Potrebbero piacerti anche
- Energy Medicine Unlocked: A Comprehensive Guide to HealingDa EverandEnergy Medicine Unlocked: A Comprehensive Guide to HealingNessuna valutazione finora
- Polarity TherapyDocumento22 paginePolarity TherapyChris Walker100% (9)
- Entrainement and The Cranial Rythmic ImpulseDocumento7 pagineEntrainement and The Cranial Rythmic ImpulseDenise Mathre100% (1)
- Polarity - Stone's Polarity TherapyDocumento4 paginePolarity - Stone's Polarity Therapykabshiel67% (3)
- Polarityintro PDFDocumento18 paginePolarityintro PDFLaban Selvey BeyNessuna valutazione finora
- 58 Soft-Tissue Manipulation: Figure 2aDocumento4 pagine58 Soft-Tissue Manipulation: Figure 2ataichi7100% (1)
- Published Applied Kinesiology TextsDocumento10 paginePublished Applied Kinesiology TextsVíctor Muñoz López100% (1)
- DR StoneDocumento4 pagineDR StoneKostrun ZupiNessuna valutazione finora
- The Power of Physical Structure: Form and Function, With Kais FaddahDocumento36 pagineThe Power of Physical Structure: Form and Function, With Kais FaddahmoiNessuna valutazione finora
- Chapmans ReflexesDocumento10 pagineChapmans ReflexesNickosteo100% (9)
- Polarity Therapy ArticlesDocumento92 paginePolarity Therapy Articleskanaloa89% (18)
- Neurovascular Holding PointsDocumento8 pagineNeurovascular Holding PointsAlexandru Baciu100% (1)
- Advanced Kinesiology FinalDocumento97 pagineAdvanced Kinesiology FinalTnum100% (1)
- Chapmans Reflex 479Documento5 pagineChapmans Reflex 479Huram-abi0% (1)
- PDF - Scan ListsDocumento19 paginePDF - Scan ListsZoraida GutierrezNessuna valutazione finora
- Dental Equilibration and OsteopathyDocumento9 pagineDental Equilibration and OsteopathyshivnairNessuna valutazione finora
- Lossing DiagnosingTreatingDu PDFDocumento33 pagineLossing DiagnosingTreatingDu PDFDiana SchlittlerNessuna valutazione finora
- The Origins of Neural Organization TechniqueDocumento134 pagineThe Origins of Neural Organization TechniqueCarmen LlerenasNessuna valutazione finora
- Motifs: The Heart of Listening Volume One by Hugh MilneDocumento1 paginaMotifs: The Heart of Listening Volume One by Hugh MilneSimon FalconiNessuna valutazione finora
- Embryogenesis SheaDocumento4 pagineEmbryogenesis Sheaimageorge13100% (1)
- A Manual of Acupuncture - Applied Kinesiology IsraelDocumento0 pagineA Manual of Acupuncture - Applied Kinesiology Israelinej65100% (6)
- Hugo Tobar - Balancing With The 5 ElementsDocumento91 pagineHugo Tobar - Balancing With The 5 Elementsbjjman50% (2)
- Energetic Kinesiology24Documento1 paginaEnergetic Kinesiology24Marius Dan GiolgauNessuna valutazione finora
- The Bioenergetic Model in Osteopathic Diagnosis and Treatment: An FAAO Thesis, Part 1Documento9 pagineThe Bioenergetic Model in Osteopathic Diagnosis and Treatment: An FAAO Thesis, Part 1nish0420100% (1)
- Chapman's Reflexes Chapter (Edited 9.25.12) (Dragged) PDFDocumento1 paginaChapman's Reflexes Chapter (Edited 9.25.12) (Dragged) PDFobliquelyNessuna valutazione finora
- NK Course Guide enDocumento52 pagineNK Course Guide enIgnacioNessuna valutazione finora
- ETouch L1Documento42 pagineETouch L1vonipkoNessuna valutazione finora
- Working With Whiplash, Part II (Myofascial Techniques)Documento5 pagineWorking With Whiplash, Part II (Myofascial Techniques)Advanced-Trainings.com100% (2)
- Applied Kinesiology Collected PapersDocumento88 pagineApplied Kinesiology Collected PapersLopez Alejandro100% (1)
- Lossing BerylArbucklesCranial PDFDocumento67 pagineLossing BerylArbucklesCranial PDFdeemoney3100% (1)
