Potrebbero piacerti anche
- How To Perform LeopoldDocumento5 pagineHow To Perform LeopoldChared Lumba100% (3)
- Leopold's ManeuversDocumento5 pagineLeopold's ManeuversUri Perez MontedeRamos100% (2)
- Leopolds and FetalDocumento7 pagineLeopolds and Fetaltyche100% (1)
- Leopolds ManueverDocumento5 pagineLeopolds ManueverRuby Dela RamaNessuna valutazione finora
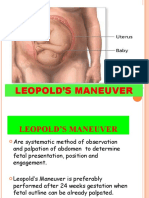
- Are Four Specific Steps in Palpating The Uterus Through The Abdomen in Order To Determine The Lie and Presentation of The FetusDocumento2 pagineAre Four Specific Steps in Palpating The Uterus Through The Abdomen in Order To Determine The Lie and Presentation of The FetusMoiraMaeBeridoBalite100% (3)
- Leopold's ManeuverDocumento22 pagineLeopold's ManeuverArlene Cerdeña Salceda100% (1)
- Leopold's Maneuver Hand OutDocumento2 pagineLeopold's Maneuver Hand OutRain Marquez100% (2)
- 10 Leopold's ManeuverDocumento5 pagine10 Leopold's ManeuverKrizia R. Pingke83% (6)
- Purpose:: Procedure: Rationale: Introduce Yourself and Inform Pregnant Woman About The ProcedureDocumento5 paginePurpose:: Procedure: Rationale: Introduce Yourself and Inform Pregnant Woman About The ProcedureArmySapphireNessuna valutazione finora
- Leopold's ManeuverDocumento2 pagineLeopold's ManeuverAnnaAlfonsoNessuna valutazione finora
- Done LEOPOLDS MANEUVER MONICITDocumento2 pagineDone LEOPOLDS MANEUVER MONICITMoiraMaeBeridoBaliteNessuna valutazione finora
- Leopold's ManeuversDocumento38 pagineLeopold's ManeuversGracy Morada Cu67% (6)
- Leopold's ManeuverDocumento2 pagineLeopold's ManeuverDeanne Stephanie Hordista100% (4)
- Leopold's ManeuverDocumento9 pagineLeopold's ManeuverAmiel Francisco Reyes100% (1)
- Leopold ManeuverDocumento4 pagineLeopold ManeuverElle100% (1)
- Leopold's Maneuver - Systematic Method for Fetal PresentationDocumento2 pagineLeopold's Maneuver - Systematic Method for Fetal PresentationPJ AmolarNessuna valutazione finora
- Problems With The PassagewayDocumento43 pagineProblems With The PassagewayMathew Beniga Gaco92% (12)
- NCM 109N: Frameworks For Maternal & Child Health NursingDocumento37 pagineNCM 109N: Frameworks For Maternal & Child Health NursingZudotaNessuna valutazione finora
- Nursing Care for High-Risk Labor and DeliveryDocumento170 pagineNursing Care for High-Risk Labor and DeliveryLongyapon Sheena Stephanie100% (2)
- 4 Core Steps of Essential Newborn CareDocumento2 pagine4 Core Steps of Essential Newborn CareAl Ronald Vincent Marcelo81% (16)
- Incompetent Cervix Case Analysis Subgroup 2Documento44 pagineIncompetent Cervix Case Analysis Subgroup 2bunso padillaNessuna valutazione finora
- 1st Topic Leopold ManeuverDocumento5 pagine1st Topic Leopold ManeuverNICOLE ANNE MARBELLA100% (1)
- Essential Intrapartum and Newborn CareDocumento160 pagineEssential Intrapartum and Newborn CareJohn Alwyn Hernandez100% (1)
- Problems of The PassengerDocumento9 pagineProblems of The PassengerDanah Grace SanchezNessuna valutazione finora
- Incompetent CervixDocumento4 pagineIncompetent CervixCharm Arroyo100% (1)
- Incompetent CervixDocumento29 pagineIncompetent CervixCyrelle Jen TorresNessuna valutazione finora
- Leopolds ManueverDocumento9 pagineLeopolds ManueverJonah R. Merano100% (3)
- Einc ReviewerDocumento4 pagineEinc ReviewerEricson Candelaria0% (1)
- Internal Examination: Prepared By: Lester D. Bongabong BSN Ii - BDocumento9 pagineInternal Examination: Prepared By: Lester D. Bongabong BSN Ii - BJustine Cagatan100% (1)
