Potrebbero piacerti anche
- Hip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHip Neck Fracture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionDa EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionNessuna valutazione finora
- Bone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsDa EverandBone Marrow Aspirate Concentrate and Expanded Stem Cell Applications in OrthopaedicsNessuna valutazione finora
- Advances in Cattle WelfareDa EverandAdvances in Cattle WelfareCassandra TuckerNessuna valutazione finora
- Soft Tissue Balance KneeDocumento10 pagineSoft Tissue Balance KneeNitin BansalNessuna valutazione finora
- Forensic Clinical Photography: A Game Changer in Medicolegal InvestigationDocumento6 pagineForensic Clinical Photography: A Game Changer in Medicolegal InvestigationFelicia HalimNessuna valutazione finora
- Early Embryological Development: Oral Histology Dent 206 DR Ashraf ShaweeshDocumento26 pagineEarly Embryological Development: Oral Histology Dent 206 DR Ashraf ShaweeshAbod NaserNessuna valutazione finora
- Lect11-Facial Nerve (CNVII)Documento17 pagineLect11-Facial Nerve (CNVII)Nayela AkramNessuna valutazione finora
- Jaw Relation GuideDocumento80 pagineJaw Relation Guidesamar yousif mohamedNessuna valutazione finora
- Total Knee ReplacementDocumento99 pagineTotal Knee ReplacementGandis Ayu WardaniNessuna valutazione finora
- NATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideDa EverandNATIONAL OPTOMETRY BOARDS (NOB) Part I BASIC SCIENCE: Passbooks Study GuideNessuna valutazione finora
- Interprofessional Rehabilitation: A Person-Centred ApproachDa EverandInterprofessional Rehabilitation: A Person-Centred ApproachSarah G. DeanNessuna valutazione finora
- A New Approach to Teaching and Learning Anatomy: Objectives and Learning ActivitiesDa EverandA New Approach to Teaching and Learning Anatomy: Objectives and Learning ActivitiesNessuna valutazione finora
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideDa EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideNessuna valutazione finora
- Prosthetic TreatmentDocumento23 pagineProsthetic Treatmenttristiarina0% (1)
- Medical Rehabilitation in Compression FractureDocumento32 pagineMedical Rehabilitation in Compression FracturegloriaNessuna valutazione finora
- DR Ashwani Panchal Jss Medical College MysoreDocumento94 pagineDR Ashwani Panchal Jss Medical College MysoreAravind RvndNessuna valutazione finora
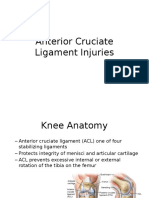
- Anterior Cruciate Ligament InjuriesDocumento16 pagineAnterior Cruciate Ligament InjuriesAlmas PrawotoNessuna valutazione finora
- Bone bank: Low antigenicity graftsDocumento2 pagineBone bank: Low antigenicity graftsMd Ahsanuzzaman PinkuNessuna valutazione finora
- Difference Between Typical and Atypical VertebraeDocumento2 pagineDifference Between Typical and Atypical VertebraeNIRANJANA SHALININessuna valutazione finora
- Varish TMJ Disorders WcaDocumento68 pagineVarish TMJ Disorders WcaFernando Delgado100% (1)
- Good Morning To ALLDocumento144 pagineGood Morning To ALLvinay agarwal100% (1)
- Knee ExaminationDocumento16 pagineKnee Examinationckyew64Nessuna valutazione finora
- Thesis TopicDocumento5 pagineThesis TopicSrikant KonchadaNessuna valutazione finora
- ActivatorDocumento69 pagineActivatorParijat Chakraborty PJNessuna valutazione finora
- Histology of BoneDocumento20 pagineHistology of Boneyudha anantha khaerul putraNessuna valutazione finora
- Facial Nerve & Trigeminal NerveDocumento25 pagineFacial Nerve & Trigeminal NerveRafiur RahmanNessuna valutazione finora
- Achilles TendonDocumento30 pagineAchilles TendonMeldianaNessuna valutazione finora
- All Papers Topic WiseDocumento55 pagineAll Papers Topic WiseZ TariqNessuna valutazione finora
- The Occlusal Splint TherapyDocumento5 pagineThe Occlusal Splint TherapyVíctor Adolfo Ravelo SalinasNessuna valutazione finora
- Joan Edelstein - Alex Moroz - Lower-Limb Prosthetics and Orthotics - Clinical Concepts-SLACK, Incorporated (2010)Documento215 pagineJoan Edelstein - Alex Moroz - Lower-Limb Prosthetics and Orthotics - Clinical Concepts-SLACK, Incorporated (2010)Andrei ȚîrleaNessuna valutazione finora
- Head and Neck Arterial SystemDocumento30 pagineHead and Neck Arterial SystemArifa parveenNessuna valutazione finora
- Management of Special ChildDocumento110 pagineManagement of Special ChildRisana RahoofNessuna valutazione finora
- Basics of Orthopedic RadiologyDocumento48 pagineBasics of Orthopedic RadiologySuganya BalachandranNessuna valutazione finora