- Craniosacral Therapy The Effects of Cranial Manipulation OnDocumento9 pagineCraniosacral Therapy The Effects of Cranial Manipulation Onaleman_gloria98420% (1)
- Cranial Intelligence: A Practical Guide To Biodynamic Craniosacral Therapy - Complementary MedicineDocumento4 pagineCranial Intelligence: A Practical Guide To Biodynamic Craniosacral Therapy - Complementary Medicinemulatabo0% (1)
- Chapman's Reflexes and Modern Clinical Applications - Lecture - William H. Devine, DODocumento94 pagineChapman's Reflexes and Modern Clinical Applications - Lecture - William H. Devine, DOHermann92% (12)
- Two Point BalanceDocumento33 pagineTwo Point BalanceMarkus van der Westhuizen100% (10)
- Applied Kinesiology FraudDocumento13 pagineApplied Kinesiology Fraudinfo7679Nessuna valutazione finora
- Tissue Provocation TherapiesDocumento7 pagineTissue Provocation TherapiesdracoscribdNessuna valutazione finora
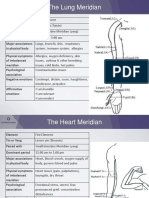
- The Body MeridiansDocumento61 pagineThe Body MeridiansAnonymous NKGMQv9100% (9)
- Health Kinesiology Reflex Point ChartsDocumento36 pagineHealth Kinesiology Reflex Point Chartssinhah100% (3)
- MeridiansDocumento12 pagineMeridianspundir100% (2)
- Pregnancy Polarity TherapyDocumento3 paginePregnancy Polarity TherapyJim FultonNessuna valutazione finora
- Vagus Nerve Deep DiveDocumento6 pagineVagus Nerve Deep DivebobNessuna valutazione finora
- Cranial Osteopathy Its Fate Seems ClearDocumento3 pagineCranial Osteopathy Its Fate Seems ClearInvincy JYNessuna valutazione finora
- Energetic Kinesiology25Documento1 paginaEnergetic Kinesiology25Marius Dan GiolgauNessuna valutazione finora
- The Clinical Applications of CranioSacral TherapyDocumento12 pagineThe Clinical Applications of CranioSacral Therapykabshiel100% (1)
- Acupuncture Shortcuts For Kinesiologists PDFDocumento2 pagineAcupuncture Shortcuts For Kinesiologists PDFCFYO Manuel Salgado FernándezNessuna valutazione finora
- Neurolymphatic Points Chapmans ReflexesDocumento15 pagineNeurolymphatic Points Chapmans Reflexestaichi7100% (14)
- L Kalichman PDFDocumento28 pagineL Kalichman PDFShahul HameedNessuna valutazione finora
- Kinesiology PDFDocumento3 pagineKinesiology PDFLeodoro LabragueNessuna valutazione finora
- What Is Potency - Exploring Phenomenon of Potency in Osteopathy in The Cranial Field - Helen Harrison - Research ProjectDocumento105 pagineWhat Is Potency - Exploring Phenomenon of Potency in Osteopathy in The Cranial Field - Helen Harrison - Research ProjectTito Alho100% (1)
- Chapman's Reflexes and Viscero-Somatic Refexes - William H. Devine, DO - Presentation 94 Slides PDFDocumento94 pagineChapman's Reflexes and Viscero-Somatic Refexes - William H. Devine, DO - Presentation 94 Slides PDFYuldash100% (2)
- Releasing Cranial/Dural Strains, Eliminating the Mystique: A Simple, Concise, New TechniqueDa EverandReleasing Cranial/Dural Strains, Eliminating the Mystique: A Simple, Concise, New TechniqueValutazione: 5 su 5 stelle5/5 (1)
- Holographic IssueDocumento44 pagineHolographic IssuemoiNessuna valutazione finora
- Touch For Health Casework02-Amy Choi Eng 2019Documento15 pagineTouch For Health Casework02-Amy Choi Eng 2019RukaphuongNessuna valutazione finora
- Muscle TestingDocumento4 pagineMuscle TestingDaniela Stranieri100% (7)
- Jim Jealous InterviewDocumento8 pagineJim Jealous InterviewFlorence Leo100% (1)
- What Is Neuro Emotional Technique?Documento4 pagineWhat Is Neuro Emotional Technique?Dr. Andrew Powell0% (2)
- Cranial Osteopathy For Babies and ChildrenDocumento2 pagineCranial Osteopathy For Babies and Childrenomddoc0% (1)