- Partograph: Jillian A. Bejoc, MSN, RNDocumento44 paginePartograph: Jillian A. Bejoc, MSN, RNJiezl Abellano AfinidadNessuna valutazione finora
- UNANG YAKAPDocumento3 pagineUNANG YAKAPBernadeth Labrador100% (1)
- Physical Examination For OBDocumento63 paginePhysical Examination For OBQuolette Constante87% (77)
- Care of The Mother and The Fetus During The Perinatal PeriodDocumento22 pagineCare of The Mother and The Fetus During The Perinatal PeriodRoshin Tejero100% (1)
- Leopold's Maneuver SkillsDocumento4 pagineLeopold's Maneuver SkillsCameron De Guzman100% (1)
- Complications With The Power of LaborDocumento8 pagineComplications With The Power of LaborEdrea Aquino MendezNessuna valutazione finora
- OB - Leopold's ManeuverDocumento2 pagineOB - Leopold's ManeuverRalph Alfonse De Jesus50% (2)
- Stages of LaborDocumento23 pagineStages of LaborPortia Dulce Toquero100% (5)
- Assessment in PregnancyDocumento15 pagineAssessment in PregnancyAna75% (4)
- Rubric For Performing Fundal Height MeasurementDocumento5 pagineRubric For Performing Fundal Height MeasurementPATRICIA JULIANNE CASTAÑETO RIVERANessuna valutazione finora
- Goals of Prenatal CareDocumento16 pagineGoals of Prenatal CareLhea Marie Trinidad100% (1)
- Notes On Obstetrics: Normal Labor (Theories of Labor Onset)Documento22 pagineNotes On Obstetrics: Normal Labor (Theories of Labor Onset)Jobelle Acena100% (1)
- Concept of unitive and procreative healthDocumento5 pagineConcept of unitive and procreative healthDONITA DALUMPINESNessuna valutazione finora
- 9 Labor and DeliveryDocumento6 pagine9 Labor and DeliveryUri Perez MontedeRamosNessuna valutazione finora
- Midterm Notes On NCM 109 EditedDocumento10 pagineMidterm Notes On NCM 109 EditedJohn Fred100% (2)
- Ballard Score: Neuromuscular Maturity 1. PostureDocumento14 pagineBallard Score: Neuromuscular Maturity 1. PostureFelix Wafula Musibi100% (2)
- Hospital Case Study 2nd Sem.Documento22 pagineHospital Case Study 2nd Sem.Salvador V Quindipan JrNessuna valutazione finora
- Uterine RuptureDocumento19 pagineUterine RuptureAna Denise Quinajon0% (1)
- Gestational AgeDocumento6 pagineGestational AgemhuniswellNessuna valutazione finora
- HEALTH STATISTICS and EPIDEMIOLOGYDocumento11 pagineHEALTH STATISTICS and EPIDEMIOLOGYarianNessuna valutazione finora
- Fetal DistressDocumento4 pagineFetal DistressAmira Attya100% (7)
- Unang Yakap DOH EINCDocumento20 pagineUnang Yakap DOH EINCLore Anne Mhae Santos100% (1)
- Our Daily Bread - LEOPOLDDocumento4 pagineOur Daily Bread - LEOPOLDJonas Marvin AnaqueNessuna valutazione finora
- Leopold's Maneuvers: Assessing Fetal PositionDocumento6 pagineLeopold's Maneuvers: Assessing Fetal PositionJoeyca Shien PiolNessuna valutazione finora
- DocumentsDocumento22 pagineDocumentsDivina D Galvez-BeronioNessuna valutazione finora
- Leopold's Maneuver.2Documento23 pagineLeopold's Maneuver.2Ces Aria100% (1)
- LEOPOLD's MANEUVER RATIONALEDocumento3 pagineLEOPOLD's MANEUVER RATIONALEAngela AquisapNessuna valutazione finora
- Leopods ManeuverDocumento8 pagineLeopods ManeuverDaryl Adrian RecaidoNessuna valutazione finora
- Leopold's maneuvers determine fetal positionDocumento39 pagineLeopold's maneuvers determine fetal positionJayrelle D. SafranNessuna valutazione finora
- LeopoldooDocumento7 pagineLeopoldooAmanda Aldilla MeutiadiNessuna valutazione finora
- Leopold's Maneuver GuideDocumento2 pagineLeopold's Maneuver GuideMoiraMaeBeridoBaliteNessuna valutazione finora