- Cementum (B. K. Berkovitz, Oral Anatomy, Histology & Embryology, 3rd Edition)Documento12 pagineCementum (B. K. Berkovitz, Oral Anatomy, Histology & Embryology, 3rd Edition)Drsumit BahlNessuna valutazione finora
- Oral Anatomy & Physiology TestDocumento34 pagineOral Anatomy & Physiology TestEliza EllieNessuna valutazione finora
- Muscles of MasticationDocumento200 pagineMuscles of MasticationzinniaNessuna valutazione finora
- Seminar Space MaintainersDocumento84 pagineSeminar Space MaintainersStranger DNessuna valutazione finora
- Introduction To Dental Anatomy (Dental Anatomy, Physiology and Occlusion) Part 3Documento1 paginaIntroduction To Dental Anatomy (Dental Anatomy, Physiology and Occlusion) Part 3Hicham KarrouchiNessuna valutazione finora
- Articulators ProsthoDocumento91 pagineArticulators ProsthoFourthMolar.com0% (1)
- 香港脊醫 Hong Kong Chiropractors Sep 2016Documento6 pagine香港脊醫 Hong Kong Chiropractors Sep 2016CDAHKNessuna valutazione finora
- Fundamentals of Occlusion and RestorativeDocumento9 pagineFundamentals of Occlusion and RestorativePhạm Văn KhoaNessuna valutazione finora
- Lecture 2 BoneDocumento22 pagineLecture 2 BoneiamkpvemuriNessuna valutazione finora
- Practical Orthopedic Examination Made Easy JP Medi 5a053bc81723dd0336da5c77Documento13 paginePractical Orthopedic Examination Made Easy JP Medi 5a053bc81723dd0336da5c77Zed HarrisNessuna valutazione finora
- Fractures in the Elderly: Types, Causes and TreatmentsDocumento27 pagineFractures in the Elderly: Types, Causes and TreatmentshazelelNessuna valutazione finora
- Pleural EffusionDocumento78 paginePleural EffusionJessa AdenigNessuna valutazione finora
- Implants and Anchorage / Orthodontic Courses by Indian Dental AcademyDocumento52 pagineImplants and Anchorage / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Simplex Cement Combined BrochureDocumento13 pagineSimplex Cement Combined BrochureICNessuna valutazione finora
- Muscles of Mastication: - DR - Asif Iqbal - 2 Year P.GDocumento85 pagineMuscles of Mastication: - DR - Asif Iqbal - 2 Year P.GSaghar AbroNessuna valutazione finora
- A History of PhysiotherapyDocumento5 pagineA History of Physiotherapyjakewilliams925Nessuna valutazione finora
- Limb Length Discrepancy: Presenter - Dr. MadhukarDocumento62 pagineLimb Length Discrepancy: Presenter - Dr. MadhukarAnil SoodNessuna valutazione finora
- 6-Fractures and Joints Dislocations ManagementDocumento91 pagine6-Fractures and Joints Dislocations ManagementMUGISHA GratienNessuna valutazione finora
- Técnica MillardDocumento10 pagineTécnica MillardMarcoNessuna valutazione finora
- HIP JOINT Special Tests-WPS OfficeDocumento51 pagineHIP JOINT Special Tests-WPS OfficeManisha MishraNessuna valutazione finora
- SM 10 - Knee Lesson 1Documento4 pagineSM 10 - Knee Lesson 1api-383568582Nessuna valutazione finora
- Lifestyle PDFDocumento19 pagineLifestyle PDFManish RajNessuna valutazione finora
- Orthopedo AssDocumento4 pagineOrthopedo AssIvyRoselleLacasandileCabañeroNessuna valutazione finora
- GROWTH ASSESSMENT METHODSDocumento65 pagineGROWTH ASSESSMENT METHODSdr parveen bathlaNessuna valutazione finora
- Easy Way To Learn ABGsDocumento13 pagineEasy Way To Learn ABGsMunaim TahirNessuna valutazione finora
- Patient RightsDocumento14 paginePatient RightsFarhan ShahidNessuna valutazione finora
- Ligament & Muscle InjuriesDocumento2 pagineLigament & Muscle InjuriesFarhan Shahid100% (1)
- Bone TumoursDocumento4 pagineBone TumoursFarhan ShahidNessuna valutazione finora
- Acute OsteomyelitisDocumento3 pagineAcute OsteomyelitisFarhan ShahidNessuna valutazione finora
- Peripheral Nerve InjuriesDocumento2 paginePeripheral Nerve InjuriesFarhan ShahidNessuna valutazione finora
- MeningitisDocumento61 pagineMeningitisFarhan ShahidNessuna valutazione finora
- Effect of Static Knee Joint Flexion On Vastus Medialis Obliquus Fiber Angle in Patellofemoral Pain Syndrome - An Ultrasonographic StudyDocumento9 pagineEffect of Static Knee Joint Flexion On Vastus Medialis Obliquus Fiber Angle in Patellofemoral Pain Syndrome - An Ultrasonographic Studycris weeNessuna valutazione finora
- Fraktur Clavicula DextraDocumento28 pagineFraktur Clavicula DextraRaisah_Ridwan382Nessuna valutazione finora
- Total Knee Arthroplasty - A Comprehensive Guide (PDFDrive)Documento278 pagineTotal Knee Arthroplasty - A Comprehensive Guide (PDFDrive)Brain AngganaNessuna valutazione finora
- Arthrorehab Course Info 2023Documento14 pagineArthrorehab Course Info 2023Braina The oneNessuna valutazione finora
- