Potrebbero piacerti anche
- Visual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsDa EverandVisual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsNessuna valutazione finora
- Approach To The Adult With Acute Persistent Visual LossDocumento17 pagineApproach To The Adult With Acute Persistent Visual LossMauricio SvNessuna valutazione finora
- Passmedicine MRCP Notes-OphthalmologyDocumento31 paginePassmedicine MRCP Notes-OphthalmologyHashim Ahmad50% (2)
- Activity7 (Sympathetic Ophthalmia)Documento4 pagineActivity7 (Sympathetic Ophthalmia)Gabbii CincoNessuna valutazione finora
- 16.cataract - MBBS ClassDocumento44 pagine16.cataract - MBBS ClassManish ShresthaNessuna valutazione finora
- Ophthalmology NotesDocumento81 pagineOphthalmology Notesmr_david50% (2)
- Ahmed 2010Documento11 pagineAhmed 2010Karamjot SinghNessuna valutazione finora
- Optic Neuritis: Demyelinating Disorders: Multiple Sclerosis (MS)Documento4 pagineOptic Neuritis: Demyelinating Disorders: Multiple Sclerosis (MS)Najibah YaNessuna valutazione finora
- OphthalDocumento17 pagineOphthalSanketNandaniNessuna valutazione finora
- Urgencias OftalmológicasDocumento20 pagineUrgencias OftalmológicasDaniela León CastilloNessuna valutazione finora
- Neuro-Ophta EditedDocumento97 pagineNeuro-Ophta EditedMarshet GeteNessuna valutazione finora
- Activity4 (Retinal-Disorders)Documento6 pagineActivity4 (Retinal-Disorders)Gabbii CincoNessuna valutazione finora
- Case 1: 70-Yr Man Complains of Sudden and Total Loss Vision in One Eye. No Pain or Other SymptomsDocumento17 pagineCase 1: 70-Yr Man Complains of Sudden and Total Loss Vision in One Eye. No Pain or Other SymptomsCherry TamNessuna valutazione finora
- Trauma & Benda Asing Pada MataDocumento14 pagineTrauma & Benda Asing Pada MataTeguh Imana NugrahaNessuna valutazione finora
- Additional Slide: Lapsus Lensa 1Documento58 pagineAdditional Slide: Lapsus Lensa 1Bram UtamaNessuna valutazione finora
- Vision Loss PreventionDocumento22 pagineVision Loss Preventionmadara ëNessuna valutazione finora
- Acute Visual LossDocumento10 pagineAcute Visual LossJim Jose AntonyNessuna valutazione finora
- UWorld Notes NeurologyDocumento6 pagineUWorld Notes NeurologysarahNessuna valutazione finora
- Ophthalmology NotesDocumento82 pagineOphthalmology NotesDr-Fadi AlkayyaliNessuna valutazione finora
- Ocular TraumaDocumento50 pagineOcular TraumafatimaNessuna valutazione finora
- Disorders of Optic Nerve and Visual Pathways: Ipek MidiDocumento24 pagineDisorders of Optic Nerve and Visual Pathways: Ipek MidiEcaterina ChiriacNessuna valutazione finora
- Posterior SegmentDocumento102 paginePosterior SegmentAlice ChirilaNessuna valutazione finora
- PEAC OphthalmologyDocumento45 paginePEAC OphthalmologySdNessuna valutazione finora
- GlaucomeaDocumento21 pagineGlaucomeamalathiNessuna valutazione finora
- Eye and Ear Disorders UpdatedDocumento78 pagineEye and Ear Disorders Updatedjose arreolaNessuna valutazione finora
- Flashes and Floaters: Ahmed Shahab M08082Documento15 pagineFlashes and Floaters: Ahmed Shahab M08082Ahmed ShahabNessuna valutazione finora
- Diseases of The Optic Nerve 09Documento25 pagineDiseases of The Optic Nerve 09somebody_maNessuna valutazione finora
- Buta Mendadak / Acute Vision Loss: Dr. R. Handoko Pratomo, SPMDocumento33 pagineButa Mendadak / Acute Vision Loss: Dr. R. Handoko Pratomo, SPMSesria NasutionNessuna valutazione finora
- GlaucomaDocumento34 pagineGlaucomabobamaryNessuna valutazione finora
- Optic AtrophyDocumento6 pagineOptic Atrophyrutuparna383Nessuna valutazione finora
- Ophthalmology For 5th Year Exams: Visual AcuityDocumento7 pagineOphthalmology For 5th Year Exams: Visual AcuitySaloni PatelNessuna valutazione finora