- Professional Adjustment: A ReviewDocumento41 pagineProfessional Adjustment: A Reviewjava_biscocho1229100% (3)
- A (H1N1) Vaccine: Questions AnsweredDocumento6 pagineA (H1N1) Vaccine: Questions Answeredjava_biscocho1229Nessuna valutazione finora
- Leprosy: A Case PresentationDocumento36 pagineLeprosy: A Case Presentationjava_biscocho122970% (10)
- ARTS: Aliswag Review and Training Specialists, IncDocumento23 pagineARTS: Aliswag Review and Training Specialists, Incjava_biscocho1229Nessuna valutazione finora
- OUR WORLD-North AmericaDocumento46 pagineOUR WORLD-North Americajava_biscocho1229Nessuna valutazione finora
- NCP-Effective Breast FeedingDocumento3 pagineNCP-Effective Breast Feedingjava_biscocho12290% (1)
- NCP Nutrition1Documento4 pagineNCP Nutrition1java_biscocho1229100% (1)
- Bronchial Asthma: A Case PresentationDocumento59 pagineBronchial Asthma: A Case Presentationjava_biscocho122985% (39)
- Pharmacology: A ReviewDocumento26 paginePharmacology: A Reviewjava_biscocho122988% (8)
- NCP-Ineffective AirwayDocumento5 pagineNCP-Ineffective Airwayjava_biscocho1229Nessuna valutazione finora
- Nursing Abbreviations, Prefixes and SuffixesDocumento10 pagineNursing Abbreviations, Prefixes and Suffixesjava_biscocho1229100% (4)
- History of Nursing-An OverviewDocumento5 pagineHistory of Nursing-An Overviewjava_biscocho1229100% (3)
- NCP Pain1Documento4 pagineNCP Pain1java_biscocho12290% (1)
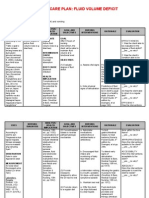
- NCP-Fluid Volume DeficitDocumento2 pagineNCP-Fluid Volume Deficitjava_biscocho122979% (33)
- Anatomy and Physiology-A ReviewDocumento38 pagineAnatomy and Physiology-A Reviewjava_biscocho1229100% (4)
- Eucharistic CelebrationDocumento40 pagineEucharistic Celebrationjava_biscocho12290% (1)
- As A Future NurseDocumento1 paginaAs A Future Nursejava_biscocho1229Nessuna valutazione finora
- Integrated Management of Childhood IllnessDocumento83 pagineIntegrated Management of Childhood Illnessjava_biscocho1229Nessuna valutazione finora
- Herbal Medicines in The PhilippinesDocumento20 pagineHerbal Medicines in The Philippinesjava_biscocho122997% (33)
- TunnelDocumento2 pagineTunneljava_biscocho1229Nessuna valutazione finora
- The Language of AnatomyDocumento4 pagineThe Language of Anatomyjava_biscocho122950% (2)
- Reviewer - Life of Dr. Jose RizalDocumento35 pagineReviewer - Life of Dr. Jose Rizaljava_biscocho122993% (105)
- Water and Landforms in The PhilippinesDocumento15 pagineWater and Landforms in The Philippinesjava_biscocho122988% (48)
- Mental Defense MechanismsDocumento2 pagineMental Defense Mechanismsjava_biscocho1229100% (2)
- Nursing Core Competencies For Quality LevelDocumento5 pagineNursing Core Competencies For Quality Leveljava_biscocho1229Nessuna valutazione finora
- Nursing Theories and Conceptual FrameworkDocumento3 pagineNursing Theories and Conceptual Frameworkjava_biscocho1229100% (3)
- Script For Leopold's Maneuver (Autorecovered)Documento3 pagineScript For Leopold's Maneuver (Autorecovered)lea mae andoloyNessuna valutazione finora
- Induced Abortion: Dr. Ali Murad Dr. Wassan NoriDocumento12 pagineInduced Abortion: Dr. Ali Murad Dr. Wassan NoriAmmarNessuna valutazione finora
- Evolution of Human Skin ColorDocumento11 pagineEvolution of Human Skin ColorTrinity ChampionNessuna valutazione finora
- Velez College - College of NursingDocumento4 pagineVelez College - College of NursingToni Angelie CaprechoNessuna valutazione finora
