margin. Some would argue this proves that hospital prices are not related to cost, but this is clearly not true. Hospital prices are directly tied to costs. The problem is that payment rates by major governmental programs and the rising incidence of uninsured patients create a very large payment gap that is covered by a majority of patients.
2006 Cleverley + Associates
Hospital Prices: Who is the Real Victim?
Summary
Perhaps the Fairness Foundation should consider a name change for its web site from hospitalvictims.com to payervictims.com. The underlying issue is not hospital pricing but hospital payment. The use of Johns Hopkins Hospital as the standard for other hospitals points this out very clearly. When every payer pays between 94% and 100% of billed charges, as they do in Maryland, the relationship of price to cost will resemble mark-ups in other industries.
2006 Cleverley + Associates
Potrebbero piacerti anche
- The Paradox of IdentityDocumento14 pagineThe Paradox of IdentityWilliam J GreenbergNessuna valutazione finora
- The Detroit BankruptcyDocumento60 pagineThe Detroit BankruptcyWilliam J GreenbergNessuna valutazione finora
- Dialetheism in The Era of Philbert Phlurk Logics: A Prelutskian Reflection On Sylvan and PriestDocumento2 pagineDialetheism in The Era of Philbert Phlurk Logics: A Prelutskian Reflection On Sylvan and PriestWilliam J GreenbergNessuna valutazione finora
- FallibilismDocumento2 pagineFallibilismWilliam J GreenbergNessuna valutazione finora
- Dialetheist Truth-TablesDocumento1 paginaDialetheist Truth-TablesWilliam J GreenbergNessuna valutazione finora
- Here's Why Plutocrats Control Our PoliticsDocumento5 pagineHere's Why Plutocrats Control Our PoliticsWilliam J GreenbergNessuna valutazione finora
- Graham Priest's Theory of ChangeDocumento4 pagineGraham Priest's Theory of ChangeWilliam J GreenbergNessuna valutazione finora
- Noam Chomsky: 'The Foundations of Liberty Are Ripped To Shreds'Documento9 pagineNoam Chomsky: 'The Foundations of Liberty Are Ripped To Shreds'William J GreenbergNessuna valutazione finora
- 02-10-13 Edward Snowden's E-Mail Provider Defied FBI Demands To Turn Over Crypto Keys, Documents ShowDocumento5 pagine02-10-13 Edward Snowden's E-Mail Provider Defied FBI Demands To Turn Over Crypto Keys, Documents ShowWilliam J GreenbergNessuna valutazione finora
- The Plot Against PensionsDocumento32 pagineThe Plot Against PensionsRobert JohnsonNessuna valutazione finora
- 22-07-13 How Big Finance Crushes Innovation and Holds Back Our EconomyDocumento8 pagine22-07-13 How Big Finance Crushes Innovation and Holds Back Our EconomyWilliam J GreenbergNessuna valutazione finora
- Dancing With Professors: The Trouble With Academic ProseDocumento7 pagineDancing With Professors: The Trouble With Academic ProseWilliam J Greenberg100% (2)
- 18-09-13 Underpaid 83-Year-Old Professor Died Trying To Make Ends Meet by Working Night Shift at Eat An' SaveDocumento4 pagine18-09-13 Underpaid 83-Year-Old Professor Died Trying To Make Ends Meet by Working Night Shift at Eat An' SaveWilliam J GreenbergNessuna valutazione finora
- 24-08-13 Chomsky: The U.S. Behaves Nothing Like A Democracy, But You'll Never Hear About It in Our 'Free Press'Documento19 pagine24-08-13 Chomsky: The U.S. Behaves Nothing Like A Democracy, But You'll Never Hear About It in Our 'Free Press'William J GreenbergNessuna valutazione finora
- Hedge Fund Billionaire: Fed's Move 'Fantastic' For The Rich: Federal ReserveDocumento10 pagineHedge Fund Billionaire: Fed's Move 'Fantastic' For The Rich: Federal ReserveWilliam J GreenbergNessuna valutazione finora
- 12-04-13 Wikileaks Releases Kissinger Cables and Two Decisions in Manning TrialDocumento12 pagine12-04-13 Wikileaks Releases Kissinger Cables and Two Decisions in Manning TrialWilliam J GreenbergNessuna valutazione finora
- 19-07-13 UK's Blood Supply To Be Sold To Bain CapitalDocumento2 pagine19-07-13 UK's Blood Supply To Be Sold To Bain CapitalWilliam J GreenbergNessuna valutazione finora
- Philosophy Talk: The Prison SystemDocumento3 paginePhilosophy Talk: The Prison SystemWilliam J GreenbergNessuna valutazione finora
- 11-07-13 Walmart Threatens To Leave Washington DC Over City's LRAA Living Wage' MandateDocumento4 pagine11-07-13 Walmart Threatens To Leave Washington DC Over City's LRAA Living Wage' MandateWilliam J GreenbergNessuna valutazione finora
- 19-07-13 The Grand Scam: Spinning Egypt's Military CoupDocumento10 pagine19-07-13 The Grand Scam: Spinning Egypt's Military CoupWilliam J GreenbergNessuna valutazione finora
