Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- 1986 Elektric M InfoDocumento1 pagina1986 Elektric M InfoDanielDiasNessuna valutazione finora
- Dental Management of Medically Compromised PatientsDocumento12 pagineDental Management of Medically Compromised Patientsمحمد ابوالمجدNessuna valutazione finora
- Etiology of MalocclusionDocumento28 pagineEtiology of MalocclusionPriyaancaHaarsh100% (3)
- Entrenamiento 3412HTDocumento1.092 pagineEntrenamiento 3412HTWuagner Montoya100% (5)
- MCQPaperSept 05Documento4 pagineMCQPaperSept 05api-26291651100% (1)
- Introduction To Philosophy of The Human Person: Presented By: Mr. Melvin J. Reyes, LPTDocumento27 pagineIntroduction To Philosophy of The Human Person: Presented By: Mr. Melvin J. Reyes, LPTMelvin J. Reyes100% (2)
- Biologic Width - The No Encroachment Zone: I J D ADocumento8 pagineBiologic Width - The No Encroachment Zone: I J D AJinny ShawNessuna valutazione finora
- MCQSeptember 2006 Paper IDocumento3 pagineMCQSeptember 2006 Paper Iapi-26291651100% (1)
- Grammar For TOEFLDocumento23 pagineGrammar For TOEFLClaudia Alejandra B0% (1)
- Gamboa Vs Chan 2012 Case DigestDocumento2 pagineGamboa Vs Chan 2012 Case DigestKrissa Jennesca Tullo100% (2)
- Reply To Pieta MR SinoDocumento9 pagineReply To Pieta MR SinoBZ RigerNessuna valutazione finora
- ChemFil Superior44Documento27 pagineChemFil Superior44محمد ابوالمجدNessuna valutazione finora
- 4 3 937Documento4 pagine4 3 937محمد ابوالمجدNessuna valutazione finora
- VitaminsDocumento13 pagineVitaminsمحمد ابوالمجدNessuna valutazione finora
- Guidelines On Infection Control in Dental ClinicsDocumento10 pagineGuidelines On Infection Control in Dental ClinicsHare RamNessuna valutazione finora
- VitaminsDocumento13 pagineVitaminsمحمد ابوالمجدNessuna valutazione finora
- Publication PDFDocumento28 paginePublication PDFمحمد ابوالمجدNessuna valutazione finora
- Dental Anatomy DecksDocumento362 pagineDental Anatomy Decksapi-2629165183% (6)
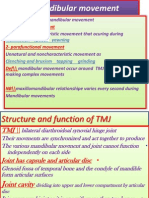
- Mandibular MovementDocumento4 pagineMandibular Movementمحمد ابوالمجدNessuna valutazione finora
- Dental Cements For UseDocumento28 pagineDental Cements For UseAhmed DolaNessuna valutazione finora
- Anatomy of CNSDocumento32 pagineAnatomy of CNSLeonita AguillonNessuna valutazione finora
- Serial Extraction PedoDocumento23 pagineSerial Extraction PedoSelim BaftiuNessuna valutazione finora
- Anatomy of CNSDocumento32 pagineAnatomy of CNSLeonita AguillonNessuna valutazione finora
- Publication PDFDocumento20 paginePublication PDFمحمد ابوالمجدNessuna valutazione finora
- Behaviour Management 2Documento59 pagineBehaviour Management 2Nikhil RaiNessuna valutazione finora
- Finishing and PolishingDocumento18 pagineFinishing and Polishingab0maiNessuna valutazione finora
- Smear LayerDocumento9 pagineSmear Layerpriyanka_gedamNessuna valutazione finora
- Emergency MedicineDocumento7 pagineEmergency Medicineمحمد ابوالمجدNessuna valutazione finora
- Mandibular MovementDocumento4 pagineMandibular Movementمحمد ابوالمجدNessuna valutazione finora
- Asnan 7 RulesDocumento2 pagineAsnan 7 Rulesمحمد ابوالمجدNessuna valutazione finora
- DentistryDocumento71 pagineDentistryAnupama NagrajNessuna valutazione finora
- Tooth MovementDocumento14 pagineTooth Movementمحمد ابوالمجدNessuna valutazione finora
