Potrebbero piacerti anche
- RHS 2011Documento44 pagineRHS 2011Esthela LoyoNessuna valutazione finora
- Insuficiencia CardiacaPLCDocumento57 pagineInsuficiencia CardiacaPLCEsthela LoyoNessuna valutazione finora
- Regulacion Inmune 2011Documento25 pagineRegulacion Inmune 2011Esthela LoyoNessuna valutazione finora
- Linfocitos T 2011Documento59 pagineLinfocitos T 2011Esthela LoyoNessuna valutazione finora
- Mhc-Hla 2011Documento43 pagineMhc-Hla 2011Esthela LoyoNessuna valutazione finora
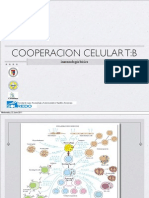
- Cooperación Celular 2011Documento22 pagineCooperación Celular 2011Esthela LoyoNessuna valutazione finora
- Bases Tto HiperlipidemiasDocumento63 pagineBases Tto HiperlipidemiasEsthela LoyoNessuna valutazione finora
- Mhc-Hla 2011Documento43 pagineMhc-Hla 2011Esthela LoyoNessuna valutazione finora
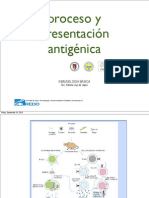
- Proceso y Present AgDocumento30 pagineProceso y Present AgEsthela LoyoNessuna valutazione finora
- Citoquinas CAMS, ComplementoDocumento89 pagineCitoquinas CAMS, ComplementoEsthela Loyo100% (1)
- Mhc-Hla 2011Documento43 pagineMhc-Hla 2011Esthela LoyoNessuna valutazione finora
- MHC HlaDocumento41 pagineMHC HlaEsthela LoyoNessuna valutazione finora
- Celulas y Tejidos, 2011Documento44 pagineCelulas y Tejidos, 2011Esthela LoyoNessuna valutazione finora
- Antígenos: AnticuerposDocumento51 pagineAntígenos: AnticuerposEsthela LoyoNessuna valutazione finora
- ToleranciaDocumento70 pagineToleranciaEsthela Loyo100% (1)
- Proceso y Present Ag 2010Documento35 pagineProceso y Present Ag 2010Esthela LoyoNessuna valutazione finora
- Colaboración Celular en La Respuesta de AnticuerposDocumento36 pagineColaboración Celular en La Respuesta de AnticuerposEsthela LoyoNessuna valutazione finora
- Linfos BDocumento47 pagineLinfos BEsthela LoyoNessuna valutazione finora
- Linfos B 2010Documento36 pagineLinfos B 2010Esthela LoyoNessuna valutazione finora
- Citoquinas Quimoquinas y CAMsDocumento38 pagineCitoquinas Quimoquinas y CAMsEsthela LoyoNessuna valutazione finora
- Anticuerpos y AntígenosDocumento35 pagineAnticuerpos y AntígenosEsthela LoyoNessuna valutazione finora
- CitoquinasDocumento41 pagineCitoquinasEsthela LoyoNessuna valutazione finora
- Linfocitos T 2010Documento40 pagineLinfocitos T 2010Esthela LoyoNessuna valutazione finora
- Células & Órganos Del SIDocumento33 pagineCélulas & Órganos Del SIEsthela LoyoNessuna valutazione finora
- MHC 2010Documento35 pagineMHC 2010Esthela LoyoNessuna valutazione finora
- Linfos B 2010Documento36 pagineLinfos B 2010Esthela LoyoNessuna valutazione finora
- Citotoxicidad 2010Documento34 pagineCitotoxicidad 2010Esthela Loyo100% (1)
- InmunoglobulinasDocumento33 pagineInmunoglobulinasEsthela LoyoNessuna valutazione finora
- Linfocitos T 2010Documento40 pagineLinfocitos T 2010Esthela LoyoNessuna valutazione finora
- Guion Radial Salud y Prevencion Del Dengue Escuela 15 de 6Documento5 pagineGuion Radial Salud y Prevencion Del Dengue Escuela 15 de 6Juan Pablo FernandezNessuna valutazione finora
- Probl-Resueltos (08) 1-3-4-5-7-9-10-12-13-14-15Documento24 pagineProbl-Resueltos (08) 1-3-4-5-7-9-10-12-13-14-15sersolisNessuna valutazione finora