- Bagheri 2015Documento15 pagineBagheri 2015Juliana Valentina CedeñoNessuna valutazione finora
- Retinal DetachmentDocumento10 pagineRetinal DetachmentSilpi HamidiyahNessuna valutazione finora
- Eye & ENTDocumento12 pagineEye & ENTShandar SadafNessuna valutazione finora
- Angle-Closure Glaucoma - UpToDateDocumento9 pagineAngle-Closure Glaucoma - UpToDateElaine June FielNessuna valutazione finora
- OPHTHA - Histiry and PEDocumento6 pagineOPHTHA - Histiry and PEMarianne R. LorenzoNessuna valutazione finora
- Neuro-Ophthalmology: Simon J HickmanDocumento10 pagineNeuro-Ophthalmology: Simon J Hickmanhalvi89Nessuna valutazione finora
- Ocular EmergDocumento41 pagineOcular EmergMohd SyazrinNessuna valutazione finora
- K.15 Ophtalmologic EmergenciesDocumento35 pagineK.15 Ophtalmologic EmergenciesZikri Putra Lan Lubis100% (1)
- Grodno State Medical University: Assistant Lecturer of The Department of OphthalmologyDocumento24 pagineGrodno State Medical University: Assistant Lecturer of The Department of OphthalmologyTeguh Imana NugrahaNessuna valutazione finora
- Approach To The Patient With Visual Hallucinations - UpToDateDocumento13 pagineApproach To The Patient With Visual Hallucinations - UpToDateImja94Nessuna valutazione finora
- Care of Clients With Sensory Problems Care of Clients With Sensory ProblemsDocumento82 pagineCare of Clients With Sensory Problems Care of Clients With Sensory Problemssnpjavier100% (1)
- Chapter 11 Eye & Vision DisordersDocumento72 pagineChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSANessuna valutazione finora
- Ophthalmology Emergencies - 2Documento32 pagineOphthalmology Emergencies - 2navenNessuna valutazione finora
- Presentation On Loss of VisionDocumento127 paginePresentation On Loss of VisionJunayed MahmudNessuna valutazione finora
- Uveitis PDFDocumento17 pagineUveitis PDFkmiz85Nessuna valutazione finora
- 2019 Dr. Halida 1. Retinopati DiabetikafixDocumento44 pagine2019 Dr. Halida 1. Retinopati DiabetikafixLuthfia WardhaniNessuna valutazione finora
- JurnalDocumento13 pagineJurnaldennisadityaNessuna valutazione finora
- Fundoscopy: Learning OutcomesDocumento6 pagineFundoscopy: Learning OutcomesSaraNessuna valutazione finora
- Assessment of EyeDocumento15 pagineAssessment of EyegemergencycareNessuna valutazione finora
- Protrusion OjoDocumento16 pagineProtrusion OjoAntonio ReaNessuna valutazione finora
- Sudden Loss of Vision & Optic NeuropathyDocumento30 pagineSudden Loss of Vision & Optic NeuropathyIshak IzharNessuna valutazione finora
- Activity2 (Glaucoma)Documento7 pagineActivity2 (Glaucoma)Gabbii CincoNessuna valutazione finora
- Ocular Emergencies: AssessmentDocumento7 pagineOcular Emergencies: AssessmentradhikasreedharNessuna valutazione finora
- Ocular EmergenciesDocumento26 pagineOcular EmergenciesYukianesa100% (1)
- Diplopia - Eye Disorders - MSD Manual Professional EditionDocumento5 pagineDiplopia - Eye Disorders - MSD Manual Professional EditionApostolos T.Nessuna valutazione finora
- Search Uptodate: Grade 1CDocumento1 paginaSearch Uptodate: Grade 1CGabriella TjondroNessuna valutazione finora
- Normal Eye With Sudden Decreased VisionDocumento38 pagineNormal Eye With Sudden Decreased VisionAnjar NuryantoNessuna valutazione finora
- Morphological and Topographical Appearance of Microaneurysms On Optical Coherence Tomography AngiographyDocumento6 pagineMorphological and Topographical Appearance of Microaneurysms On Optical Coherence Tomography AngiographyConnie STNessuna valutazione finora
- Review of Ophthalmology Supplemental Questions - Friedman - 2005Documento134 pagineReview of Ophthalmology Supplemental Questions - Friedman - 2005Radu Smaranda100% (1)
- Good Practice in OrthokeratologyDocumento12 pagineGood Practice in OrthokeratologyPhilip McNelsonNessuna valutazione finora
