Potrebbero piacerti anche
- Carbohydrates InfoDocumento5 pagineCarbohydrates Infokaukau4everNessuna valutazione finora
- TANNINS CompleteDocumento61 pagineTANNINS Completekaukau4everNessuna valutazione finora
- Practical Exam PicsDocumento3 paginePractical Exam Picskaukau4everNessuna valutazione finora
- Glycosides For Practical PDFDocumento2 pagineGlycosides For Practical PDFkaukau4everNessuna valutazione finora
- Suha / Lukban: Citrus Grandis RutaceaeDocumento12 pagineSuha / Lukban: Citrus Grandis Rutaceaekaukau4everNessuna valutazione finora
- Volatile OilDocumento38 pagineVolatile Oilkaukau4everNessuna valutazione finora
- Tannins & LipidsDocumento46 pagineTannins & Lipidskaukau4ever100% (1)
- TanninsDocumento61 pagineTanninskaukau4everNessuna valutazione finora
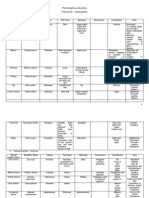
- Cac O Crystal of QuillajaDocumento22 pagineCac O Crystal of Quillajakaukau4everNessuna valutazione finora
- Resins (Practical Exam 8)Documento93 pagineResins (Practical Exam 8)kaukau4everNessuna valutazione finora
- Boards GlycosidesDocumento11 pagineBoards Glycosideskaukau4everNessuna valutazione finora
- Volatile OilDocumento38 pagineVolatile Oilkaukau4everNessuna valutazione finora
- Dosage Form Design Pharmaceutical and Formulation ConsiderationsDocumento103 pagineDosage Form Design Pharmaceutical and Formulation Considerationsprinceamit67% (3)
- AlkaloidsDocumento4 pagineAlkaloidskaukau4everNessuna valutazione finora
- Alkaloids SummaryDocumento1 paginaAlkaloids Summarykaukau4everNessuna valutazione finora
- Module 2 - Topic 1 - Protein Structure & Function Cont.Documento65 pagineModule 2 - Topic 1 - Protein Structure & Function Cont.kaukau4everNessuna valutazione finora
- Glycosides LecDocumento5 pagineGlycosides Leckaukau4everNessuna valutazione finora
- Module 1 - Topic 1 - The Chemistry of LifeDocumento142 pagineModule 1 - Topic 1 - The Chemistry of Lifekaukau4everNessuna valutazione finora
- Amino Acids TutorialDocumento9 pagineAmino Acids Tutorialkaukau4everNessuna valutazione finora
- AATableDocumento2 pagineAATablekaukau4everNessuna valutazione finora
- Amino AcidDocumento29 pagineAmino Acidmjzapant09Nessuna valutazione finora
- Dosage - Chapter 2 and Chapter 5Documento13 pagineDosage - Chapter 2 and Chapter 5Kim ManlangitNessuna valutazione finora
- Dosage - Chapter 13 (2d Half)Documento7 pagineDosage - Chapter 13 (2d Half)kaukau4everNessuna valutazione finora
- Dosage - Chapter 15Documento67 pagineDosage - Chapter 15Kim ManlangitNessuna valutazione finora
- Suppositories and InsertsDocumento5 pagineSuppositories and InsertsKim ManlangitNessuna valutazione finora
- Special Application SolutionsDocumento41 pagineSpecial Application SolutionsKim Manlangit100% (1)
- Dosage - Chapter 6Documento6 pagineDosage - Chapter 6kaukau4ever100% (3)
- Dosage - Chapter 14Documento57 pagineDosage - Chapter 14kaukau4ever100% (1)
- Dosage - Chapter 7Documento6 pagineDosage - Chapter 7kaukau4everNessuna valutazione finora
- Dosage - Chapter 9Documento5 pagineDosage - Chapter 9kaukau4everNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Quiz #1 Questions A&P 1Documento14 pagineQuiz #1 Questions A&P 1trick49Nessuna valutazione finora
- 2007, Vol.25, Issues 4, Cutaneous Receptors - Clinical Implications and Therapeutic RelevanceDocumento202 pagine2007, Vol.25, Issues 4, Cutaneous Receptors - Clinical Implications and Therapeutic RelevanceRizweta DestinNessuna valutazione finora
- Burn Case StudyDocumento76 pagineBurn Case StudyJoshua Agawin100% (1)
- Dermatology Revision E6.5 'Documento35 pagineDermatology Revision E6.5 'Riya SharmaNessuna valutazione finora
- Vdoc - Pub Clear Skin CookbookDocumento166 pagineVdoc - Pub Clear Skin CookbookAnca OanaNessuna valutazione finora