- Técnicas básicas de canto: respiración, apoyo vocal y resonanciaDocumento21 pagineTécnicas básicas de canto: respiración, apoyo vocal y resonanciaMultinegocios Internacional100% (6)
- 2 Pti Cusco 1Documento7 pagine2 Pti Cusco 1Luz Elena Miranda HernandezNessuna valutazione finora
- Patologia AviarDocumento6 paginePatologia AviarDanteEnrriquezGamezNessuna valutazione finora
- Tipos de Circulación SanguíneaDocumento2 pagineTipos de Circulación SanguíneaEspeRed Para TodosNessuna valutazione finora
- Examen Soluciones Operaciones Administrativas Modelo ADocumento13 pagineExamen Soluciones Operaciones Administrativas Modelo Acarlos ANessuna valutazione finora
- Complicaciones de La PancreatitisDocumento79 pagineComplicaciones de La Pancreatitispaul alvaNessuna valutazione finora
- Cirugia General 1Documento50 pagineCirugia General 1ANtonyMV100% (1)
- Medicina ModernaDocumento31 pagineMedicina ModernaJennifer Ariadna Perez CastellanosNessuna valutazione finora
- Cie 10Documento7 pagineCie 10dyeret95% (22)
- El TulipánDocumento2 pagineEl TulipánmariaNessuna valutazione finora
- Calidad de Los Alimentos Trofoterapia Usmp 2014Documento78 pagineCalidad de Los Alimentos Trofoterapia Usmp 2014Víctor Artica100% (1)
- Tacto y sensibilidad diferencial en el cuerpo humanoDocumento1 paginaTacto y sensibilidad diferencial en el cuerpo humanoAlejandro CarcamoNessuna valutazione finora
- Normas Oficiales MexicanasDocumento11 pagineNormas Oficiales MexicanasBere Arias100% (1)
- Hervario de BotanicaDocumento7 pagineHervario de BotanicaAlvert Wen CientNessuna valutazione finora
- Inseminacion ArtificialDocumento53 pagineInseminacion ArtificialAnonymous qHoHXaIz78Nessuna valutazione finora
- Formulario N°1 Ficha Clínica Epidemiológica 1Documento2 pagineFormulario N°1 Ficha Clínica Epidemiológica 1HECTOR ROLY ACHACOLLO MARTINEZNessuna valutazione finora
- Cuáles Son Las Enzimas de La Digestión de CarbohidratosDocumento4 pagineCuáles Son Las Enzimas de La Digestión de CarbohidratosRosa SanchezNessuna valutazione finora
- Texto Lakoff Liquidez DiagnosticaDocumento7 pagineTexto Lakoff Liquidez DiagnosticaRolandoJaimeNessuna valutazione finora
- Medicina AlternativaDocumento12 pagineMedicina Alternativajeampol yallico chamorroNessuna valutazione finora
- Drenaje de AbscesosDocumento15 pagineDrenaje de AbscesosDariely Ramis GuzmánNessuna valutazione finora
- Cro No GramaDocumento6 pagineCro No GramaEstefa Carabali QuiñonesNessuna valutazione finora
- Tesis I - Anemia - Margory ImprimirDocumento35 pagineTesis I - Anemia - Margory Imprimirjgonzales_323696Nessuna valutazione finora
- Balance HidricoDocumento14 pagineBalance Hidricojoao zarateNessuna valutazione finora
- TanatologíaDocumento6 pagineTanatologíaYei LiNessuna valutazione finora
- Trastorno Límite de La PersonalidadDocumento33 pagineTrastorno Límite de La Personalidadpepe martinez100% (1)
- Cadena de SupervivenciaDocumento10 pagineCadena de SupervivenciaJoleyda Pinto ColqueNessuna valutazione finora
- Narcotrafico: Amapola en El PeruDocumento24 pagineNarcotrafico: Amapola en El Peruhans waldeNessuna valutazione finora
- Ejemplo Auditoria Interna HospitalDocumento8 pagineEjemplo Auditoria Interna HospitalGabriella QuinteroNessuna valutazione finora