- 1Documento15 pagine1محمد ابوالمجدNessuna valutazione finora
- Anatomy of CNSDocumento32 pagineAnatomy of CNSLeonita AguillonNessuna valutazione finora
- RO0111 00-00 WebberDocumento6 pagineRO0111 00-00 WebberARTNessuna valutazione finora
- OcclusionDocumento17 pagineOcclusionمحمد ابوالمجدNessuna valutazione finora
- Diane Mediano CareerinfographicDocumento1 paginaDiane Mediano Careerinfographicapi-344393975Nessuna valutazione finora
- Logo DesignDocumento4 pagineLogo Designdarshan kabraNessuna valutazione finora
- TEsis Doctoral en SuecoDocumento312 pagineTEsis Doctoral en SuecoPruebaNessuna valutazione finora
- BRAC BrochureDocumento2 pagineBRAC BrochureKristin SoukupNessuna valutazione finora
- Grafton Business Services 2023Documento61 pagineGrafton Business Services 2023Vigh ZsoltNessuna valutazione finora
- Custom Belt Buckles: Custom Brass Belt Buckles - Hand Made in The USA - Lifetime Guarantee of QualityDocumento1 paginaCustom Belt Buckles: Custom Brass Belt Buckles - Hand Made in The USA - Lifetime Guarantee of QualityAndrew HunterNessuna valutazione finora
- Theo Hermans (Cáp. 3)Documento3 pagineTheo Hermans (Cáp. 3)cookinglike100% (1)
- Maule M7 ChecklistDocumento2 pagineMaule M7 ChecklistRameez33Nessuna valutazione finora
- Curriculum Vitae Mukhammad Fitrah Malik FINAL 2Documento1 paginaCurriculum Vitae Mukhammad Fitrah Malik FINAL 2Bill Divend SihombingNessuna valutazione finora
- Wwe SVR 2006 07 08 09 10 11 IdsDocumento10 pagineWwe SVR 2006 07 08 09 10 11 IdsAXELL ENRIQUE CLAUDIO MENDIETANessuna valutazione finora
- Feuerhahn Funeral Bullet 17 March 2015Documento12 pagineFeuerhahn Funeral Bullet 17 March 2015brandy99Nessuna valutazione finora
- RESO NO. 4 - LANYARD FinalDocumento1 paginaRESO NO. 4 - LANYARD FinalsharonleefulloNessuna valutazione finora
- TestDocumento56 pagineTestFajri Love PeaceNessuna valutazione finora
- Present Continuous WorkshopDocumento5 paginePresent Continuous WorkshopPaula Camila Castelblanco (Jenni y Paula)Nessuna valutazione finora
- International Gustav-Bumcke-Competition Berlin / July 25th - August 1st 2021Documento5 pagineInternational Gustav-Bumcke-Competition Berlin / July 25th - August 1st 2021Raul CuarteroNessuna valutazione finora
- Irregular Verbs-1Documento1 paginaIrregular Verbs-1timas2Nessuna valutazione finora
- Chapter 15 (Partnerships Formation, Operation and Ownership Changes) PDFDocumento58 pagineChapter 15 (Partnerships Formation, Operation and Ownership Changes) PDFAbdul Rahman SholehNessuna valutazione finora
- Test AmeeshDocumento7 pagineTest AmeeshUdit DravidNessuna valutazione finora
- First Aid General PathologyDocumento8 pagineFirst Aid General PathologyHamza AshrafNessuna valutazione finora
- QTP Common FunctionsDocumento55 pagineQTP Common FunctionsAnkur TiwariNessuna valutazione finora
- DMemo For Project RBBDocumento28 pagineDMemo For Project RBBRiza Guste50% (8)
- Fry 2016Documento27 pagineFry 2016Shahid RashidNessuna valutazione finora
- CHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 5Documento4 pagineCHIR12007 Clinical Assessment and Diagnosis Portfolio Exercises Week 5api-479849199Nessuna valutazione finora
- Political and Institutional Challenges of ReforminDocumento28 paginePolitical and Institutional Challenges of ReforminferreiraccarolinaNessuna valutazione finora