- 176 Anatomy Integumentary SystemDocumento29 pagine176 Anatomy Integumentary SystemJoana Mae PortezaNessuna valutazione finora
- The Integumentary System: Powerpoint Lecture Slides Prepared by Meg Flemming Austin Community CollegeDocumento62 pagineThe Integumentary System: Powerpoint Lecture Slides Prepared by Meg Flemming Austin Community CollegetanarNessuna valutazione finora
- Dermatopathology Diagnosis by First Impression 3rd Edition Ebook PDFDocumento57 pagineDermatopathology Diagnosis by First Impression 3rd Edition Ebook PDFmario.becker252100% (37)
- Campus Collusio N: Review Questions For Test PreparationDocumento3 pagineCampus Collusio N: Review Questions For Test PreparationGenna LedesmaNessuna valutazione finora
- His To Logical Changes in Radial Forearm Skin Flaps in The Oral Cavity - DR Darwish Badran - Medics Index MemberDocumento6 pagineHis To Logical Changes in Radial Forearm Skin Flaps in The Oral Cavity - DR Darwish Badran - Medics Index MemberMedicsindex Telepin Slidecase100% (1)
- Well Differentiated Squamous Cell Carcinoma, Keratoacanthoma Type. Three Cases. DR Sarma's DermpathDocumento17 pagineWell Differentiated Squamous Cell Carcinoma, Keratoacanthoma Type. Three Cases. DR Sarma's DermpathDeba P SarmaNessuna valutazione finora
- ANAPHY 1st ExamDocumento12 pagineANAPHY 1st ExamVine OrtegaNessuna valutazione finora
- Clinical, Dermoscopic and Histhopatological Findings in Diagnosis of Nevus SpilusDocumento7 pagineClinical, Dermoscopic and Histhopatological Findings in Diagnosis of Nevus SpilusYeni PuspitasariNessuna valutazione finora
- Diabetic Foot Ulcer Case StudyDocumento38 pagineDiabetic Foot Ulcer Case StudySanti Moore100% (1)
- Science6 q2 Mod1 Lesson1-2 Human Body System v1Documento32 pagineScience6 q2 Mod1 Lesson1-2 Human Body System v1HONEYLENE ORNOSNessuna valutazione finora
- Dermatologic Disorders PDFDocumento48 pagineDermatologic Disorders PDFWilda Hanim100% (1)
- Randyr Integumentary System WorksheetDocumento9 pagineRandyr Integumentary System WorksheetRandy ReynosoNessuna valutazione finora
- Geriatric DermatologyDocumento30 pagineGeriatric DermatologyMudsa Iing IletoNessuna valutazione finora
- Case Study Scarlet Fever Repaired)Documento34 pagineCase Study Scarlet Fever Repaired)Reimark RabanalNessuna valutazione finora
- SkinDocumento38 pagineSkinrodelagapito100% (1)
- eng - план разработка 7 2021Documento11 pagineeng - план разработка 7 2021НургулNessuna valutazione finora
- Microbiome and Skin Biology: ReviewDocumento6 pagineMicrobiome and Skin Biology: ReviewLinhNguyeNessuna valutazione finora
- The Integumentary System: Structure and FunctionsDocumento9 pagineThe Integumentary System: Structure and FunctionsJohn Paul ArcillaNessuna valutazione finora
- Unit VI Lecture NotesDocumento5 pagineUnit VI Lecture NotesSteve Sullivan100% (1)
- DR SARMA'S DERMPATH: Acantholytic Seborrheic Keratosis. The Internet Journal of Dermatology 2008: Volume 6 Number 2Documento4 pagineDR SARMA'S DERMPATH: Acantholytic Seborrheic Keratosis. The Internet Journal of Dermatology 2008: Volume 6 Number 2Deba P SarmaNessuna valutazione finora
- Caps HTMLDocumento152 pagineCaps HTMLUchy Luph'milimiLy0% (1)
- The Integumentary System: Skin, Hair, and NailsDocumento55 pagineThe Integumentary System: Skin, Hair, and NailsSandy CaliguiaNessuna valutazione finora
- RenovHyal Anti-Ageing Ingredient Reinforces Skin BarrierDocumento8 pagineRenovHyal Anti-Ageing Ingredient Reinforces Skin BarrierMaritaNetoNessuna valutazione finora
- Who Guidelines Hand Hygiene PDFDocumento170 pagineWho Guidelines Hand Hygiene PDFKomite PpiNessuna valutazione finora
- Activity 2B Integumentary System LOPEZ 1.0Documento3 pagineActivity 2B Integumentary System LOPEZ 1.0Ma. Joanna Catherine LopezNessuna valutazione finora