Potrebbero piacerti anche
- Hydrocephalus, (Fluid in Brain) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHydrocephalus, (Fluid in Brain) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Sudden Cardiac Death: Ischaemic Heart DiseaseDocumento4 pagineSudden Cardiac Death: Ischaemic Heart Diseasenmyza89Nessuna valutazione finora
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Decrease All Properties of Cardiac Muscle: - H.R - C.O.P Essential For Normal Development of Nervous SystemDocumento1 paginaDecrease All Properties of Cardiac Muscle: - H.R - C.O.P Essential For Normal Development of Nervous Systemahmed K.Abd el SaterNessuna valutazione finora
- Pathophysiology 101-823: Unit 1 Basic Concepts of Health & DiseaseDocumento31 paginePathophysiology 101-823: Unit 1 Basic Concepts of Health & DiseaseReni PuspitasariNessuna valutazione finora
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- NCLEX SampleDocumento12 pagineNCLEX SampleYasser AhmedNessuna valutazione finora
- Sign and SymptomsDocumento8 pagineSign and SymptomsCaral Grace Gatdula-PenalbaNessuna valutazione finora
- Cardiovascular DiseasesDocumento8 pagineCardiovascular DiseasesRebecca MarshallNessuna valutazione finora
- Cardiovascular Dysfunction: (Patent Ductus Arteriosus)Documento6 pagineCardiovascular Dysfunction: (Patent Ductus Arteriosus)Jc MacujaNessuna valutazione finora
- Cheat Sheet For Fluid Balance and ElectrolytesDocumento2 pagineCheat Sheet For Fluid Balance and ElectrolytesLiel TorresNessuna valutazione finora
- Rheumatology OXF.: I. Immunology & InvestigationsDocumento12 pagineRheumatology OXF.: I. Immunology & InvestigationsFarah FarahNessuna valutazione finora
- Post-Strep Infxn Ddressler's Sydrome: Endocarditis Valvular Dse Pericarditis Cardiac TamponadeDocumento5 paginePost-Strep Infxn Ddressler's Sydrome: Endocarditis Valvular Dse Pericarditis Cardiac TamponadeEben Ezar Dela CruzNessuna valutazione finora
- SHOCK Slide WorkbookDocumento10 pagineSHOCK Slide WorkbookPATHMAPRIYA GANESANNessuna valutazione finora
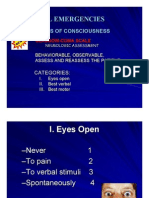
- Medical EmergenciesDocumento81 pagineMedical EmergenciesKreshnik HAJDARINessuna valutazione finora
- Endocarditis: (Post Strep Infection)Documento8 pagineEndocarditis: (Post Strep Infection)Eben Ezar Dela CruzNessuna valutazione finora
- Cerebrovascular AccidentDocumento79 pagineCerebrovascular AccidentKathy B. AbuanNessuna valutazione finora
- Adrenal Insufficiency and Addison's DiseaseDocumento8 pagineAdrenal Insufficiency and Addison's DiseaseyancefinceNessuna valutazione finora
- 1538 Exam 4 Cell Reg & GriefDocumento35 pagine1538 Exam 4 Cell Reg & GriefJade EdanoNessuna valutazione finora
- Electrolyte Cheat SheetDocumento1 paginaElectrolyte Cheat SheetChristinaNessuna valutazione finora
- Pericarditis Vs Mi: Internal Medicine: CvsDocumento6 paginePericarditis Vs Mi: Internal Medicine: CvsRojales FrancisNessuna valutazione finora
- Cerebrovascular Accident (Stroke)Documento15 pagineCerebrovascular Accident (Stroke)mesdejen100% (1)
- Heart BNHADocumento13 pagineHeart BNHAX OloGyNessuna valutazione finora
- Diagnosis of Acute Ischemic and Hemorrhagic StrokeDocumento22 pagineDiagnosis of Acute Ischemic and Hemorrhagic Strokeyulian100% (2)
- Cardio I: Shock, CHF, HTN, ACS Cheat Sheet: by ViaDocumento3 pagineCardio I: Shock, CHF, HTN, ACS Cheat Sheet: by ViaMariana NannettiNessuna valutazione finora