- Egyptian Turmoil Brings Greater Suffering in Gaza: War Dollars HomeDocumento3 pagineEgyptian Turmoil Brings Greater Suffering in Gaza: War Dollars HomeWilliam J GreenbergNessuna valutazione finora
- Should We Give Pot To Suffering Pets? Animal Expert Darlene Arden Says YesDocumento5 pagineShould We Give Pot To Suffering Pets? Animal Expert Darlene Arden Says YesWilliam J GreenbergNessuna valutazione finora
- Racism and The Aesthetic of Hyperreal Violence (Giroux 1995)Documento19 pagineRacism and The Aesthetic of Hyperreal Violence (Giroux 1995)William J GreenbergNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Club Amigos Caravan Park:: Contact Persons: Pieter and Sonja Van WykDocumento2 pagineClub Amigos Caravan Park:: Contact Persons: Pieter and Sonja Van WykRobNessuna valutazione finora
- Cambridge O Level: Accounting 7707/22 October/November 2022Documento16 pagineCambridge O Level: Accounting 7707/22 October/November 2022Marlene BandaNessuna valutazione finora
- Management Accounting Level 3/series 2-2009Documento16 pagineManagement Accounting Level 3/series 2-2009Hein Linn Kyaw100% (1)
- DERVFOP - Lecture 3 (Hedging Strategies Using Futures)Documento29 pagineDERVFOP - Lecture 3 (Hedging Strategies Using Futures)RedNessuna valutazione finora
- Fundamental Analysis of FMCG Sector Ashish Chanchlani PDFDocumento61 pagineFundamental Analysis of FMCG Sector Ashish Chanchlani PDFSAKSHI KHAITAN0% (1)
- Iim Calcutta - Job Description Form: Name of The Firm ICICI Bank LTDDocumento2 pagineIim Calcutta - Job Description Form: Name of The Firm ICICI Bank LTDAmit KohadNessuna valutazione finora
- W. Edwards Deming's 14 PointsDocumento4 pagineW. Edwards Deming's 14 PointsAr'anne ZabalaNessuna valutazione finora
- Assignment of PoonamDocumento73 pagineAssignment of PoonamPinky ChowdhuryNessuna valutazione finora
- Overpopulation and Its Economic EffectsDocumento8 pagineOverpopulation and Its Economic EffectsGeriHalliwellNessuna valutazione finora
- Over Not Over Tax: Basic Income Table (Tax Code, Section 24 A)Documento2 pagineOver Not Over Tax: Basic Income Table (Tax Code, Section 24 A)Juliana ChengNessuna valutazione finora
- Intermediate Accounting: Non-Financial and Current LiabilitiesDocumento79 pagineIntermediate Accounting: Non-Financial and Current LiabilitiesShuo LuNessuna valutazione finora
- Book 1Documento2 pagineBook 1agus suyadiNessuna valutazione finora
- Offer Letter - SameerDocumento3 pagineOffer Letter - SameerAshwin SupeNessuna valutazione finora
- Corporate Social ResponsibilityDocumento8 pagineCorporate Social ResponsibilityJustin Miguel IniegoNessuna valutazione finora
- Summer Internship Report at Future Generali Insurance LTDDocumento44 pagineSummer Internship Report at Future Generali Insurance LTDpratiksha2467% (3)
- Peter LynchDocumento2 paginePeter LynchShiv PratapNessuna valutazione finora
- Full Solution Manual For South Western Federal Taxation 2019 Individual Income Taxes 42Nd Edition James C Young PDF Docx Full Chapter ChapterDocumento11 pagineFull Solution Manual For South Western Federal Taxation 2019 Individual Income Taxes 42Nd Edition James C Young PDF Docx Full Chapter Chaptershrunkenyojan6amf2100% (17)
- Assignment No 1Documento8 pagineAssignment No 1manesh1234Nessuna valutazione finora
- CH 16Documento10 pagineCH 16Daniel Caesar PanjaitanNessuna valutazione finora
- The Zimbabwean DollarDocumento4 pagineThe Zimbabwean DollarDeepak NadarNessuna valutazione finora
- Auditing and Consulting Business PlanDocumento36 pagineAuditing and Consulting Business PlanHACHALU FAYE0% (1)
- Sinking FundDocumento11 pagineSinking FundSrit MechNessuna valutazione finora
- Growth and Prospects of Odisha Tourism An Empirical StudyDocumento4 pagineGrowth and Prospects of Odisha Tourism An Empirical StudyAshis Kumar MohapatraNessuna valutazione finora
- Ssm-Arry Urus SDN Bhd-Mar17Documento6 pagineSsm-Arry Urus SDN Bhd-Mar17xidaNessuna valutazione finora
- Full Download Test Bank For Labour Relations 5th by Suffield PDF Full ChapterDocumento36 pagineFull Download Test Bank For Labour Relations 5th by Suffield PDF Full Chapteralbigeoisungeld.5h2u100% (21)
- 6 - Working Capital ManagementDocumento4 pagine6 - Working Capital ManagementChristian LimNessuna valutazione finora
- The Concept of Entrepreneurship - Entrep BehaviorDocumento27 pagineThe Concept of Entrepreneurship - Entrep BehaviorEmmanuel BurcerNessuna valutazione finora
- Correction of ErrorsDocumento15 pagineCorrection of ErrorsEliyah Jhonson100% (1)
- Economics PDFDocumento44 pagineEconomics PDFyesuNessuna valutazione finora
- Siobhan Stewart 92 %Documento2 pagineSiobhan Stewart 92 %Roland Lovelace OpokuNessuna valutazione finora