- Raphael Rettner - Advanced Healing Techniques For BodyworkersDocumento52 pagineRaphael Rettner - Advanced Healing Techniques For BodyworkersYuldash100% (1)
- 10 Acupuncture Shortcuts For KinesiologistsDocumento2 pagine10 Acupuncture Shortcuts For Kinesiologiststaichi7100% (10)
- Effectiveness of PTSD TreatmentsDocumento63 pagineEffectiveness of PTSD TreatmentsTariq J Faridi100% (1)
- Neurochemistry PPT in PDFDocumento52 pagineNeurochemistry PPT in PDFTariq J FaridiNessuna valutazione finora
- Lyones Combined Team FlyerDocumento13 pagineLyones Combined Team FlyerTariq J FaridiNessuna valutazione finora
- Healing Through Sound An Exploration of A Vocal Sound Healing Method in Great BritainDocumento254 pagineHealing Through Sound An Exploration of A Vocal Sound Healing Method in Great BritainTariq J Faridi100% (7)
- Call Us And: Order TodayDocumento14 pagineCall Us And: Order TodayTariq J FaridiNessuna valutazione finora
- Chronic Stress and Neural FunctionDocumento9 pagineChronic Stress and Neural FunctionTariq J FaridiNessuna valutazione finora
- Cervical Spine Decmpression Normal Shealy Paper in PainDocumento3 pagineCervical Spine Decmpression Normal Shealy Paper in PainTariq J FaridiNessuna valutazione finora
- Bio Mechanical Forces Promote Embryonic HaematopoiesisDocumento1 paginaBio Mechanical Forces Promote Embryonic HaematopoiesisTariq J FaridiNessuna valutazione finora
- Spinal Biomechanics ErgonomicsDocumento57 pagineSpinal Biomechanics ErgonomicsTariq J FaridiNessuna valutazione finora
- Music and Medicine The Affect of Music On The Human BeingDocumento10 pagineMusic and Medicine The Affect of Music On The Human BeingTariq J FaridiNessuna valutazione finora
- Principles of Physical Rehabilitation MedicineDocumento39 paginePrinciples of Physical Rehabilitation MedicineTariq J FaridiNessuna valutazione finora
- Accepted Manuscript: Behavioural Brain ResearchDocumento21 pagineAccepted Manuscript: Behavioural Brain ResearchPsiholog Monica StănescuNessuna valutazione finora
- The Place of Psychoanalytic Treatments Within Psychiatry: Glen O. Gabbard, MD John G. Gunderson, MD Peter Fonagy, PHDDocumento6 pagineThe Place of Psychoanalytic Treatments Within Psychiatry: Glen O. Gabbard, MD John G. Gunderson, MD Peter Fonagy, PHDapi-194035532Nessuna valutazione finora
- The Effects of Exercise Training in Adult Solid Organ Transplant Recipients A Systematic Review and Meta-AnalysisDocumento24 pagineThe Effects of Exercise Training in Adult Solid Organ Transplant Recipients A Systematic Review and Meta-AnalysisJesusNavarrete97Nessuna valutazione finora
- Psychodynamic Treatment For DepressionDocumento20 paginePsychodynamic Treatment For DepressionRenzo GonzalesNessuna valutazione finora
- Neuromuscular ExerciseDocumento10 pagineNeuromuscular ExerciseJuan Fran CoachNessuna valutazione finora
- 11 08 11 NewsletterDocumento33 pagine11 08 11 NewsletterifuckyoutitchNessuna valutazione finora
- Rao, Et Al, Anatomy of Failure PDFDocumento17 pagineRao, Et Al, Anatomy of Failure PDFJayaseelan RajNessuna valutazione finora
- Do We Still Need Formocresol in Pediatric DentistryDocumento3 pagineDo We Still Need Formocresol in Pediatric DentistryAlexanderDetorakisNessuna valutazione finora
- PR DR Coana - IntanArdylaMDocumento140 paginePR DR Coana - IntanArdylaMAnnisa Tria FadillaNessuna valutazione finora
- The Search For Disease-Modifying Agents in Decompensated Cirrhosis: From Drug Repurposing To Drug DiscoveryDocumento17 pagineThe Search For Disease-Modifying Agents in Decompensated Cirrhosis: From Drug Repurposing To Drug Discoverymuhamad deniansyahNessuna valutazione finora
