Potrebbero piacerti anche
- 2000-WHO Drug Information Vol. 14 - No. 4 PDFDocumento79 pagine2000-WHO Drug Information Vol. 14 - No. 4 PDFAngela Castro RNessuna valutazione finora
- 10 Reasons To Legalize All DrugsDocumento2 pagine10 Reasons To Legalize All Drugsbebbydear123Nessuna valutazione finora
- DPA Fact Sheet Criminalization of Prescription Drug UseDocumento1 paginaDPA Fact Sheet Criminalization of Prescription Drug Usewebmaster@drugpolicy.orgNessuna valutazione finora
- Drugs Dilemmas and ChoicesDocumento304 pagineDrugs Dilemmas and ChoicesClément JanequinNessuna valutazione finora
- MASS Pharmacy Law 2014Documento313 pagineMASS Pharmacy Law 20147bostondrNessuna valutazione finora
- PEAC Prescription Drug MisuseDocumento25 paginePEAC Prescription Drug MisuseSdNessuna valutazione finora
- Drug Schedules and Prescription Writing Clifford M. Knapp, PH.DDocumento36 pagineDrug Schedules and Prescription Writing Clifford M. Knapp, PH.DEman ElzeftawyNessuna valutazione finora
- FDA-Drug Disposal GuidelineDocumento2 pagineFDA-Drug Disposal GuidelineDian PusNessuna valutazione finora
- Detox OverviewDocumento6 pagineDetox OverviewLauren ENessuna valutazione finora
- Pharmacist CV TemplateDocumento2 paginePharmacist CV TemplatevractivaNessuna valutazione finora
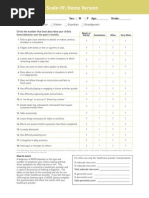
- Screening ADHDDocumento2 pagineScreening ADHDPsiholog Alina Mirela CraiuNessuna valutazione finora
- Prohibited DrugsDocumento3 pagineProhibited Drugswild girl100% (1)
- Critical Issues in Alcohol and Drugs of Abuse TestingDa EverandCritical Issues in Alcohol and Drugs of Abuse TestingNessuna valutazione finora
- Meditation For Kids - PDFDocumento18 pagineMeditation For Kids - PDFJamesNessuna valutazione finora
- SUD I - Opioid-Related Disorders Cheat Sheet: by ViaDocumento4 pagineSUD I - Opioid-Related Disorders Cheat Sheet: by ViaDonatella S.Nessuna valutazione finora
- Drug and Pharmacy Regulation ActDocumento12 pagineDrug and Pharmacy Regulation ActrajvirNessuna valutazione finora
- Implementation of Anti-Drug CampaignDocumento40 pagineImplementation of Anti-Drug Campaignjake beseraNessuna valutazione finora
- Language of Addiction MedicineDocumento16 pagineLanguage of Addiction MedicineChristopher CookNessuna valutazione finora
- Ketamine For Opiate WithdrawalDocumento3 pagineKetamine For Opiate WithdrawalroboNessuna valutazione finora
- Gombos, Justin - Fooling The Bladder Cops - The Complete Drug Testing Guide PDFDocumento85 pagineGombos, Justin - Fooling The Bladder Cops - The Complete Drug Testing Guide PDFJózsa VilmosNessuna valutazione finora
- The Cancer of Our Society: DrugsDocumento14 pagineThe Cancer of Our Society: DrugsAman Maity100% (1)
- Treatment Approaches For Drug Addiction DrugfactsDocumento10 pagineTreatment Approaches For Drug Addiction DrugfactsMustafa AlmasoudiNessuna valutazione finora
- Pharmacogenetics and PharmacogenomicsDocumento25 paginePharmacogenetics and PharmacogenomicsBogdan CoșmanNessuna valutazione finora
- Yy Yyy Y Yy Y YYYDocumento64 pagineYy Yyy Y Yy Y YYYsreedam100% (1)
- CH 8. Laws Governing The Practice of PharmacyDocumento62 pagineCH 8. Laws Governing The Practice of Pharmacyaberhaneth1163Nessuna valutazione finora
- 150Documento68 pagine150Andrei Miguel RoqueNessuna valutazione finora
- Drug Information ResourcesDocumento34 pagineDrug Information ResourceslucaNessuna valutazione finora
- Substance Use Disorder - Manual For PhysiciansDocumento213 pagineSubstance Use Disorder - Manual For PhysiciansRoh JitenNessuna valutazione finora
- Medical History FormDocumento16 pagineMedical History FormSpreadsheetZONENessuna valutazione finora
- Study of Women Drug UsersDocumento177 pagineStudy of Women Drug UsersIrfan AhmadNessuna valutazione finora
- Modifiers-Table 122015 2Documento25 pagineModifiers-Table 122015 2khatNessuna valutazione finora
- IT 8 - MTK Drug AbuseDocumento223 pagineIT 8 - MTK Drug AbusedeviamufidazaharaNessuna valutazione finora
- Pharmaceutical CareDocumento114 paginePharmaceutical CareRisdaFitriaNessuna valutazione finora