- Subrata Day - Genetics and Etiology of Down Syndrome (2011, Intech)Documento340 pagineSubrata Day - Genetics and Etiology of Down Syndrome (2011, Intech)EMI URSANNessuna valutazione finora
- Human SexualityDocumento11 pagineHuman Sexualitylanilyn aquinoNessuna valutazione finora
- Benemile Leopolds-ManeuverDocumento15 pagineBenemile Leopolds-ManeuverIsabelle Hazel BenemileNessuna valutazione finora
- Ruptured Corpus Luteum During Early PregnancyDocumento17 pagineRuptured Corpus Luteum During Early PregnancyityNessuna valutazione finora
- Essential Revision Notes For Part 2 MrcoDocumento27 pagineEssential Revision Notes For Part 2 MrcotahzeemtarakhanNessuna valutazione finora
- Consentimiento Informado RCOG 2015Documento13 pagineConsentimiento Informado RCOG 2015Paola RoigNessuna valutazione finora
- Antenatal Examination According To WHODocumento6 pagineAntenatal Examination According To WHOManisha ThakurNessuna valutazione finora
- Reproductive System Grade 7Documento5 pagineReproductive System Grade 7Valentina NapitupuluNessuna valutazione finora
- Health10 - q2 - Mod1 - Reproductive Health Laws - Version3Documento22 pagineHealth10 - q2 - Mod1 - Reproductive Health Laws - Version3Avril100% (2)
- Lec.23 Congenital Abnormalities of Female Genital OrgansDocumento5 pagineLec.23 Congenital Abnormalities of Female Genital Organsشريف محمد حسين شريف يوسفNessuna valutazione finora
- Abnormal Labor: Dystocia and Its CausesDocumento51 pagineAbnormal Labor: Dystocia and Its CausesMa. Bernadette PinedaNessuna valutazione finora
- Multiple PregnancyDocumento20 pagineMultiple PregnancySelma FraNessuna valutazione finora
- Week 13 Care of Mother, ChildDocumento27 pagineWeek 13 Care of Mother, ChildAnthonet AtractivoNessuna valutazione finora
- Clinic SchedDocumento3 pagineClinic SchedMyra MalabaguioNessuna valutazione finora
- Uterine InversionDocumento15 pagineUterine InversionMaggie Huatea Schnittka50% (2)
- Sexual SelfDocumento13 pagineSexual SelfANNE MARIE SANCHEZ100% (1)
- Text GasmDocumento18 pagineText GasmMervin Imhotep Accouche71% (7)
- Intercourse and IslamDocumento52 pagineIntercourse and IslamEngr. Khandaker Marsus75% (4)
- Tmbool's Notes in Obstetrics and Gynecology PDFDocumento113 pagineTmbool's Notes in Obstetrics and Gynecology PDFOsman SomiNessuna valutazione finora
- Management of Miscarriage 2016 PDFDocumento16 pagineManagement of Miscarriage 2016 PDFJLan JoNessuna valutazione finora
- Relly Yanuari Primariawan, DR., SpOG (K) - Kenapa Penting Terapi Post Op Endometriosis-1Documento38 pagineRelly Yanuari Primariawan, DR., SpOG (K) - Kenapa Penting Terapi Post Op Endometriosis-1oktavianusNessuna valutazione finora
- Desordenes Del Desarrollo Sexual Copia 2Documento16 pagineDesordenes Del Desarrollo Sexual Copia 2mariakjaimesNessuna valutazione finora
- Joshi Abhishek F.Y.P.B.B.SC - Nursing Govt College of Nursing JamnagarDocumento49 pagineJoshi Abhishek F.Y.P.B.B.SC - Nursing Govt College of Nursing JamnagarPoonam RanaNessuna valutazione finora
- Mother Zen by Jacinta Tynan - Chapter SamplerDocumento32 pagineMother Zen by Jacinta Tynan - Chapter SamplerHarlequinAustraliaNessuna valutazione finora
- Management of Reproductive Health and DysmenorrheaDocumento33 pagineManagement of Reproductive Health and DysmenorrheaIntan Permatasari Putri SNessuna valutazione finora
- Management of LabourDocumento38 pagineManagement of LabourAnjali Rahul AjmeriNessuna valutazione finora