Potrebbero piacerti anche
- Assessment of the Politraumatized PatientDa EverandAssessment of the Politraumatized PatientNessuna valutazione finora
- Iii. Physical Assessment and Review of SystemDocumento7 pagineIii. Physical Assessment and Review of SystemBiya MacunteNessuna valutazione finora
- OB Patho Assessment Tool EditedDocumento6 pagineOB Patho Assessment Tool EditedDarren RobertoNessuna valutazione finora
- Preparation Worksheets For NUR 345 Heart Failure SimDocumento14 paginePreparation Worksheets For NUR 345 Heart Failure SimclarimerNessuna valutazione finora
- 2 Abdomen Checklist 1Documento3 pagine2 Abdomen Checklist 1Angela DancelNessuna valutazione finora
- 01 Nursing Note SampleDocumento1 pagina01 Nursing Note Sampletesttest testNessuna valutazione finora
- Care PlanDocumento11 pagineCare PlanCathy GewontNessuna valutazione finora
- Physician EvaluationDocumento6 paginePhysician Evaluationbartoncreekal100% (2)
- Cagayan de Oro City College of Nursing Assessment Form General InformationDocumento11 pagineCagayan de Oro City College of Nursing Assessment Form General Informationdjanggo18Nessuna valutazione finora
- Tgs Ibu Ellen 1Documento11 pagineTgs Ibu Ellen 1rosna wallyNessuna valutazione finora
- Case Study (Iph) Amoebiasis Diarrhea With Mild DHNDocumento9 pagineCase Study (Iph) Amoebiasis Diarrhea With Mild DHNLance_Joshua_7907Nessuna valutazione finora
- Clinical Pathway For Hypertensive Urgency (Revised)Documento6 pagineClinical Pathway For Hypertensive Urgency (Revised)Heide Danica A. BaltazarNessuna valutazione finora
- Tgas Ibu LlenDocumento10 pagineTgas Ibu LlenFifi FebriantiNessuna valutazione finora
- Case-Study-2 AsthmaDocumento5 pagineCase-Study-2 Asthmaangelica dizon100% (1)
- Telemetry Recognition WorkbookDocumento29 pagineTelemetry Recognition WorkbookQueenNessuna valutazione finora
- Complete COVID AdmissionVentilation Decision Tree Formatted 1Documento4 pagineComplete COVID AdmissionVentilation Decision Tree Formatted 1Beauty NightlymareNessuna valutazione finora
- BlehDocumento3 pagineBlehkula diamondNessuna valutazione finora
- Last CareplanDocumento22 pagineLast CareplanNneka Adaeze AnyanwuNessuna valutazione finora
- Nursing Care Plan Example NR450Documento8 pagineNursing Care Plan Example NR450J15Nessuna valutazione finora
- Nursing Concept Map 1Documento3 pagineNursing Concept Map 1Norah Okafor Ezike67% (3)
- Heath Assessment ToolDocumento8 pagineHeath Assessment ToolHouda Hayek100% (1)
- Labor Room and NurseryDocumento2 pagineLabor Room and NurseryLecery Sophia WongNessuna valutazione finora
- Baystate Med CTR Rapid Response Team Recordwith SBARDocumento3 pagineBaystate Med CTR Rapid Response Team Recordwith SBARDanishyana DhiwaneoNessuna valutazione finora
- Physical AssessmentDocumento51 paginePhysical AssessmentJasmin Jacob100% (2)
- Diabetic Evaluation (Adults Only) : Form To Be Completed by StudentDocumento2 pagineDiabetic Evaluation (Adults Only) : Form To Be Completed by StudentNabeel ShahzadNessuna valutazione finora
- Case Study Jim SandersonDocumento6 pagineCase Study Jim SandersonJessica McAlexanderNessuna valutazione finora
- Admit OrdersDocumento2 pagineAdmit OrdersTariq Niaz Ahmad, MDNessuna valutazione finora
- P.A. Tool (Case Pres FINAL.)Documento23 pagineP.A. Tool (Case Pres FINAL.)Crystal Ann TadiamonNessuna valutazione finora
- 2.physical E, HISTORY NCPDocumento13 pagine2.physical E, HISTORY NCPمريم حجيNessuna valutazione finora
