Potrebbero piacerti anche
- Pathophysiology of Rheumatic Heart DiseaseDocumento3 paginePathophysiology of Rheumatic Heart DiseaseLouie Kem Anthony Babaran50% (8)
- Thyroid Care - A Nine Step Program For Busy WomenDocumento161 pagineThyroid Care - A Nine Step Program For Busy WomenAnisa A Abeytia100% (3)
- Home Study Course-HomeopathDocumento155 pagineHome Study Course-HomeopathAzad Ansari67% (6)
- Yuan and Luo PointsDocumento23 pagineYuan and Luo Pointssale18100% (5)
- Dengue Fever Health TeachingDocumento3 pagineDengue Fever Health TeachingDante Sales100% (3)
- HSE Manager & Supervisor CV - Niranjan 30-04-2021Documento4 pagineHSE Manager & Supervisor CV - Niranjan 30-04-2021NiraNessuna valutazione finora
- Hyperthyroidsm: EpidemiologyDocumento6 pagineHyperthyroidsm: EpidemiologyEllieNessuna valutazione finora
- Thyroid Disorders During PregnancyDocumento25 pagineThyroid Disorders During PregnancyA.H.ANessuna valutazione finora
- Thyroid DX PXLDocumento62 pagineThyroid DX PXLabduljebarNessuna valutazione finora
- Therapeutics: Thyroid DisordersDocumento24 pagineTherapeutics: Thyroid DisordersSharas FarhadNessuna valutazione finora
- Hyperthyroidism: A Practical Approach To Diagnosis and ManagementDocumento70 pagineHyperthyroidism: A Practical Approach To Diagnosis and ManagementMutiara Manuella TambaNessuna valutazione finora
- Grave'S Disease: Farida Ulfa 1510211057Documento11 pagineGrave'S Disease: Farida Ulfa 1510211057farida ulfaNessuna valutazione finora
- Hypothyroid in Pregnancy Andi CakraDocumento32 pagineHypothyroid in Pregnancy Andi CakraCakraEkkyNessuna valutazione finora
- Hypothyroidism in PregnancyDocumento14 pagineHypothyroidism in PregnancyShajia ZafarNessuna valutazione finora
- Pemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKDocumento12 paginePemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKBonitavanyNessuna valutazione finora
- Biol 460 Case StudyDocumento11 pagineBiol 460 Case Studyapi-353888678Nessuna valutazione finora
- Endocrine 160110083024Documento65 pagineEndocrine 160110083024Ryan CracknellNessuna valutazione finora
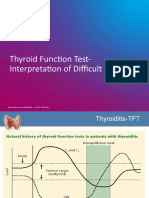
- TFT Interpretation of Difficult CasesDocumento51 pagineTFT Interpretation of Difficult CasesAditya GautamNessuna valutazione finora
- Week 3 Pharmaco Part 2Documento34 pagineWeek 3 Pharmaco Part 2Tiko JomidavaNessuna valutazione finora
- Thyroid Emergencies-Dr. AM IyagbaDocumento13 pagineThyroid Emergencies-Dr. AM IyagbaDr. Amb. Monday ZaccheausNessuna valutazione finora
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocumento22 pagineGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNessuna valutazione finora
- Thyroid and InfertilityDocumento36 pagineThyroid and InfertilitySairindri SahooNessuna valutazione finora
- TPO in PregnancyDocumento18 pagineTPO in PregnancyRoxana TudorNessuna valutazione finora
- Abnormal Thyroid Function in PregnancyDocumento54 pagineAbnormal Thyroid Function in Pregnancyasri khazaliNessuna valutazione finora
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDocumento36 pagineThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaNessuna valutazione finora
- Conference Brochure With Link7Documento16 pagineConference Brochure With Link7Shrutik AshiyaniNessuna valutazione finora
- FunctionTests Brochure PDFDocumento2 pagineFunctionTests Brochure PDFArslan SaleemNessuna valutazione finora
- Thyroid Drug and Calcium Homeostasis - PHD332 - 30112017Documento62 pagineThyroid Drug and Calcium Homeostasis - PHD332 - 30112017Alisa BoonsukNessuna valutazione finora
