Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- ACE - Personal Trainer University Curriculum - Lab Manual PDFDocumento36 pagineACE - Personal Trainer University Curriculum - Lab Manual PDFdiego100% (1)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- LIFEWINDOW LW8 ManualDocumento65 pagineLIFEWINDOW LW8 ManualKihanNessuna valutazione finora
- Blood Pressure RegulationDocumento35 pagineBlood Pressure Regulationبراءة أحمد السلاماتNessuna valutazione finora
- COPD Patient Profile: 73-Year-Old Male TeacherDocumento14 pagineCOPD Patient Profile: 73-Year-Old Male Teacherprashanth100% (1)
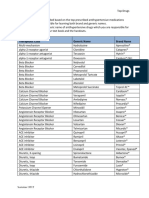
- Top Antihypertensive Drugs Generic-Brand Names PDFDocumento1 paginaTop Antihypertensive Drugs Generic-Brand Names PDFvidbala0% (1)
- Grade 8Documento8 pagineGrade 8Mohammad Zaid Sayaheen50% (2)
- Primary FRCA OSCE QuestionsDocumento10 paginePrimary FRCA OSCE QuestionsDsdNessuna valutazione finora
- General Appearance and Mental StatusDocumento4 pagineGeneral Appearance and Mental Statusmadamcloudnine100% (1)
- 2018-Journal of The American Geriatrics SocietyDocumento369 pagine2018-Journal of The American Geriatrics SocietyKevin PatrickNessuna valutazione finora
- Impact of 1-Hour Bundle Achievement in Septic Shock: Clinical MedicineDocumento8 pagineImpact of 1-Hour Bundle Achievement in Septic Shock: Clinical MedicineshishichanNessuna valutazione finora
- Tensiometro Cvs PharmacyDocumento38 pagineTensiometro Cvs PharmacyAlfredo PonsNessuna valutazione finora
- Blood Pressure Monitor: User ManualDocumento16 pagineBlood Pressure Monitor: User ManualAyush KumarNessuna valutazione finora
- TOP 5 Considerations for Anesthesia of a Geriatric PatientDocumento5 pagineTOP 5 Considerations for Anesthesia of a Geriatric PatientMabe AguirreNessuna valutazione finora
- Protap PenakibDocumento1 paginaProtap Penakibsiti marfu'atinNessuna valutazione finora
- Introduction To Clinical ExaminationDocumento153 pagineIntroduction To Clinical ExaminationBnB UsmleNessuna valutazione finora
- The Heart, Part 1 - Under Pressure: Crash Course A&P # 25Documento5 pagineThe Heart, Part 1 - Under Pressure: Crash Course A&P # 25Jordan TorresNessuna valutazione finora
- mcv00067845 - CC - Picco - Technology - Brochure - Us - 6 - Lo-Res-En-Us 2Documento32 paginemcv00067845 - CC - Picco - Technology - Brochure - Us - 6 - Lo-Res-En-Us 2Andrei ModreanuNessuna valutazione finora
- Prevalence and Awareness of Hypertension in NigeriaDocumento13 paginePrevalence and Awareness of Hypertension in NigeriaTaoreed AdegokeNessuna valutazione finora
- Multi-Parameter Vital Signs PM With Extendible Parameters: Monitor Directly Are StoredDocumento2 pagineMulti-Parameter Vital Signs PM With Extendible Parameters: Monitor Directly Are Storedcicik wijayantiNessuna valutazione finora
- Effect of Ultrafiltration Rate on Blood Pressure in Hemodialysis Patients: A Literature ReviewDocumento11 pagineEffect of Ultrafiltration Rate on Blood Pressure in Hemodialysis Patients: A Literature ReviewEka Septiani RinaiNessuna valutazione finora
- Preoperative Health Status Evaluation: An Accurate Medical HistoryDocumento18 paginePreoperative Health Status Evaluation: An Accurate Medical HistoryNisaNessuna valutazione finora
- Hyper TentionDocumento19 pagineHyper TentionAnthony MarkNessuna valutazione finora
- MCQs on cardiovascular disease, risk factors, and consequencesDocumento4 pagineMCQs on cardiovascular disease, risk factors, and consequencesZaina TNessuna valutazione finora
- GE Health Care - Individual Moduls Technical MaualDocumento622 pagineGE Health Care - Individual Moduls Technical MaualmaruthaiNessuna valutazione finora
- Essentials of Physiotherapy After Thoracic Surgery - What Physiotherapists Need To Know. A Narrative ReviewDocumento15 pagineEssentials of Physiotherapy After Thoracic Surgery - What Physiotherapists Need To Know. A Narrative ReviewMariana MadridNessuna valutazione finora
- Chaper 3: Probability and Probability Models: (Introductory Biostatistics - Chap T. Le)Documento7 pagineChaper 3: Probability and Probability Models: (Introductory Biostatistics - Chap T. Le)Hà Anh Minh LêNessuna valutazione finora
- Utility of Pulse Chapter in Murphy’s RepertoryDocumento2 pagineUtility of Pulse Chapter in Murphy’s RepertoryBABLU ROY100% (1)
- Acute Effects of Non-Nicotine Vaping On Vo2max, Blood Pressure, Heart Rate, and Lung VolumeDocumento23 pagineAcute Effects of Non-Nicotine Vaping On Vo2max, Blood Pressure, Heart Rate, and Lung VolumeKevin SNessuna valutazione finora
- Schiller Argus LCM - Service ManualDocumento144 pagineSchiller Argus LCM - Service ManualAbdel MundenNessuna valutazione finora
- Test For Two Relates SamplesDocumento48 pagineTest For Two Relates SamplesMiqz ZenNessuna valutazione finora