- Pemeriksaan Refraksi Sikloplegik Pada AnakDocumento38 paginePemeriksaan Refraksi Sikloplegik Pada AnakTia AfelitaNessuna valutazione finora
- Biology Investigatory Project On Eye DiseasesDocumento18 pagineBiology Investigatory Project On Eye DiseasesBHALAJI KARUNANITHI100% (1)
- Optha Samplex and Recalls All inDocumento51 pagineOptha Samplex and Recalls All inDey SibalNessuna valutazione finora
- Wavefront Customized Visual Correction - The Quest For Super Vision II (PDFDrive)Documento413 pagineWavefront Customized Visual Correction - The Quest For Super Vision II (PDFDrive)sandiNessuna valutazione finora
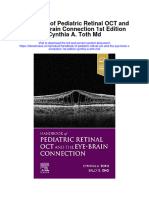
- Handbook of Pediatric Retinal Oct and The Eye Brain Connection 1St Edition Cynthia A Toth MD Full ChapterDocumento67 pagineHandbook of Pediatric Retinal Oct and The Eye Brain Connection 1St Edition Cynthia A Toth MD Full Chapterpaul.grissom854100% (4)
- Vision Screening - Dr. WagnerDocumento37 pagineVision Screening - Dr. WagnerDien Doan QuangNessuna valutazione finora
- Rameshwar PatidarDocumento22 pagineRameshwar PatidarnkhljainNessuna valutazione finora
- Endophthalmitis 1Documento42 pagineEndophthalmitis 1Nasrin sultana rmcNessuna valutazione finora
- Ocular Foreign Bodies A Review 2155 9570 1000645 1Documento5 pagineOcular Foreign Bodies A Review 2155 9570 1000645 1memey100% (1)
- Vision Therapy Information KitDocumento14 pagineVision Therapy Information Kitmoniquitta2000Nessuna valutazione finora
- Crizal Prevencia - AV ChartDocumento10 pagineCrizal Prevencia - AV ChartfazzlieNessuna valutazione finora
- Medical Devices-Physio Eye PresentationDocumento37 pagineMedical Devices-Physio Eye PresentationPharmacy Admission ExpertNessuna valutazione finora
- Zenni Optical PD Ruler PDFDocumento1 paginaZenni Optical PD Ruler PDFkameliasitorusNessuna valutazione finora
- Exotropiain AdultsDocumento3 pagineExotropiain AdultsTlati AmineNessuna valutazione finora
- Prevalence and Prognosis of Corneal Perforation Patient in Beijing ChinaDocumento4 paginePrevalence and Prognosis of Corneal Perforation Patient in Beijing Chinaalifah syarafinaNessuna valutazione finora
- SIM For Grade 3Documento21 pagineSIM For Grade 3Mark Cua96% (154)
- Cataract NotesDocumento4 pagineCataract NotesJeremy LauNessuna valutazione finora
- Macular Function TestDocumento2 pagineMacular Function TestNeha SinghNessuna valutazione finora
- Ophthalmology InstrumentsDocumento38 pagineOphthalmology InstrumentsDevansh SinghNessuna valutazione finora
- 07 Crossed Eyes Nystagmus and AmblyopiaDocumento7 pagine07 Crossed Eyes Nystagmus and AmblyopiaMwanja MosesNessuna valutazione finora
- Module Opthalmology Corneal Ulcer: Group 7 Wulan-Fadzely-Arif Amri-Safuan Arif-Nadiah-Insyira-Fatimah-Andi AbsharinaDocumento19 pagineModule Opthalmology Corneal Ulcer: Group 7 Wulan-Fadzely-Arif Amri-Safuan Arif-Nadiah-Insyira-Fatimah-Andi Absharinaarifamri92Nessuna valutazione finora
- Risk Factor Analysis FOR Long-Term Unfavorable Ocular Outcomes in Children Treated FOR RETINOPATHY OF PREMATURITYDocumento7 pagineRisk Factor Analysis FOR Long-Term Unfavorable Ocular Outcomes in Children Treated FOR RETINOPATHY OF PREMATURITYSalma HamdyNessuna valutazione finora
- Patients' Attitudes and Beliefs To Presbyopia and Its CorrectionDocumento6 paginePatients' Attitudes and Beliefs To Presbyopia and Its CorrectionPutri kartiniNessuna valutazione finora
- Ophthalmology Osce Exam - PPTX PP by Abel - 230170110143Documento86 pagineOphthalmology Osce Exam - PPTX PP by Abel - 230170110143Chefera Aga100% (1)
- Summary OphthalmologyDocumento86 pagineSummary Ophthalmologymarina_shawkyNessuna valutazione finora