- CHN1 Health Care Delivery System2Documento22 pagineCHN1 Health Care Delivery System2MicaNessuna valutazione finora
- Variations, Errors, and QualityDocumento46 pagineVariations, Errors, and QualityJohn Reden RomeroNessuna valutazione finora
- Critical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STDocumento24 pagineCritical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STMohammad Naufal AliefNessuna valutazione finora
- Guidelines of The American Thyroid Association PREGNANCY PDFDocumento47 pagineGuidelines of The American Thyroid Association PREGNANCY PDFIqra AnugerahNessuna valutazione finora
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Documento63 pagineClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaNessuna valutazione finora
- Thyroid HormonesDocumento7 pagineThyroid HormonesAbdullah EssaNessuna valutazione finora
- Thyroid Emergencies: Abrar AlharbiDocumento35 pagineThyroid Emergencies: Abrar AlharbiabrarNessuna valutazione finora
- Parathyroid-Hormone Calcium HomeostasisDocumento58 pagineParathyroid-Hormone Calcium HomeostasisSudhakar LakavathNessuna valutazione finora
- '3'hyperthyroid and HypothyroidDocumento42 pagine'3'hyperthyroid and Hypothyroidafriskha bulawanNessuna valutazione finora
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocumento48 pagineLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNessuna valutazione finora
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDocumento38 pagineSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- Thyroiddisease 190216062020Documento42 pagineThyroiddisease 190216062020Manikandan Vp100% (1)
- Laboratory Tests of Thyroid Function: Uses and Limitations: D. Robert Dufour, MDDocumento16 pagineLaboratory Tests of Thyroid Function: Uses and Limitations: D. Robert Dufour, MDStacy SmithNessuna valutazione finora
- Thyroid Function TestDocumento28 pagineThyroid Function TestDhinesh Muthusamy100% (1)
- ThyrotoxicosisDocumento105 pagineThyrotoxicosisAli Murtaza Abbas100% (1)
- 1-Good Health Gold Package - PO2257496339-951Documento1 pagina1-Good Health Gold Package - PO2257496339-951Aafaq BhuttoNessuna valutazione finora
- HYPOTHYROIDISMDocumento30 pagineHYPOTHYROIDISMTopeNessuna valutazione finora
- HyperthyroidDocumento12 pagineHyperthyroidChristine Joy PepitoNessuna valutazione finora
- Hormon GDSDocumento23 pagineHormon GDSBRI KUNessuna valutazione finora
- Hormones and Related DrugsDocumento42 pagineHormones and Related DrugsRamya PrabhuNessuna valutazione finora
- Hypothalamic Pitutary Axis and Thyroid Hormone SynthesisDocumento5 pagineHypothalamic Pitutary Axis and Thyroid Hormone Synthesis78 shivangi mauryaNessuna valutazione finora
- Thyroid Panel-1 (T3/T4/TSH) : Investigation Observed Value Unit Biological Reference IntervalDocumento2 pagineThyroid Panel-1 (T3/T4/TSH) : Investigation Observed Value Unit Biological Reference IntervalShashikantNessuna valutazione finora
- Autoverification ImplementationDocumento53 pagineAutoverification ImplementationEi JamNessuna valutazione finora
- Lab Report NewDocumento2 pagineLab Report Newnsdh5v5v5sNessuna valutazione finora
- Thyroid Function Test: The "Hidden" Health ProblemDocumento34 pagineThyroid Function Test: The "Hidden" Health Problemvjanand07100% (1)
- Thyroid Function Tests (TFTS)Documento27 pagineThyroid Function Tests (TFTS)ธิติวุฒิ แสงคล้อยNessuna valutazione finora
- HipothyroidDocumento48 pagineHipothyroidCakraEkkyNessuna valutazione finora
- Lecture 29 30 Thyroid TherapeuticsDocumento3 pagineLecture 29 30 Thyroid TherapeuticsAhmed MashalyNessuna valutazione finora
