Potrebbero piacerti anche
- Switch WordsDocumento65 pagineSwitch WordsAashish Kulkarni97% (34)
- Penis Enlargement Pill IngredientsDocumento7 paginePenis Enlargement Pill Ingredientsspanda091750% (1)
- Welcome TO Intensive Care UnitDocumento42 pagineWelcome TO Intensive Care UnitKharene Lirazan100% (1)
- The Crash CartDocumento39 pagineThe Crash Cartpramod kumawat100% (1)
- ACLS DrugDocumento7 pagineACLS DrugPhongsatorn Thunin100% (1)
- Heart Catheterization & AngioplastyDocumento25 pagineHeart Catheterization & AngioplastyRifa'atul MahmudahNessuna valutazione finora
- American Heart Association Guidelines For CPR 2015: Christopher RyalinoDocumento50 pagineAmerican Heart Association Guidelines For CPR 2015: Christopher RyalinoLightNessuna valutazione finora
- Poster 10 PALS 01 01 ENG V20100927 PDFDocumento1 paginaPoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoNessuna valutazione finora
- ACLS Algorithm GuideDocumento1 paginaACLS Algorithm GuideAhmed AlkhaqaniNessuna valutazione finora
- 2017 05 GC Pocket CardDocumento2 pagine2017 05 GC Pocket Cardapi-312241089Nessuna valutazione finora
- ACLS Study GuideDocumento28 pagineACLS Study GuideNicole Berry100% (1)
- CABG PresentationDocumento55 pagineCABG Presentationnmaykanathan100% (7)
- ACLS Algorithms SlideDocumento26 pagineACLS Algorithms SlidehrsoNessuna valutazione finora
- ACLS Training - Most Important Points To RememberDocumento5 pagineACLS Training - Most Important Points To RememberEman ElzeftawyNessuna valutazione finora
- Rapid Sequence IonDocumento36 pagineRapid Sequence IonSyazwani MohamadNessuna valutazione finora
- Rapid Sequence IntubationDocumento58 pagineRapid Sequence IntubationArya VikneshNessuna valutazione finora
- Atrial Fibrillation and Dysrhythmias GuideDocumento10 pagineAtrial Fibrillation and Dysrhythmias Guideyaneidys perezNessuna valutazione finora
- Acls Manual PDFDocumento30 pagineAcls Manual PDFCyner Cruz100% (2)
- Ecg 01Documento103 pagineEcg 01Bandar al ghamdi100% (1)
- Anatomy and Physiology by Ross and WilsonDocumento21 pagineAnatomy and Physiology by Ross and WilsonAnonymous iEjePNZ50% (2)
- Cardiac Tamponade and ManagementDocumento42 pagineCardiac Tamponade and ManagementRezwanul Hoque Bulbul100% (2)
- Fall Risk Assessment FormDocumento3 pagineFall Risk Assessment FormMichael Silva100% (1)
- AHA ACLS Written Test: Ready To Study? Start With FlashcardsDocumento8 pagineAHA ACLS Written Test: Ready To Study? Start With FlashcardssallyNessuna valutazione finora
- Massive BleedingDocumento32 pagineMassive BleedingJanine Torreon LozaritaNessuna valutazione finora
- ECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial CentreDocumento90 pagineECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial Centrevaishali TayadeNessuna valutazione finora
- 2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes AlgorithmDocumento1 pagina2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes Algorithmms_lezahNessuna valutazione finora
- Ventricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmDocumento2 pagineVentricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmsafasayedNessuna valutazione finora
- Necrotizing Otitis 2022Documento20 pagineNecrotizing Otitis 2022asmashNessuna valutazione finora
- Understanding the Concept of Srotas in AyurvedaDocumento112 pagineUnderstanding the Concept of Srotas in AyurvedaSanjana SajjanarNessuna valutazione finora
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Basic Ecg 2016Documento75 pagineBasic Ecg 2016api-284503860Nessuna valutazione finora
- IU Health ACLS Study GuideDocumento8 pagineIU Health ACLS Study Guideeng78ineNessuna valutazione finora
- Fenestrated Capillaries Distinguishing FeaturesDocumento11 pagineFenestrated Capillaries Distinguishing Featuresمصطفى حسن هاديNessuna valutazione finora