- RevisedDocumento16 pagineRevisedZymer Lee AbasoloNessuna valutazione finora
- Neuro AssessmentDocumento42 pagineNeuro AssessmentLydia Lopz MsnrncdNessuna valutazione finora
- Nursing Care Plan PackageCDocumento23 pagineNursing Care Plan PackageCralsadat100% (1)
- Intestnal ObstructionDocumento4 pagineIntestnal ObstructionRenea Joy ArruejoNessuna valutazione finora
- (193213049) Putu Riska Pramudita DewiDocumento10 pagine(193213049) Putu Riska Pramudita DewiDianNessuna valutazione finora
- ChartingDocumento3 pagineChartingLorina Lynne ApelacioNessuna valutazione finora
- Head-To-Toe Checklist: Beautiful Nursing LLCDocumento4 pagineHead-To-Toe Checklist: Beautiful Nursing LLCcarlyNessuna valutazione finora
- Pharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDocumento20 paginePharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDzaky UlayyaNessuna valutazione finora
- Mang Kanor ROSDocumento2 pagineMang Kanor ROSChamelli RobinNessuna valutazione finora
- Head To ToeDocumento4 pagineHead To Toenazbeen.ahmadiNessuna valutazione finora
- Care Plan For CHFDocumento9 pagineCare Plan For CHFJon Djchimz IsidroNessuna valutazione finora
- Assessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationDocumento10 pagineAssessment Needs Nursing Diagnos IS Goal/Obj Ective Intervention Rationale EvaluationApol Pen67% (3)
- Welcome To Orthopedics Care Center !Documento2 pagineWelcome To Orthopedics Care Center !Ahmed M. RafatNessuna valutazione finora
- Competency Assessment Exam For Nurses: Qibah Hospital Qibah, Algassim, KsaDocumento4 pagineCompetency Assessment Exam For Nurses: Qibah Hospital Qibah, Algassim, KsaSherina W. Edding100% (1)
- Acute Kidney Failure Assesment FormDocumento5 pagineAcute Kidney Failure Assesment FormAahad AmeenNessuna valutazione finora
- Documentation in Your 3 Year and Beyond: Summer Quarter 2010Documento32 pagineDocumentation in Your 3 Year and Beyond: Summer Quarter 2010Roberto ParedesNessuna valutazione finora
- Nifedipine 30 MG 1tab PO OD : SPS Shaina Sango SN, SJPIICDDocumento17 pagineNifedipine 30 MG 1tab PO OD : SPS Shaina Sango SN, SJPIICDInnocent-j CartagenaNessuna valutazione finora
- Case Study Medical WardDocumento14 pagineCase Study Medical WardJoshNessuna valutazione finora
- Csu, Stanislaus B.S.N. Clinical Plan of Care Patient DataDocumento18 pagineCsu, Stanislaus B.S.N. Clinical Plan of Care Patient Dataapi-284664489Nessuna valutazione finora
- Antepartum Record Labor WatchDocumento4 pagineAntepartum Record Labor WatchMaryJoy rosalesNessuna valutazione finora
- Neri NCP 1Documento4 pagineNeri NCP 1Emmanuel_Neri_3662Nessuna valutazione finora
- Health Examination RecordDocumento4 pagineHealth Examination Recordmary joy dela cruzNessuna valutazione finora
- 1-General ExaminationDocumento5 pagine1-General Examinationalmatrim10Nessuna valutazione finora
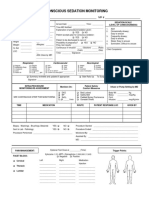
- 34 An Consious Sedation MonitoringDocumento2 pagine34 An Consious Sedation Monitoringabu alauon abed almohsenNessuna valutazione finora
- EKONSULTA FormDocumento13 pagineEKONSULTA FormJirhana Lindagan Karon-KampangNessuna valutazione finora
- 05 Nursing Note SampleDocumento3 pagine05 Nursing Note Sampletesttest testNessuna valutazione finora
- Health Screening and Assessment Form - SampleDocumento3 pagineHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- Intake and OutputDocumento3 pagineIntake and Outputtina100% (1)
