Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- The Smart Parking Management SystemDocumento12 pagineThe Smart Parking Management Systemsimo mjidiNessuna valutazione finora
- From Clicks To Security: Investigating Continuous Authentication Via Mouse DynamicsDocumento16 pagineFrom Clicks To Security: Investigating Continuous Authentication Via Mouse DynamicsAnonymous Gl4IRRjzNNessuna valutazione finora
- A Comparative Study of Text Comprehension in IELTS Reading Exam Using GPT-3Documento8 pagineA Comparative Study of Text Comprehension in IELTS Reading Exam Using GPT-3Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Papers - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Papers - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Papers - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Papers - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Variations in Outcome For The Same Map Reduce Transitive Closure Algorithm Implemented On Different Hadoop PlatformsDocumento8 pagineVariations in Outcome For The Same Map Reduce Transitive Closure Algorithm Implemented On Different Hadoop PlatformsAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- XML Encryption and Signature For Securing Web ServicesDocumento14 pagineXML Encryption and Signature For Securing Web ServicesAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Machine Learning in Early Genetic Detection of Multiple Sclerosis Disease: A SurveyDocumento18 pagineMachine Learning in Early Genetic Detection of Multiple Sclerosis Disease: A SurveyAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- IoT Security: Penetration Testing of White-Label Cloud-Based IoT Camera Compromising Personal Data PrivacyDocumento12 pagineIoT Security: Penetration Testing of White-Label Cloud-Based IoT Camera Compromising Personal Data PrivacyAnonymous Gl4IRRjzNNessuna valutazione finora
- Comparison of Rendering Processes On 3D ModelDocumento10 pagineComparison of Rendering Processes On 3D ModelAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Determining Business Intelligence Usage SuccessDocumento23 pagineDetermining Business Intelligence Usage SuccessAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- A New Approach For Ranking Shadowed Fuzzy Numbers and Its ApplicationDocumento16 pagineA New Approach For Ranking Shadowed Fuzzy Numbers and Its ApplicationAnonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Call For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Documento2 pagineCall For Articles - International Journal of Computer Science & Information Technology (IJCSIT)Anonymous Gl4IRRjzNNessuna valutazione finora
- Secure Arcade: A Gamified Defense Against Cyber AttacksDocumento17 pagineSecure Arcade: A Gamified Defense Against Cyber AttacksAnonymous Gl4IRRjzNNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- BSBPMG531 - Assessment Task 3 v2Documento19 pagineBSBPMG531 - Assessment Task 3 v2Felipe ParadaNessuna valutazione finora
- Android User GuideDocumento15 pagineAndroid User GuideAnonymous 1Wb6JCkNessuna valutazione finora
- Company in India" DTDC Constantly Endeavours To Meet & Exceed Customers'Documento7 pagineCompany in India" DTDC Constantly Endeavours To Meet & Exceed Customers'Vinod KumarNessuna valutazione finora
- 2020.04.24 BC thamtratonghop TKCS Trường Fulbright Lần 1Documento32 pagine2020.04.24 BC thamtratonghop TKCS Trường Fulbright Lần 1Khac Hoang PhamNessuna valutazione finora
- Detailed Lesson Log in MathematicsDocumento7 pagineDetailed Lesson Log in MathematicsChan Chan100% (1)
- QAch 02Documento13 pagineQAch 02Rami Alnajjar100% (1)
- Growth of Escherichia Coli in A 5 Litre Batch Fermentation VesselDocumento15 pagineGrowth of Escherichia Coli in A 5 Litre Batch Fermentation VesselAs'ad Mughal100% (2)
- 1082-Adding New Replication From Sybase To OracleDocumento4 pagine1082-Adding New Replication From Sybase To Oraclegirish10670Nessuna valutazione finora
- Ingrid Olderock La Mujer de Los Perros by Nancy GuzmnDocumento14 pagineIngrid Olderock La Mujer de Los Perros by Nancy GuzmnYuki Hotaru0% (3)
- Specification For Foamed Concrete: by K C Brady, G R A Watts and Ivi R JonesDocumento20 pagineSpecification For Foamed Concrete: by K C Brady, G R A Watts and Ivi R JonesMaria Aiza Maniwang Calumba100% (1)
- StetindDocumento6 pagineStetindGiovanniNessuna valutazione finora
- L1 Differential AmplifiersDocumento21 pagineL1 Differential AmplifiersTemesgen ZelekeNessuna valutazione finora
- NTS - Math Notes & Mcqs Solved Grade 8thDocumento10 pagineNTS - Math Notes & Mcqs Solved Grade 8thZahid KumailNessuna valutazione finora
- QCDD-Duyar-QR SprinklersDocumento2 pagineQCDD-Duyar-QR SprinklersBaraa' KahlawiNessuna valutazione finora
- Tool PresettingDocumento22 pagineTool PresettingAtulMaurya100% (1)
- UbnfilelDocumento3 pagineUbnfilelJorge LorenzoNessuna valutazione finora
- HartfordDocumento7 pagineHartfordapi-443631703Nessuna valutazione finora
- Feedwater Heating SystemsDocumento82 pagineFeedwater Heating SystemsJitendra ChaudhariNessuna valutazione finora
- 4 10 59 08 Juni 2023Documento5 pagine4 10 59 08 Juni 2023ihor.vezhninNessuna valutazione finora
- LS-VINA EHV Cable's CatalogueDocumento36 pagineLS-VINA EHV Cable's CatalogueDjar Ndoeth0% (1)
- IOT SyllabusDocumento3 pagineIOT Syllabuspoojan thakkarNessuna valutazione finora
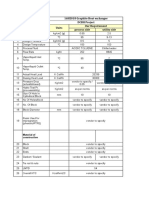
- 16HE018 Graphite Heat Exchanger DCBH Project Sr. No. Particulars Units Our Requirement Process Side Utility SideDocumento2 pagine16HE018 Graphite Heat Exchanger DCBH Project Sr. No. Particulars Units Our Requirement Process Side Utility SideBhaumik BhuvaNessuna valutazione finora
- Surface Finish StandardDocumento3 pagineSurface Finish StandardvinodmysoreNessuna valutazione finora
- Swiss FCM Ordinance - EuPIA QDocumento6 pagineSwiss FCM Ordinance - EuPIA Qiz_nazNessuna valutazione finora
- Checklists 4yrDocumento2 pagineChecklists 4yrKarla TreviñoNessuna valutazione finora
- 2SK3377Documento5 pagine2SK3377Jheremy Sebastian TorresNessuna valutazione finora
- Drainage CapacityDocumento33 pagineDrainage Capacityfan_luc89Nessuna valutazione finora
- ETG3000 BrochureDocumento9 pagineETG3000 BrochureMayolo MartinezNessuna valutazione finora
- Appendix 1: Lesson Plan (Template)Documento4 pagineAppendix 1: Lesson Plan (Template)Anonymous X7u8sMNessuna valutazione finora
- Supervisory Setpoint Control (SSC) : I/A Series SystemDocumento46 pagineSupervisory Setpoint Control (SSC) : I/A Series SystemMiguel Angel GiménezNessuna valutazione finora