- 8-22-16-Lecture Grand Rounds Drug Drug Interactions PDFDocumento44 pagine8-22-16-Lecture Grand Rounds Drug Drug Interactions PDFCastov LiubițaNessuna valutazione finora
- Impurity Profiling and Drug Characterization: Backdrop and ApproachDocumento17 pagineImpurity Profiling and Drug Characterization: Backdrop and ApproachBaru Chandrasekhar RaoNessuna valutazione finora
- Sources Drug InfoDocumento16 pagineSources Drug InfoAhmed ZakariaNessuna valutazione finora
- Professional Competencies For Canadian Pharmacy Technicians at Entry To PracticeDocumento26 pagineProfessional Competencies For Canadian Pharmacy Technicians at Entry To PracticeAnonymous jVZOuTNessuna valutazione finora
- Managing Clinical PracticeDocumento46 pagineManaging Clinical PracticeAhmad MakhloufNessuna valutazione finora
- Drug Approval & RegulationDocumento62 pagineDrug Approval & Regulationadni_wgNessuna valutazione finora
- 8 GCP R2 ICH TraduccionDocumento78 pagine8 GCP R2 ICH TraduccionGuillermo PocoviNessuna valutazione finora
- TriageDocumento40 pagineTriagerizka50% (2)
- Novel Drug Delivery Techniques-A Changing and Challenging Global ScenarioDocumento15 pagineNovel Drug Delivery Techniques-A Changing and Challenging Global ScenarioARUNKANTH KRISHNAKUMARNessuna valutazione finora
- Safety Data Sheet Quorum Red Ii: Section 1. Product and Company IdentificationDocumento11 pagineSafety Data Sheet Quorum Red Ii: Section 1. Product and Company IdentificationMauricio Camarena100% (1)
- Chapter 3 Rationality of DrugsDocumento56 pagineChapter 3 Rationality of DrugsS.Srinivasan ('Chinu'); Renu KhannaNessuna valutazione finora
- Detox of The Opiate Dependent Pain Patient and Ongoing Pain Control No Diag 12 13 08Documento14 pagineDetox of The Opiate Dependent Pain Patient and Ongoing Pain Control No Diag 12 13 08Rick Chavez, M.D.100% (1)
- Drug ScreenDocumento94 pagineDrug ScreenardodotNessuna valutazione finora
- Dawson Compton Grant 2010Documento10 pagineDawson Compton Grant 2010Francisco Porá TuzinkievichNessuna valutazione finora
- Medical Conditions HandoutDocumento19 pagineMedical Conditions HandoutMPPNessuna valutazione finora
- Alcohol and DrugsDocumento16 pagineAlcohol and DrugsPame RománNessuna valutazione finora
- 9b) Medical Complications of Drug TakingDocumento19 pagine9b) Medical Complications of Drug TakingDr. Zirwa AsimNessuna valutazione finora
- Health Article - Illicit Drugs and Drug InteractionsDocumento6 pagineHealth Article - Illicit Drugs and Drug Interactions733Nessuna valutazione finora
- Heroin Addiction PaperDocumento9 pagineHeroin Addiction Paperapi-400796139Nessuna valutazione finora
- Evans, D., 2013. The Economic Impacts of Marijuana Legalization.Documento39 pagineEvans, D., 2013. The Economic Impacts of Marijuana Legalization.maja0205Nessuna valutazione finora
- NDPS Saliet FeatyresDocumento63 pagineNDPS Saliet FeatyrespzohmingthangaNessuna valutazione finora
- Oklahoma's Low-THC LawDocumento1 paginaOklahoma's Low-THC LawMPPNessuna valutazione finora
- Psychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDocumento18 paginePsychopharmacologic Drugs: - Antipsychotic Agents - Antimanic Drugs - Antidepressant DrugsDrima EdiNessuna valutazione finora
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDocumento1 paginaSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNessuna valutazione finora
- Irrational Drug CombiDocumento2 pagineIrrational Drug CombiabkinareNessuna valutazione finora
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceDa EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceValutazione: 3 su 5 stelle3/5 (1)
- Pharmacovigilance Ensuring The Safe Use of MedicinesDocumento18 paginePharmacovigilance Ensuring The Safe Use of MedicinespopadrianionutzNessuna valutazione finora
- Problems of Irrational Drug Use: Session GuideDocumento22 pagineProblems of Irrational Drug Use: Session Guidearyo aryoNessuna valutazione finora
- Poly PharmacyDocumento17 paginePoly PharmacyAubrey ManimtimNessuna valutazione finora
- RUM NewDocumento53 pagineRUM NewbennyNessuna valutazione finora
