Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocumento25 pagineFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04Nessuna valutazione finora
- SYNAPSEDocumento35 pagineSYNAPSEkiedd_04100% (3)
- "Traditional" Exegeses of Q 4:34Documento15 pagine"Traditional" Exegeses of Q 4:34kiedd_04Nessuna valutazione finora
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Documento2 pagineIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04Nessuna valutazione finora
- The Place For Others in IslamDocumento27 pagineThe Place For Others in Islamkiedd_04Nessuna valutazione finora
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocumento13 pagineOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- Refleks ArcsDocumento34 pagineRefleks Arcskiedd_04100% (1)
- Fadhilat Surah at TakwirDocumento1 paginaFadhilat Surah at Takwirkiedd_04Nessuna valutazione finora
- Cell PhysiologyDocumento61 pagineCell Physiologykiedd_04100% (4)
- Microbiology Colour Plate No.8Documento1 paginaMicrobiology Colour Plate No.8kiedd_04Nessuna valutazione finora
- Microbiology Colour Plate No.6Documento1 paginaMicrobiology Colour Plate No.6kiedd_04Nessuna valutazione finora
- API® CoryneDocumento4 pagineAPI® Corynekiedd_04Nessuna valutazione finora
- Microbiology Colour Plate No.7Documento1 paginaMicrobiology Colour Plate No.7kiedd_04Nessuna valutazione finora
- Microbiology Colour Plate No.4Documento1 paginaMicrobiology Colour Plate No.4kiedd_04Nessuna valutazione finora
- Microbiology Colour Plate No.3Documento1 paginaMicrobiology Colour Plate No.3kiedd_04Nessuna valutazione finora
- Microbiology Colour Plate No.9Documento1 paginaMicrobiology Colour Plate No.9kiedd_04Nessuna valutazione finora
- Microbiology Colour Plate No.5Documento1 paginaMicrobiology Colour Plate No.5kiedd_04Nessuna valutazione finora
- Microbiology Colour Plate No.1Documento1 paginaMicrobiology Colour Plate No.1kiedd_04Nessuna valutazione finora
- Microbiology Colour Plate No.2Documento1 paginaMicrobiology Colour Plate No.2kiedd_04Nessuna valutazione finora
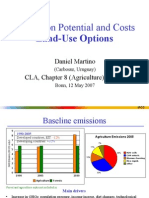
- Mitigation Potential and Costs Land-Use OptionsDocumento9 pagineMitigation Potential and Costs Land-Use Optionskiedd_04Nessuna valutazione finora
- Mitigation of Climate ChangeDocumento41 pagineMitigation of Climate Changekiedd_04Nessuna valutazione finora
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocumento10 paginePhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04Nessuna valutazione finora
- Carnitine DeficiencyDocumento21 pagineCarnitine Deficiencykiedd_04100% (1)
- Mitigation of Climate ChangeDocumento25 pagineMitigation of Climate Changekiedd_04Nessuna valutazione finora
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocumento1 paginaAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
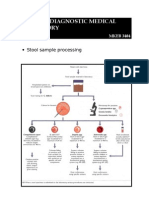
- Stool Sample ProcessingDocumento1 paginaStool Sample Processingkiedd_04Nessuna valutazione finora
- Oxidase TestDocumento1 paginaOxidase Testkiedd_04100% (1)
- Diagram of Classification of EnterobacteriaDocumento1 paginaDiagram of Classification of Enterobacteriakiedd_04100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- What Is Osteopenia?: What Are Causes and Risk Factors For Osteopenia?Documento2 pagineWhat Is Osteopenia?: What Are Causes and Risk Factors For Osteopenia?Jeremy EvansNessuna valutazione finora
- Do Not Substitute Date Time Finger-Stick Blood GlucoseDocumento2 pagineDo Not Substitute Date Time Finger-Stick Blood GlucoserizukichanNessuna valutazione finora