- Thyroid DisordersDocumento67 pagineThyroid DisordersMA 09Nessuna valutazione finora
- Thyroid PathophysiologyDocumento7 pagineThyroid PathophysiologyS RiarNessuna valutazione finora
- Fertility: Assessment and Treatment For People With Fertility ProblemsDocumento4 pagineFertility: Assessment and Treatment For People With Fertility ProblemsPatrick CoghlanNessuna valutazione finora
- 10 16 Thyroid Function NitinDocumento7 pagine10 16 Thyroid Function NitinStrawberry ShortcakeNessuna valutazione finora
- Dneerajalaxmi 20220611120615333Documento1 paginaDneerajalaxmi 20220611120615333Donthula SripathiNessuna valutazione finora
- 16 - Hypo and HyperthyroidismDocumento58 pagine16 - Hypo and HyperthyroidismRouda Abdulla100% (1)
- Im Testing For Endocrine DisordersDocumento7 pagineIm Testing For Endocrine DisordersChristine MendozaNessuna valutazione finora
- Deepika.R:::: Patient Age / Sex 26 Y / Female BranchDocumento2 pagineDeepika.R:::: Patient Age / Sex 26 Y / Female BranchkannanNessuna valutazione finora
- Hyperthyroid Is Med ItDocumento31 pagineHyperthyroid Is Med ItJuliana Sanjaya VocNessuna valutazione finora
- BEC-1A June 19, 2016Documento134 pagineBEC-1A June 19, 2016Louie Kem Anthony BabaranNessuna valutazione finora
- Kahit Maputi Na Ang Buhok KoDocumento13 pagineKahit Maputi Na Ang Buhok KoLouie Kem Anthony Babaran100% (1)
- Downloaded From Perfect Notes and Guitar Tabs SearcherDocumento30 pagineDownloaded From Perfect Notes and Guitar Tabs SearcherLouie Kem Anthony BabaranNessuna valutazione finora
- The Moral Issue of Paternalism and Truth TellingDocumento4 pagineThe Moral Issue of Paternalism and Truth TellingLouie Kem Anthony Babaran0% (2)
- Pork Binagoongan RecipeDocumento1 paginaPork Binagoongan RecipeLouie Kem Anthony BabaranNessuna valutazione finora
- AtherosclerosisDocumento11 pagineAtherosclerosisLouie Kem Anthony BabaranNessuna valutazione finora
- Borrelia SPP Are Gram Negative Helical Bacteria: Rickketsia Tsutsugamushi Is The CausativeDocumento1 paginaBorrelia SPP Are Gram Negative Helical Bacteria: Rickketsia Tsutsugamushi Is The CausativeLouie Kem Anthony BabaranNessuna valutazione finora
- Fundamentals in NursingDocumento2 pagineFundamentals in NursingLouie Kem Anthony BabaranNessuna valutazione finora
- I Wont Give UpDocumento9 pagineI Wont Give UpRose AnnNessuna valutazione finora
- Cake Decorating RubricDocumento1 paginaCake Decorating RubricLouie Kem Anthony BabaranNessuna valutazione finora
- Who Am IDocumento30 pagineWho Am ILouie Kem Anthony BabaranNessuna valutazione finora
- Mental Health and Mental DisordersDocumento24 pagineMental Health and Mental DisordersLouie Kem Anthony BabaranNessuna valutazione finora
- Perioperative NursingDocumento9 paginePerioperative NursingLouie Kem Anthony BabaranNessuna valutazione finora
- Pathophysiology PP FinalDocumento2 paginePathophysiology PP FinalLouie Kem Anthony Babaran0% (1)
- On Pies and PastriesDocumento44 pagineOn Pies and PastriesLouie Kem Anthony Babaran100% (2)
- Pie Details Fact or FictionDocumento2 paginePie Details Fact or FictionLouie Kem Anthony BabaranNessuna valutazione finora
- Single-Crust Pie Demo FormDocumento2 pagineSingle-Crust Pie Demo FormLouie Kem Anthony BabaranNessuna valutazione finora
- Case Presentation On CholelithiasisDocumento24 pagineCase Presentation On CholelithiasisLouie Kem Anthony Babaran100% (1)
- Jamica L. Ramirez Bsn-4 Set2Documento44 pagineJamica L. Ramirez Bsn-4 Set2Louie Kem Anthony BabaranNessuna valutazione finora
- Sites of An Ectopic Pregnancy AreDocumento11 pagineSites of An Ectopic Pregnancy AreLouie Kem Anthony BabaranNessuna valutazione finora