- Neuro CH 14 Study GuideDocumento9 pagineNeuro CH 14 Study GuideMichael J MillerNessuna valutazione finora
- PANCE Word Associations PDFDocumento27 paginePANCE Word Associations PDFkatNessuna valutazione finora
- Cerebellar DisordersDocumento12 pagineCerebellar DisordersAnn SamNessuna valutazione finora
- Common Presenting Signs and Symptoms PDFDocumento1 paginaCommon Presenting Signs and Symptoms PDFehidrobo1Nessuna valutazione finora
- Cardiovascular ADocumento3 pagineCardiovascular AAutumn AllisonNessuna valutazione finora
- 4.cardivascular System ExaminationDocumento60 pagine4.cardivascular System ExaminationElvisNessuna valutazione finora
- Neuro 3 Flashcards - QuizletDocumento24 pagineNeuro 3 Flashcards - QuizletAbdul Ghaffar AbdullahNessuna valutazione finora
- Head To Toe Checklist (Masroni)Documento13 pagineHead To Toe Checklist (Masroni)hillary elsaNessuna valutazione finora
- Peripheral Vascular (PVS) Examination OSCE Station GuideDocumento4 paginePeripheral Vascular (PVS) Examination OSCE Station GuideNikita JacobsNessuna valutazione finora
- Journal - Alzheimer DiseaseDocumento1 paginaJournal - Alzheimer DiseaseTriLightNessuna valutazione finora
- REVISED Head InjuryDocumento4 pagineREVISED Head InjuryJanselle H Arma0% (1)
- 1228 HFStroke Altered Neuro 2011Documento74 pagine1228 HFStroke Altered Neuro 2011Cyndy EnterlineNessuna valutazione finora
- Hypoxic Ischemic Encephalopathy (Hie) : AlgorithmDocumento11 pagineHypoxic Ischemic Encephalopathy (Hie) : AlgorithmAndreiMunteanuNessuna valutazione finora
- EATING DISORDERS: Note Taking OutlineDocumento6 pagineEATING DISORDERS: Note Taking OutlinePaula GarciaNessuna valutazione finora
- Spinal CordDocumento15 pagineSpinal Cordsimi y100% (1)
- Preventive CardiologyDocumento28 paginePreventive CardiologyerizonNessuna valutazione finora
- Clinical Lab Guide: by MedgeeksDocumento17 pagineClinical Lab Guide: by MedgeeksHuy HoangNessuna valutazione finora
- Head Injury 1Documento33 pagineHead Injury 1drvishal bhattNessuna valutazione finora
- Stroke FullDocumento10 pagineStroke Fullshowkat3Nessuna valutazione finora
- Anaphylaxis Diagnosis and ManagementDocumento10 pagineAnaphylaxis Diagnosis and Managementd dNessuna valutazione finora
- Source NotesDocumento30 pagineSource NotesChris Jardine Li100% (1)
- CardiomyopathyDocumento8 pagineCardiomyopathyKarisaNessuna valutazione finora
- Circulatory ShockDocumento4 pagineCirculatory ShockDasha VeeNessuna valutazione finora
- Cardiovascular DisordersDocumento9 pagineCardiovascular DisordersChristine Evan HoNessuna valutazione finora
- Acute Ischaemic StrokeDocumento40 pagineAcute Ischaemic StrokeDana Crusoveanu100% (1)
- Part 3 Huntingtons To EpilepsyDocumento10 paginePart 3 Huntingtons To EpilepsyNurse Ambassadors100% (1)
- Cerebrovascular Accident: TypesDocumento10 pagineCerebrovascular Accident: TypesJulia SalvioNessuna valutazione finora
- Common Histories and Red Flags Presentation Noninteractive VersionDocumento21 pagineCommon Histories and Red Flags Presentation Noninteractive VersionesmarNessuna valutazione finora
- Q: Describe The Diagnostic Criteria & Lab Investigation of SLE. AnsDocumento28 pagineQ: Describe The Diagnostic Criteria & Lab Investigation of SLE. AnsSajib Nakib100% (1)
- CardiologyDocumento7 pagineCardiologyMazhar WarisNessuna valutazione finora