- Kyoto Kagaku - Eye Examination SimulatorDocumento2 pagineKyoto Kagaku - Eye Examination SimulatorGabriela Zavaleta Camacho100% (1)
- Daftar PustakaDocumento4 pagineDaftar PustakaHariz Ghulam RNessuna valutazione finora
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndDa EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndNessuna valutazione finora
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (1)
- The Bridesmaid: The addictive psychological thriller that everyone is talking aboutDa EverandThe Bridesmaid: The addictive psychological thriller that everyone is talking aboutValutazione: 4 su 5 stelle4/5 (131)
- Breaking the Habit of Being YourselfDa EverandBreaking the Habit of Being YourselfValutazione: 4.5 su 5 stelle4.5/5 (1458)
- Gut: the new and revised Sunday Times bestsellerDa EverandGut: the new and revised Sunday Times bestsellerValutazione: 4 su 5 stelle4/5 (392)
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerDa EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerValutazione: 4.5 su 5 stelle4.5/5 (58)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissDa EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissValutazione: 4.5 su 5 stelle4.5/5 (81)
- Prisoners of Geography: Ten Maps That Explain Everything About the WorldDa EverandPrisoners of Geography: Ten Maps That Explain Everything About the WorldValutazione: 4.5 su 5 stelle4.5/5 (1145)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipDa EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipValutazione: 4.5 su 5 stelle4.5/5 (1135)
- Neville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!Da EverandNeville Goddard Master Course to Manifest Your Desires Into Reality Using The Law of Attraction: Learn the Secret to Overcoming Your Current Problems and Limitations, Attaining Your Goals, and Achieving Health, Wealth, Happiness and Success!Valutazione: 5 su 5 stelle5/5 (284)
- Love Yourself, Heal Your Life Workbook (Insight Guide)Da EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Valutazione: 5 su 5 stelle5/5 (40)
- Peaceful Sleep Hypnosis: Meditate & RelaxDa EverandPeaceful Sleep Hypnosis: Meditate & RelaxValutazione: 4.5 su 5 stelle4.5/5 (142)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (169)
- How to Walk into a Room: The Art of Knowing When to Stay and When to Walk AwayDa EverandHow to Walk into a Room: The Art of Knowing When to Stay and When to Walk AwayValutazione: 4.5 su 5 stelle4.5/5 (6)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDa EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningValutazione: 4 su 5 stelle4/5 (3)
- Summary of The Art of Seduction by Robert GreeneDa EverandSummary of The Art of Seduction by Robert GreeneValutazione: 4 su 5 stelle4/5 (46)
- Summary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisDa EverandSummary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- The Three Waves of Volunteers & The New EarthDa EverandThe Three Waves of Volunteers & The New EarthValutazione: 5 su 5 stelle5/5 (179)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Da EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Valutazione: 4 su 5 stelle4/5 (378)
- No Mud, No Lotus: The Art of Transforming SufferingDa EverandNo Mud, No Lotus: The Art of Transforming SufferingValutazione: 5 su 5 stelle5/5 (175)
- Forever Strong: A New, Science-Based Strategy for Aging WellDa EverandForever Strong: A New, Science-Based Strategy for Aging WellNessuna valutazione finora
- The Waitress: The gripping, edge-of-your-seat psychological thriller from the bestselling author of The BridesmaidDa EverandThe Waitress: The gripping, edge-of-your-seat psychological thriller from the bestselling author of The BridesmaidValutazione: 4 su 5 stelle4/5 (65)