- Anatomyofthe Annexesofthe Digestive TractDocumento67 pagineAnatomyofthe Annexesofthe Digestive TractsreedamNessuna valutazione finora
- Dose AdjustmentDocumento30 pagineDose AdjustmentsreedamNessuna valutazione finora
- Barrons 333 High Freq Words With Meanings PDFDocumento8 pagineBarrons 333 High Freq Words With Meanings PDFahmedhussien1Nessuna valutazione finora
- Fundamentals of SalivaDocumento15 pagineFundamentals of SalivasreedamNessuna valutazione finora
- Scribe 4Documento4 pagineScribe 4sreedamNessuna valutazione finora
- Standard Treatment GuidelineDocumento261 pagineStandard Treatment GuidelineEmaNessuna valutazione finora
- Unit 5-Soil Science Soil FertilityDocumento20 pagineUnit 5-Soil Science Soil FertilitysreedamNessuna valutazione finora
- Dental ProductsDocumento13 pagineDental ProductssreedamNessuna valutazione finora
- Thompson & Thompson Genetics in Medicine Genetik EthicDocumento21 pagineThompson & Thompson Genetics in Medicine Genetik EthickartalxyusufNessuna valutazione finora
- UntitledDocumento6 pagineUntitledPriscilla GabanamotseNessuna valutazione finora
- Medical Treatment Recuperation Convalescence With HomoeopathyDocumento4 pagineMedical Treatment Recuperation Convalescence With HomoeopathyEditor IJTSRDNessuna valutazione finora
- PPT Referat Syok Argia AnjaniDocumento34 paginePPT Referat Syok Argia Anjanidhana2395Nessuna valutazione finora
- FluidDocumento190 pagineFluidAndrias OzNessuna valutazione finora
- Module 5 MGCQ Edition The Physical and Sexual SelfDocumento28 pagineModule 5 MGCQ Edition The Physical and Sexual SelfRan Dy MangosingNessuna valutazione finora
- Guide Questions For NCM 107Documento4 pagineGuide Questions For NCM 107Miguel LigasNessuna valutazione finora
- Homework PaperDocumento12 pagineHomework Paperapi-509662228Nessuna valutazione finora
- Regulatory Bodies of Nursing in India: Dr. Maheswari JaikumarDocumento75 pagineRegulatory Bodies of Nursing in India: Dr. Maheswari Jaikumarkalla sharonNessuna valutazione finora
- GMC Handwara Recruitment 2023Documento4 pagineGMC Handwara Recruitment 2023Ummar WaniNessuna valutazione finora
- The Early Trauma Inventory Self Report-Short FormDocumento8 pagineThe Early Trauma Inventory Self Report-Short FormMiguel Angel Alemany NaveirasNessuna valutazione finora
- InBody 270Documento27 pagineInBody 270lee CeeNessuna valutazione finora
- Physical Fitness TestDocumento5 paginePhysical Fitness TestJhona Nodado RiveraNessuna valutazione finora
- Mo2vate Issue 15 - March 2022Documento74 pagineMo2vate Issue 15 - March 2022Mo2vate MagazineNessuna valutazione finora
- Reflection 1Documento5 pagineReflection 1api-400554289Nessuna valutazione finora
- Product Monograph of TelmisartanDocumento8 pagineProduct Monograph of Telmisartandini hanifaNessuna valutazione finora
- Himachal StatsDocumento115 pagineHimachal StatsVikrant ChaudharyNessuna valutazione finora
- 10 Physical and Mental Benefits of BasketballDocumento4 pagine10 Physical and Mental Benefits of BasketballJohn Kenzo NavatoNessuna valutazione finora
- Ab Respiratory Assessment NPG GuidelinesDocumento10 pagineAb Respiratory Assessment NPG GuidelinesSuhaila NajibNessuna valutazione finora
- FARC-01 - Senior First Aid (Occupational First Aid Course OFAC)Documento2 pagineFARC-01 - Senior First Aid (Occupational First Aid Course OFAC)Ewien Vars SianturieNessuna valutazione finora
- Burning Mouth SyndromeDocumento28 pagineBurning Mouth SyndromeMelissa KanggrianiNessuna valutazione finora
- STROBE Case-Control Study PDFDocumento3 pagineSTROBE Case-Control Study PDFLuis Gabriel Parra LaraNessuna valutazione finora
- Nifedipine and Prednisone Drug StudyDocumento4 pagineNifedipine and Prednisone Drug StudyJomer GonzalesNessuna valutazione finora
- Supporting Young Children's Emotional Well-Being: Cumbria County CouncilDocumento32 pagineSupporting Young Children's Emotional Well-Being: Cumbria County CouncilAlbina ScutaruNessuna valutazione finora
- Bacteria and Viruses PDFDocumento1 paginaBacteria and Viruses PDFSchöne Frau TapiaNessuna valutazione finora