- Pericarditis 65 SlidesDocumento65 paginePericarditis 65 SlidesAtifBhoreNessuna valutazione finora
- Cerebral Vascular Accident PresentationDocumento43 pagineCerebral Vascular Accident PresentationsgolbariNessuna valutazione finora
- Clinical Neurology Answers OnlyDocumento68 pagineClinical Neurology Answers Onlyanas kNessuna valutazione finora
- Cerebrovascular AccidentDocumento62 pagineCerebrovascular AccidentJaydee DalayNessuna valutazione finora
- 2012-European Journal of Neurology IMPRIMIR PAGINA 141Documento368 pagine2012-European Journal of Neurology IMPRIMIR PAGINA 141Francisco A. Villegas-LópezNessuna valutazione finora
- The Cisterna Magna SeptaDocumento13 pagineThe Cisterna Magna SeptaFrancisco A. Villegas-LópezNessuna valutazione finora
- Evaluaicon Del Dolor Por RMF Nejmoa1204471Documento10 pagineEvaluaicon Del Dolor Por RMF Nejmoa1204471Francisco A. Villegas-LópezNessuna valutazione finora
- A Parieto-Occipital Artery Arising From ICA Directly and Resultant Incomplete PCADocumento3 pagineA Parieto-Occipital Artery Arising From ICA Directly and Resultant Incomplete PCAFrancisco A. Villegas-LópezNessuna valutazione finora
- Bringing The Hospital To The Patient - First Treatment of Stroke Patients at The Emergency SiteDocumento5 pagineBringing The Hospital To The Patient - First Treatment of Stroke Patients at The Emergency SiteFrancisco A. Villegas-LópezNessuna valutazione finora
- StrokeDocumento8 pagineStrokeFrancisco A. Villegas-LópezNessuna valutazione finora
- Y de RouxDocumento5 pagineY de RouxFrancisco A. Villegas-LópezNessuna valutazione finora
- Retinal Diseases (Notes)Documento76 pagineRetinal Diseases (Notes)khloud ywsefNessuna valutazione finora
- Pinto 2013, BK and JC VirusDocumento7 paginePinto 2013, BK and JC VirusRodrigo GarciaNessuna valutazione finora
- The Endocrine System: Part ADocumento48 pagineThe Endocrine System: Part AYeuk NamNessuna valutazione finora
- Third Quarter Exam in Science 10Documento3 pagineThird Quarter Exam in Science 10Marife GuadalupeNessuna valutazione finora
- Pro-Fit - Internal Booklet (Print)Documento24 paginePro-Fit - Internal Booklet (Print)Meet GohilNessuna valutazione finora
- Neoplasms of The LungDocumento58 pagineNeoplasms of The LungLloyd Daniel BarrantesNessuna valutazione finora
- Assessment Explanation of The Problem Outcomes Interventions Rationale Evaluation STO: (Goal Met)Documento2 pagineAssessment Explanation of The Problem Outcomes Interventions Rationale Evaluation STO: (Goal Met)Arian May MarcosNessuna valutazione finora
- Medical Terminology List 350 TermsDocumento4 pagineMedical Terminology List 350 TermsSir SuneNessuna valutazione finora
- MG II - TEMA 4 Limba EnglezaDocumento3 pagineMG II - TEMA 4 Limba EnglezaGabriel IlinoiuNessuna valutazione finora
- Training in Microvascular Surgery UsingDocumento4 pagineTraining in Microvascular Surgery UsingBob sponjaNessuna valutazione finora
- Trigeminal Neuralgia in A Young Female Patient With V1 InvolementDocumento19 pagineTrigeminal Neuralgia in A Young Female Patient With V1 Involement6ixSideCreate MNessuna valutazione finora
- Benign and Malignant TumorsDocumento22 pagineBenign and Malignant TumorsmoupriyanagNessuna valutazione finora
- Cancer OropharynxDocumento108 pagineCancer OropharynxAshokNessuna valutazione finora
