Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
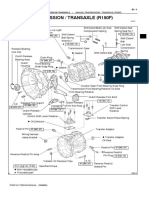
- Manual Transmission (R150F)Documento3 pagineManual Transmission (R150F)daniel_gustavo_2002100% (4)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Product Technical Application Guide: Volvo RemanDocumento49 pagineProduct Technical Application Guide: Volvo RemanJonah RagleNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Texas Everyday Mathematics Grade 3 - Student Reference BookDocumento381 pagineTexas Everyday Mathematics Grade 3 - Student Reference BookTuyếnĐặng100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Terminals of EcmDocumento10 pagineTerminals of Ecmjorge luis guevara martinezNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Piper PA-34-200T Seneca II Manual PDFDocumento23 paginePiper PA-34-200T Seneca II Manual PDFMuhammad Naveed0% (1)
- Pumps, Valves, & Fans: Moving FluidsDocumento33 paginePumps, Valves, & Fans: Moving Fluidskamal_muralikumarNessuna valutazione finora
- 1GR TIMING ToyotaDocumento6 pagine1GR TIMING ToyotaGenaro GonzaleNessuna valutazione finora
- Carraro TLB1 - UP - 4WDDocumento15 pagineCarraro TLB1 - UP - 4WDИрина CML75% (8)
- Hang Out 3 - Unit Test 6Documento2 pagineHang Out 3 - Unit Test 6iSpeak SumbersariNessuna valutazione finora
- Organization and Management of Sports EventDocumento4 pagineOrganization and Management of Sports EventErnan GuevarraNessuna valutazione finora
- Teen Wolf 1x02 - Second Chance at First LineDocumento60 pagineTeen Wolf 1x02 - Second Chance at First LineChristina HuntNessuna valutazione finora
- Saga BLM 1.3 M-Line (M) Spare Parts Price ListDocumento11 pagineSaga BLM 1.3 M-Line (M) Spare Parts Price ListIbnu Asad100% (1)
- Oferta de Pret Rulmenti GenOparts GermaniaDocumento10 pagineOferta de Pret Rulmenti GenOparts GermaniaPopa CatalinNessuna valutazione finora
- AniGame - How To Beat LocsDocumento4 pagineAniGame - How To Beat LocsJoshue Gonz00Nessuna valutazione finora
- Top 10 Cable HM 25-44 ABCDocumento3 pagineTop 10 Cable HM 25-44 ABCVeronica ArteagaNessuna valutazione finora
- Kinematics 1Documento6 pagineKinematics 1Shiva Ram Prasad PulagamNessuna valutazione finora
- Injection Pump Specification ©Documento4 pagineInjection Pump Specification ©johnny sabinNessuna valutazione finora
- 48 TopRigid BrochureDocumento16 pagine48 TopRigid BrochureRonaldo B VillaromanNessuna valutazione finora
- Storyboards and ScenariosDocumento2 pagineStoryboards and ScenariosSiddharth JaiswalNessuna valutazione finora
- Asthma Case Study.Documento6 pagineAsthma Case Study.sammyNessuna valutazione finora
- Nabtesco Item ListDocumento10 pagineNabtesco Item ListAkachat ToufikNessuna valutazione finora
- URW-094 Product SheetDocumento1 paginaURW-094 Product Sheetdiego.peinado8856Nessuna valutazione finora
- Silent Hill 3 Guia InglesDocumento13 pagineSilent Hill 3 Guia InglesTark NerakaNessuna valutazione finora
- Endurace CF SL - CF SLX Disc R36-17 - R054-01-AM - BOM - EL PDFDocumento1 paginaEndurace CF SL - CF SLX Disc R36-17 - R054-01-AM - BOM - EL PDFRoberto EmmeNessuna valutazione finora
- Shariah Judges Paper - Langkawi 2012.3Documento4 pagineShariah Judges Paper - Langkawi 2012.3Adly ZulkeflyNessuna valutazione finora
- Rick Zunigar Resume-BioDocumento5 pagineRick Zunigar Resume-BioRick ZunigarNessuna valutazione finora
- Harbinger - Fitness Guide CablesDocumento2 pagineHarbinger - Fitness Guide Cablesedwin69roNessuna valutazione finora
- Bugatti Veyron Super Sport: World's Fastest Cars: 1Documento7 pagineBugatti Veyron Super Sport: World's Fastest Cars: 1senthilkumar7374Nessuna valutazione finora
- Moto2 Race Results (Mugello 2010)Documento2 pagineMoto2 Race Results (Mugello 2010)AttilaNessuna valutazione finora
- Chapter Four Class 9thDocumento11 pagineChapter Four Class 9thAliNessuna valutazione finora