- Cardiac Arrest Drugs & ProceduresDocumento8 pagineCardiac Arrest Drugs & ProceduresAstri Adel BudiarsoNessuna valutazione finora
- CABGDocumento3 pagineCABGprofarmahNessuna valutazione finora
- Haemodynamic MonitoringDocumento6 pagineHaemodynamic MonitoringAnusha Verghese100% (1)
- 12 Lead ECG Mod 1Documento31 pagine12 Lead ECG Mod 1johnmmenahNessuna valutazione finora
- First Grading Periodical Test in Mapeh 6 2017-2018 For Deped ShareDocumento6 pagineFirst Grading Periodical Test in Mapeh 6 2017-2018 For Deped Shareareeya mae factores100% (6)
- Congestive Heart FailureDocumento8 pagineCongestive Heart Failureiancel_038893% (27)
- Surya Namaskar BenefitsDocumento16 pagineSurya Namaskar BenefitsMillion Dollar KnowledgeNessuna valutazione finora
- PMLS 2 PrelimsDocumento55 paginePMLS 2 PrelimsCassey Stephane PinedaNessuna valutazione finora
- DR Yassir Javaid Interpreting The 12 Lead ECGDocumento28 pagineDR Yassir Javaid Interpreting The 12 Lead ECGTirtha TaposhNessuna valutazione finora
- Saudi CPR Guidlines in EnglishDocumento16 pagineSaudi CPR Guidlines in EnglishpiyushbamsNessuna valutazione finora
- Askep AliDocumento34 pagineAskep AliadinsNessuna valutazione finora
- On Emergency DrugsDocumento25 pagineOn Emergency DrugsBikram Chhetry100% (1)
- ACLSDocumento46 pagineACLSYeoh Hong Shin100% (3)
- ACLS and MegacodeDocumento33 pagineACLS and MegacodeMark Joseph100% (1)
- Acls LectureDocumento15 pagineAcls LectureVincent BautistaNessuna valutazione finora
- Advanced Cardiovascular Life Support (ACLS)Documento27 pagineAdvanced Cardiovascular Life Support (ACLS)Sara Ali100% (3)
- ACLS and PALS Certification Practice QuestionsDocumento11 pagineACLS and PALS Certification Practice Questionsdyah rahayu hutamiNessuna valutazione finora
- Cardiac SurgeryDocumento27 pagineCardiac SurgeryReeti Singh100% (1)
- Harris Regional ICU Daily Sedation Vacation GuidelinesDocumento1 paginaHarris Regional ICU Daily Sedation Vacation GuidelinesFebri Yudha Adhi KurniawanNessuna valutazione finora
- ACLS ChartDocumento1 paginaACLS ChartJev DespiNessuna valutazione finora
- Rapid Response TeamDocumento4 pagineRapid Response TeamMichael SilvaNessuna valutazione finora
- Arterial Lines in PACU: Presented by Autum Jacobs RN, BSNDocumento34 pagineArterial Lines in PACU: Presented by Autum Jacobs RN, BSNinuko1212Nessuna valutazione finora
- ECG MonitoringDocumento28 pagineECG MonitoringGlaiza Mae Olivar-ArguillesNessuna valutazione finora
- ACLS 2015 Guidelines for Cardiac Arrest ManagementDocumento13 pagineACLS 2015 Guidelines for Cardiac Arrest ManagementI Gede Aditya100% (5)
- Blood Pressure Drugs ReviewDocumento54 pagineBlood Pressure Drugs ReviewJeremy VivitNessuna valutazione finora
- Management of Arterial LineDocumento16 pagineManagement of Arterial LineFarcasanu Liana GeorgianaNessuna valutazione finora
- CPR Class QuestionnaireDocumento4 pagineCPR Class QuestionnaireParikshit PekhaleNessuna valutazione finora
- ACLS Review Guide for Cardiac Arrest Scenarios and TreatmentDocumento29 pagineACLS Review Guide for Cardiac Arrest Scenarios and TreatmentJB Reyes100% (2)
- Patient Examination GuideDocumento118 paginePatient Examination GuideJun JavierNessuna valutazione finora
- Min Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentDocumento1 paginaMin Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentAlma Alnajjar0% (1)
- CPR AED Choking Guidelines for Healthcare ProvidersDocumento2 pagineCPR AED Choking Guidelines for Healthcare Providersreyes markNessuna valutazione finora
- Terminology Causes of Cardiac Arrest C.P.R. For The Adult, Child & Baby Stroke & Stroke ManagementDocumento28 pagineTerminology Causes of Cardiac Arrest C.P.R. For The Adult, Child & Baby Stroke & Stroke Managementbusiness911Nessuna valutazione finora
- Acls MegacodeDocumento8 pagineAcls Megacodes33d_destinyNessuna valutazione finora