- AphasiaDocumento28 pagineAphasiaEmilio Emmanué Escobar CruzNessuna valutazione finora
- AAOS Orthopaedic Knowledge Update 8Documento763 pagineAAOS Orthopaedic Knowledge Update 8Hiohi LianaNessuna valutazione finora
- Better Medicine, Better Treatment, Better Health (DR Purnamawati SP SpAK MMPaed)Documento69 pagineBetter Medicine, Better Treatment, Better Health (DR Purnamawati SP SpAK MMPaed)Ivan Danusaputra100% (1)
- Perineural Versus Intravenous Dexamethasone As An Adjuvant For Peripheral Nerve BlocksDocumento8 paginePerineural Versus Intravenous Dexamethasone As An Adjuvant For Peripheral Nerve Blockssome buddyyNessuna valutazione finora
- The Body As A Resource in PsychotherapyDocumento113 pagineThe Body As A Resource in PsychotherapyInglês The Right WayNessuna valutazione finora
- Occupational Therapy in Fatigue Management in MultDocumento8 pagineOccupational Therapy in Fatigue Management in MultghvntjbrbkNessuna valutazione finora
- A Systematic Review and Meta-A PDFDocumento17 pagineA Systematic Review and Meta-A PDFAprilia Aldila EnggardiniNessuna valutazione finora
- CD003709 PDFDocumento101 pagineCD003709 PDFMateoZuluagaGomezNessuna valutazione finora
- Types of Study DesignsDocumento53 pagineTypes of Study Designsselvakumar.anbalagan100% (8)
- Delta Frame Versus Blocking Wire in Management of Mallet Finger. Which Has Better Surgical Outcome A Systematic Review and Meta-AnalysisDocumento7 pagineDelta Frame Versus Blocking Wire in Management of Mallet Finger. Which Has Better Surgical Outcome A Systematic Review and Meta-AnalysisInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- 2018 - Early Intensive Behavioral Intervention (EIBI) For Young Children With Autism Spectrum Disorders (ASD)Documento65 pagine2018 - Early Intensive Behavioral Intervention (EIBI) For Young Children With Autism Spectrum Disorders (ASD)Raúl VerdugoNessuna valutazione finora
- Page 2012 RESEARCH DESIGNS IN SPORTS PHYSICAL THERAPY PDFDocumento11 paginePage 2012 RESEARCH DESIGNS IN SPORTS PHYSICAL THERAPY PDFValeRichardNessuna valutazione finora
- Ada 2018Documento174 pagineAda 2018CarlosChávezNessuna valutazione finora
- Diagnosis DVT Stage2Documento68 pagineDiagnosis DVT Stage2Naniek OkvitasariNessuna valutazione finora
- Title Perioperative Antibiotic Prophylaxis in Orthognathic SurgeryDocumento80 pagineTitle Perioperative Antibiotic Prophylaxis in Orthognathic SurgeryKuriyan ArimboorNessuna valutazione finora
- Master in Social Work (2019-2021) : Block Field Work Report Concurrent Field Work Topic: Vivid 19 VaccinationDocumento36 pagineMaster in Social Work (2019-2021) : Block Field Work Report Concurrent Field Work Topic: Vivid 19 Vaccination9415697349100% (1)
- Adverse Events Associated With Melatonin For The Treatment of Primary or Secondary Sleep Disorders: A Systematic ReviewDocumento20 pagineAdverse Events Associated With Melatonin For The Treatment of Primary or Secondary Sleep Disorders: A Systematic ReviewZach Segmuel MiñanoNessuna valutazione finora
- The Future of EU - HTADocumento16 pagineThe Future of EU - HTAMohamed HamilaNessuna valutazione finora
- Physical Therapy After Spinal Cord Injury: A Systematic Review of Treatments Focused On ParticipationDocumento10 paginePhysical Therapy After Spinal Cord Injury: A Systematic Review of Treatments Focused On ParticipationInaauliahanNessuna valutazione finora
- Facial PalsyDocumento7 pagineFacial PalsyPedro FonsecaNessuna valutazione finora