- Biopsycho QuestionsDocumento4 pagineBiopsycho QuestionsArianne PicanaNessuna valutazione finora
- Concept Strengthening Sheet (CSS-06) Based On CST-11 & 12 - Zoology-1Documento4 pagineConcept Strengthening Sheet (CSS-06) Based On CST-11 & 12 - Zoology-1Rudraksh AhujaNessuna valutazione finora
- Lesson Plan On OvaryDocumento4 pagineLesson Plan On OvaryJay PaulNessuna valutazione finora
- Ospe Du EntDocumento114 pagineOspe Du Entmfshihab3352Nessuna valutazione finora
- EX 9 Fetal Pig Dissection Answer KeyDocumento6 pagineEX 9 Fetal Pig Dissection Answer KeyThalia SandersNessuna valutazione finora
- Full Download Book Intraoperative Neuromonitoring PDFDocumento41 pagineFull Download Book Intraoperative Neuromonitoring PDFgeorge.crabtree472100% (17)
- Check Your English Vocabulary For MedicineDocumento57 pagineCheck Your English Vocabulary For MedicineМакс Колосов100% (1)
- Hormona de Crecimiento en NiñosDocumento15 pagineHormona de Crecimiento en NiñosEdinson Cabrera MenesesNessuna valutazione finora
- Ophthalmology MCQsDocumento532 pagineOphthalmology MCQsSaiSri LalamNessuna valutazione finora
- 4.the Vaginal Fluid Is Strongly Acid With PH 4.5 This Is Mainly Related ToDocumento16 pagine4.the Vaginal Fluid Is Strongly Acid With PH 4.5 This Is Mainly Related Tohasan ahmdNessuna valutazione finora
- Neuropsychology 2 BetDocumento11 pagineNeuropsychology 2 BetMike TemboNessuna valutazione finora
- Module Body Fluids For Board ExamDocumento8 pagineModule Body Fluids For Board ExamMichelle San Miguel FeguroNessuna valutazione finora
- Staff Nurse Exam Modal Question Paper PDF - 1 With AnswerDocumento9 pagineStaff Nurse Exam Modal Question Paper PDF - 1 With AnswerRoshita G Pillai0% (3)
- Memory Unit 10Documento41 pagineMemory Unit 10Rabia IsrafilNessuna valutazione finora
- Gladys Cheing RS3030 CNN Introduction To Neuroscience Note 2021Documento73 pagineGladys Cheing RS3030 CNN Introduction To Neuroscience Note 2021Tsang AmyNessuna valutazione finora
- Dissertation On Stem CellsDocumento8 pagineDissertation On Stem CellsCollegePaperWritingHelpCanada100% (1)
- Learning Module in NCM 114Documento28 pagineLearning Module in NCM 114JIMENEZ, TRISHA MARIE D.Nessuna valutazione finora
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (30)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (81)
- The Marshmallow Test: Mastering Self-ControlDa EverandThe Marshmallow Test: Mastering Self-ControlValutazione: 4.5 su 5 stelle4.5/5 (60)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 4 su 5 stelle4/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 4 su 5 stelle4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (170)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (253)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDa EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisValutazione: 3.5 su 5 stelle3.5/5 (2)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (45)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDa EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessValutazione: 4.5 su 5 stelle4.5/5 (328)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainDa EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainValutazione: 4 su 5 stelle4/5 (95)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDa EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesValutazione: 4.5 su 5 stelle4.5/5 (1412)