- Post Anaesthesia Recovery ScoreDocumento2 paginePost Anaesthesia Recovery ScoreRaviraj Pishe50% (2)
- Post Anaesthesia Recovery Score PDFDocumento2 paginePost Anaesthesia Recovery Score PDFBombay Hospital100% (1)
- Acute SinusitisDocumento7 pagineAcute SinusitisNader SmadiNessuna valutazione finora
- Management of Diabetes: DR Rukman Mecca M I 51 ST Batch Calicut Med CollegeDocumento47 pagineManagement of Diabetes: DR Rukman Mecca M I 51 ST Batch Calicut Med CollegeRukman MeccaNessuna valutazione finora
- My Top Resources (Summer 08) Adult StammeringDocumento1 paginaMy Top Resources (Summer 08) Adult StammeringSpeech & Language Therapy in PracticeNessuna valutazione finora
- Nclex PNDocumento416 pagineNclex PNSandhu Sdhu100% (9)
- How and When To Be Your Own Doctor by Moser, IsabelDocumento135 pagineHow and When To Be Your Own Doctor by Moser, IsabelGutenberg.org100% (2)
- Jill Getchell, BS, CCP, LCP, LPNDocumento115 pagineJill Getchell, BS, CCP, LCP, LPNapi-301270014Nessuna valutazione finora
- How Black Salve Is Being Used To Treat Skin Cancer in The 21st CenturyDocumento57 pagineHow Black Salve Is Being Used To Treat Skin Cancer in The 21st CenturyBoddhi SattvaNessuna valutazione finora
- Neonatal Polycythemia: Is Partial Exchange Transfusion Justified?Documento9 pagineNeonatal Polycythemia: Is Partial Exchange Transfusion Justified?Lulú PérezNessuna valutazione finora
- GlomerulonephritisDocumento35 pagineGlomerulonephritisapi-19916399Nessuna valutazione finora
- The House Tree and Person TestDocumento10 pagineThe House Tree and Person TestRidaNessuna valutazione finora
- Psychiatric MisadventuresDocumento10 paginePsychiatric MisadventuresRob_212Nessuna valutazione finora
- HERNIIDocumento4 pagineHERNIISeceleanu MarianNessuna valutazione finora
- ACLS Study GuideDocumento30 pagineACLS Study GuidemmmmzNessuna valutazione finora
- Pulp Vitality TestDocumento3 paginePulp Vitality TestAbhinandan KatageriNessuna valutazione finora
- Pricelist Treatment Larissa CilacapDocumento11 paginePricelist Treatment Larissa CilacapFitra BagasNessuna valutazione finora
- Aprv Power PointDocumento96 pagineAprv Power PointAndi HidayatNessuna valutazione finora
- InjectomatTivaAgilia PDFDocumento2 pagineInjectomatTivaAgilia PDFBagas AnggerNessuna valutazione finora
- OctreotideDocumento4 pagineOctreotideMihaela VișanNessuna valutazione finora
- Oxygen InsufficiencyDocumento24 pagineOxygen InsufficiencyAnusha VergheseNessuna valutazione finora
- Acupuncture For Body 1 10Documento10 pagineAcupuncture For Body 1 10mamun310% (1)
- Soc CardiogenDocumento11 pagineSoc CardiogenOlga HMNessuna valutazione finora
- FootDocumento59 pagineFootAnmar Hamid Abd AlmageedNessuna valutazione finora
- Exam in MS1 Cope 2nd ExamDocumento5 pagineExam in MS1 Cope 2nd ExamIbrahim RegachoNessuna valutazione finora
- ReserarchDocumento4 pagineReserarchapi-287181456Nessuna valutazione finora
- Rebuilding The CommunityDocumento2 pagineRebuilding The CommunityMohammed SameerNessuna valutazione finora
- Medical Acupuncture: A Practical GuideDocumento20 pagineMedical Acupuncture: A Practical Guidegiovanna2004100% (2)
- Anti AcidsDocumento8 pagineAnti AcidsMohammad Ali Abu Ma'ashNessuna valutazione finora
- Kapapa 2009Documento10 pagineKapapa 2009iwanNessuna valutazione finora
- 9 Intravenous TherapyDocumento23 pagine9 Intravenous TherapyKareem Mae Pines RaborNessuna valutazione finora