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocumento2 pagineAssessment Diagnosis Planning Intervention Rationale EvaluationLouie Kem Anthony BabaranNessuna valutazione finora
- Or InstrumentDocumento1 paginaOr InstrumentLouie Kem Anthony BabaranNessuna valutazione finora
- Matt SantiagoDocumento1 paginaMatt SantiagoJillian Lee NadiakNessuna valutazione finora
- Chaos, Solitons and Fractals: Vinay Kumar Reddy Chimmula, Lei ZhangDocumento6 pagineChaos, Solitons and Fractals: Vinay Kumar Reddy Chimmula, Lei ZhangS AbdNessuna valutazione finora
- Subdermal HematomaDocumento2 pagineSubdermal HematomaDristi KhanalNessuna valutazione finora
- Government of Kerala: Read 1 GO (RT) No. 396/2021/DMD Dated 03/05/2021Documento3 pagineGovernment of Kerala: Read 1 GO (RT) No. 396/2021/DMD Dated 03/05/2021hpindigo clubNessuna valutazione finora
- 30 BÀI LUẬN MẪU DÀNH CHO HS CẤP 2Documento7 pagine30 BÀI LUẬN MẪU DÀNH CHO HS CẤP 2Đào Thị HảiNessuna valutazione finora
- School of Health and Natural Sciences Nursing DepartmentDocumento52 pagineSchool of Health and Natural Sciences Nursing DepartmentJosephine Mae TumanutNessuna valutazione finora
- California Retailers Guide To Hazardous Waste ComplianceDocumento4 pagineCalifornia Retailers Guide To Hazardous Waste ComplianceStericycle100% (1)
- Pharmacological and Parenteral TherapiesDocumento99 paginePharmacological and Parenteral TherapieslNessuna valutazione finora
- English Acad Module and Activity MODULE 1 WEEK 1 2Documento9 pagineEnglish Acad Module and Activity MODULE 1 WEEK 1 2Genesis PalmaNessuna valutazione finora
- Shankar BillingDocumento5 pagineShankar BillingUdayan PandaNessuna valutazione finora
- AKAPULKODocumento4 pagineAKAPULKOMaricelPlacioNessuna valutazione finora
- Emotional Intelligence in LEADERSDocumento77 pagineEmotional Intelligence in LEADERSImran MalikNessuna valutazione finora
- Culture Bound Syndromes NotesDocumento7 pagineCulture Bound Syndromes NotesPragnya NidugondaNessuna valutazione finora
- Echocardiography in Coronary Artery DiseaseDocumento277 pagineEchocardiography in Coronary Artery DiseaseMichael HartNessuna valutazione finora
- Beyond OralityDocumento27 pagineBeyond OralityYnon WeismanNessuna valutazione finora
- 3304 Part B DCHB Vellore PDFDocumento432 pagine3304 Part B DCHB Vellore PDFrajashekhar asNessuna valutazione finora
- SPF 55 BrochureDocumento2 pagineSPF 55 Brochureapi-528907705Nessuna valutazione finora
- Case Analysis PaperDocumento2 pagineCase Analysis PaperKukugirl DavisNessuna valutazione finora
- 6.-Organic-Resource-Agency-v4-170915-AH-food Waste in ScotlandDocumento27 pagine6.-Organic-Resource-Agency-v4-170915-AH-food Waste in ScotlandVita NurhikmahNessuna valutazione finora
- Emergency HandbookDocumento96 pagineEmergency HandbookZenith Sabando Manawatao100% (1)
- Primary Containment For BiohazardsDocumento21 paginePrimary Containment For BiohazardschitradeviNessuna valutazione finora
- Correlates To Work-Related Stress of Newly-Graduated Nurses in Critical-Care UnitsDocumento11 pagineCorrelates To Work-Related Stress of Newly-Graduated Nurses in Critical-Care UnitsbabiNessuna valutazione finora
- KYOKUSHIN KARATE NutritionDocumento14 pagineKYOKUSHIN KARATE Nutritionwaqar aliNessuna valutazione finora
- Checklist With RationalesDocumento174 pagineChecklist With RationalesZoey Francisco100% (1)
- Introductions: Important Grammar RulesDocumento11 pagineIntroductions: Important Grammar RulesyazzNessuna valutazione finora
- Total NutritionDocumento5 pagineTotal NutritionSmiley ShariffNessuna valutazione finora