- Science 10 Quarter 3 Module 3Documento15 pagineScience 10 Quarter 3 Module 3Zahra Alexä DavidsonNessuna valutazione finora
- First Summative Test in SCIENCE 5 2nd QuarterDocumento2 pagineFirst Summative Test in SCIENCE 5 2nd QuarterGrace Cruz Delos Reyes89% (9)
- Digital Tools For Managing DiabetesDocumento1 paginaDigital Tools For Managing DiabetesTaufiqurrokhman RofiiNessuna valutazione finora
- The Multiple Roles of Life Stress in Metabolic DisordersDocumento18 pagineThe Multiple Roles of Life Stress in Metabolic DisordersArgenis SalinasNessuna valutazione finora
- Daftar PustakaDocumento3 pagineDaftar PustakaAtin AtinNessuna valutazione finora
- BE02: Anatomy and Physiology of The Lactating Breast WorkbookDocumento5 pagineBE02: Anatomy and Physiology of The Lactating Breast WorkbookSyed Hussain AsafNessuna valutazione finora
- Sexual Reproduction in Humans Notes (CAPE)Documento29 pagineSexual Reproduction in Humans Notes (CAPE)Desmond JonesNessuna valutazione finora
- New Microsoft Office Word DocumentDocumento16 pagineNew Microsoft Office Word DocumentDavid LeeNessuna valutazione finora
- Thyroid Hormones: Thyroid Gland - Structure and FunctionDocumento11 pagineThyroid Hormones: Thyroid Gland - Structure and FunctionWaleed W Al-AzharyNessuna valutazione finora
- Physiology of Menstrual CycleDocumento2 paginePhysiology of Menstrual CycleAmiel simon NgoNessuna valutazione finora
- Neonatal HyperglycemiaDocumento18 pagineNeonatal HyperglycemiayumicheongNessuna valutazione finora
- Reiki Level 1 ManualDocumento29 pagineReiki Level 1 ManualFabian DeeNessuna valutazione finora
- Preboards 2 - NP3 (Printable)Documento10 paginePreboards 2 - NP3 (Printable)Joana Marie DomingoNessuna valutazione finora
- (Dwarfism) : Regents BiologyDocumento23 pagine(Dwarfism) : Regents BiologyReshu ThakuriNessuna valutazione finora
- Thyroid by Dr. Shyam Kalavalapalli, Endocrinologist, HyderabadDocumento87 pagineThyroid by Dr. Shyam Kalavalapalli, Endocrinologist, HyderabadSherman BellNessuna valutazione finora
- Thyroid Storm - Mary L SchreiberDocumento4 pagineThyroid Storm - Mary L Schreibervanny leutualyNessuna valutazione finora
- Case Study 52 Cushing SyndromDocumento2 pagineCase Study 52 Cushing SyndromJoshua del PozoNessuna valutazione finora
- Q3 Science Reviewer - PopoDocumento10 pagineQ3 Science Reviewer - PopoXY PLAYZNessuna valutazione finora
- Hipofisis 7Documento13 pagineHipofisis 7RafaelPetitNessuna valutazione finora
- Diabetes TutorialDocumento3 pagineDiabetes TutorialmorsiNessuna valutazione finora
- Science 5 DLP 3 - PubertyDocumento8 pagineScience 5 DLP 3 - PubertyMark Cua100% (4)
- Testosterone Total and FreeDocumento9 pagineTestosterone Total and FreeRobert Gerald RaoNessuna valutazione finora
- Study Guide Unit 13 "Reproductive System" 1Documento4 pagineStudy Guide Unit 13 "Reproductive System" 1Christopher EstevezNessuna valutazione finora
- Oet WritingDocumento5 pagineOet WritingEloiseBalasbas50% (2)
- Diabetes InsipidusDocumento8 pagineDiabetes InsipidusNader Smadi100% (5)
- Greendale-1999-The MenopauseDocumento10 pagineGreendale-1999-The MenopauseRya RatnaNessuna valutazione finora
- Exocrine Glands-Endocrine GlandsDocumento8 pagineExocrine Glands-Endocrine GlandsneerleoNessuna valutazione finora
- Menstrual Cycle and Physical Performance of Female AthletesDocumento3 pagineMenstrual Cycle and Physical Performance of Female AthletesBiee BarbNessuna valutazione finora