Potrebbero piacerti anche
- Guidelines Ovarian CancerDocumento78 pagineGuidelines Ovarian CancerCher'ieie'sa RifirandaNessuna valutazione finora
- Hyperemesis GravidarumDocumento7 pagineHyperemesis GravidarumPrawira Weka AkbariNessuna valutazione finora
- A Prediction Score For Safe and Successful Vaginal Birth After Cesarean Delivery A Prospective Controlled Study 2167 0420.1000129Documento7 pagineA Prediction Score For Safe and Successful Vaginal Birth After Cesarean Delivery A Prospective Controlled Study 2167 0420.1000129Cher'ieie'sa RifirandaNessuna valutazione finora
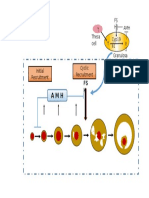
- T Cyp19 A1 T Theca Cell FS H AMHDocumento1 paginaT Cyp19 A1 T Theca Cell FS H AMHCher'ieie'sa RifirandaNessuna valutazione finora
- Role of Oocyte Morphology On Fertilization and Embryo Formation in Assisted Reproductive Techniques.Documento6 pagineRole of Oocyte Morphology On Fertilization and Embryo Formation in Assisted Reproductive Techniques.Cher'ieie'sa RifirandaNessuna valutazione finora
- Syndrome of Newborn: Versus: THE Respiratory Distress THE Immaturity PrematurityDocumento5 pagineSyndrome of Newborn: Versus: THE Respiratory Distress THE Immaturity PrematurityCher'ieie'sa RifirandaNessuna valutazione finora
- 19 Pengukuran Dalam PenelitianDocumento7 pagine19 Pengukuran Dalam PenelitianCher'ieie'sa RifirandaNessuna valutazione finora
- Multiple-Choice Questions: Paper 2: A B C D eDocumento35 pagineMultiple-Choice Questions: Paper 2: A B C D eCher'ieie'sa RifirandaNessuna valutazione finora
- Performance of First Trimester Fetal Ultrasound ScanDocumento12 paginePerformance of First Trimester Fetal Ultrasound ScanPujianti LestarinaNessuna valutazione finora
- Rymer CHPT 01-29a40fc0rdzDocumento29 pagineRymer CHPT 01-29a40fc0rdzCher'ieie'sa RifirandaNessuna valutazione finora
- An Care Tutor 20 DecDocumento75 pagineAn Care Tutor 20 DecCher'ieie'sa RifirandaNessuna valutazione finora
- Foot UlcersDocumento29 pagineFoot UlcersCher'ieie'sa RifirandaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Xyngular Ingredient BenefitsDocumento18 pagineXyngular Ingredient BenefitsAnthony RodriguezNessuna valutazione finora
- Mimickers of UrticariaDocumento9 pagineMimickers of UrticariaNaeNessuna valutazione finora
- NHS Highland Wound Management Guidelines and Formulary PDFDocumento91 pagineNHS Highland Wound Management Guidelines and Formulary PDFubayyumr100% (1)
- Unit-1 Intro To ImmunologyDocumento49 pagineUnit-1 Intro To ImmunologyRituNessuna valutazione finora
- PsiconeuroinmunologíaDocumento10 paginePsiconeuroinmunologíaLuis Alfredo Rosales GuerreroNessuna valutazione finora
- AutoimmuneSolution FINAL PDFDocumento24 pagineAutoimmuneSolution FINAL PDFMihaela Gradinaru100% (6)
- Homeopathy Philosophy and Proving ExplainedDocumento43 pagineHomeopathy Philosophy and Proving ExplainedVijay Agrawal100% (2)
- Consensus Document Surgical Wound Dehiscence Improving Prevention and OutcomesDocumento48 pagineConsensus Document Surgical Wound Dehiscence Improving Prevention and OutcomesJeffri syaputraNessuna valutazione finora
- REFERAT - ToxicologieDocumento21 pagineREFERAT - ToxicologieCotovici Catana AlinaNessuna valutazione finora
- Johnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-241-260Documento20 pagineJohnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-241-260toanbau100% (1)
- 881 2026 1 PBDocumento12 pagine881 2026 1 PBwanferol -Nessuna valutazione finora
- Curing Back Pain NaturallyDocumento37 pagineCuring Back Pain Naturallyyashvirsingh2150% (2)
- Test Bank For Understanding Pathophysiology 7th Edition Sue Huether Kathryn MccanceDocumento12 pagineTest Bank For Understanding Pathophysiology 7th Edition Sue Huether Kathryn Mccancekimberlymatthewsddsqocjewyibg90% (10)
- GangreneDocumento18 pagineGangreneFelita Surya RiniNessuna valutazione finora
- Golden Milk Turmeric LatteDocumento4 pagineGolden Milk Turmeric LatteHelena AzevedoNessuna valutazione finora
- CABALIDA - Herbal PlantsDocumento29 pagineCABALIDA - Herbal PlantsJeralyn CABALIDANessuna valutazione finora
- Paediatrica IndonesianaDocumento6 paginePaediatrica IndonesianayusrinastitiNessuna valutazione finora
- Ann Clin Transl Neurol - 2021 - Horino - Intrathecal Dexamethasone Therapy For Febrile Infection Related Epilepsy SyndromeDocumento11 pagineAnn Clin Transl Neurol - 2021 - Horino - Intrathecal Dexamethasone Therapy For Febrile Infection Related Epilepsy SyndromePt.Natasha AriviaNessuna valutazione finora
- Presentation Metabolic SyndromeDocumento56 paginePresentation Metabolic SyndromeAbdulhakeem Tleimat100% (1)
- Double Cleanse Case StudyDocumento8 pagineDouble Cleanse Case StudyVivi VivianaNessuna valutazione finora
- Manual Therapy: Annina B. Schmid, Robert J. Nee, Michel W. CoppietersDocumento9 pagineManual Therapy: Annina B. Schmid, Robert J. Nee, Michel W. CoppietersJose PerezNessuna valutazione finora
- BSC Diylasis SinghaniaDocumento20 pagineBSC Diylasis Singhaniaom vermaNessuna valutazione finora
- PeritonitisDocumento6 paginePeritonitisDiane ArgoteNessuna valutazione finora
- Toward Nanotechnology-Enabled Approaches Against The COVID-19 PandemicDocumento24 pagineToward Nanotechnology-Enabled Approaches Against The COVID-19 Pandemicmadcraft9832Nessuna valutazione finora
- Fish Nutrition and Current Issues in Aquaculture The Balance in Providing Safe and Nutritious Seafood in An Environmentally Sustainable Manner 2155 9546.1000234Documento10 pagineFish Nutrition and Current Issues in Aquaculture The Balance in Providing Safe and Nutritious Seafood in An Environmentally Sustainable Manner 2155 9546.1000234Maarij SaleemNessuna valutazione finora
- Dietary Intervention in AcneDocumento13 pagineDietary Intervention in AcnePhelipe Auerswald Do AmaralNessuna valutazione finora
- Rheumatic Heart Disease Types and CausesDocumento3 pagineRheumatic Heart Disease Types and CausesWay LeeNessuna valutazione finora
- Essay ImmuneDocumento8 pagineEssay ImmuneAishah Najihah100% (1)
- Immuno Sero Lec Prelim TransDocumento15 pagineImmuno Sero Lec Prelim TransLoren EscotoNessuna valutazione finora
- Bee Pollen Chemical Composition and Therapeutic ApplicationDocumento6 pagineBee Pollen Chemical Composition and Therapeutic ApplicationZeynep Emirhan ŞenyüzNessuna valutazione finora