- Post-Cardiac Arrest Management in Adults - UpToDateDocumento34 paginePost-Cardiac Arrest Management in Adults - UpToDatehatsuneNessuna valutazione finora
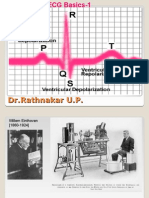
- ECG Basics 1Documento24 pagineECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNessuna valutazione finora
- Introduction Definition: Types of PacemakersDocumento8 pagineIntroduction Definition: Types of PacemakersPrasann RoyNessuna valutazione finora
- ACLS Study GuideDocumento30 pagineACLS Study GuidemmmmzNessuna valutazione finora
- Spinal Cord Injuries-KyienDocumento25 pagineSpinal Cord Injuries-KyienjohnnyienNessuna valutazione finora
- Cardiovascular EmergenciesDocumento20 pagineCardiovascular EmergenciesJohn FisherNessuna valutazione finora
- ICU Scoring Systems A Complete Guide - 2020 EditionDa EverandICU Scoring Systems A Complete Guide - 2020 EditionNessuna valutazione finora
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Final Announcement PIT7 & Mukernas PDUI PDFDocumento8 pagineFinal Announcement PIT7 & Mukernas PDUI PDFAdhydeva PurusantiNessuna valutazione finora
- Dietary Recall: Tanggal Pola Makan Intake Keterangan Jam JenisDocumento1 paginaDietary Recall: Tanggal Pola Makan Intake Keterangan Jam JenisAdhydeva PurusantiNessuna valutazione finora
- Death CaseDocumento18 pagineDeath CaseAdhydeva PurusantiNessuna valutazione finora
- Cover CTG Arini HarlianaDocumento1 paginaCover CTG Arini HarlianaAdhydeva PurusantiNessuna valutazione finora
- EkgDocumento75 pagineEkgAdhydeva PurusantiNessuna valutazione finora
- A Cardiac Contouring Atlas For RadiotherapyDocumento7 pagineA Cardiac Contouring Atlas For RadiotherapyChendil VNessuna valutazione finora
- Post Operative HypotensionDocumento7 paginePost Operative HypotensionbbyesNessuna valutazione finora
- Cardiac Cycle: DR Rakesh JainDocumento97 pagineCardiac Cycle: DR Rakesh JainKemoy FrancisNessuna valutazione finora
- Flyer at A Glance + LecturesDocumento4 pagineFlyer at A Glance + LecturesStella RNessuna valutazione finora
- ASD with Pleural Effusion and AscitesDocumento1 paginaASD with Pleural Effusion and AscitesHapsari Kartika DewiNessuna valutazione finora
- Child Development Milestones and Age-Appropriate Toys for Hospitalized Infants, Toddlers, Preschoolers and School-Aged ChildrenDocumento64 pagineChild Development Milestones and Age-Appropriate Toys for Hospitalized Infants, Toddlers, Preschoolers and School-Aged ChildrenLilly Daye100% (1)
- Electrocardiography - Wikipedia, The Free EncyclopediaDocumento18 pagineElectrocardiography - Wikipedia, The Free Encyclopediapayments8543Nessuna valutazione finora
- P 6-ScienceDocumento8 pagineP 6-ScienceMonydit santinoNessuna valutazione finora
- Trepopnea in CHFDocumento4 pagineTrepopnea in CHFprobowurNessuna valutazione finora
- Heart and Blood VesselsDocumento15 pagineHeart and Blood VesselsIDKNessuna valutazione finora
- Session 11: Heart FailureDocumento41 pagineSession 11: Heart FailureRayan MziriNessuna valutazione finora
- Test Bank For Interpreting Ecgs A Practical Approach 3rd Edition Bruce ShadeDocumento11 pagineTest Bank For Interpreting Ecgs A Practical Approach 3rd Edition Bruce ShadeLisaTurnerMDkfym100% (27)
- Management of Cardiogenic ShockDocumento15 pagineManagement of Cardiogenic ShockcastillojessNessuna valutazione finora
- Assessing Heart and Neck Vessel Heart Heart Chambers: (Tricuspid & Bicuspid)Documento7 pagineAssessing Heart and Neck Vessel Heart Heart Chambers: (Tricuspid & Bicuspid)Dan Floyd FernandezNessuna valutazione finora
- Ghadeer Haider - Finger Heart Rate and Pulse Oximeter Smart SensorDocumento14 pagineGhadeer Haider - Finger Heart Rate and Pulse Oximeter Smart SensorGhadeer HaiderNessuna valutazione finora
- HHW Biology X PDFDocumento9 pagineHHW Biology X PDFNikhil bhatiNessuna valutazione finora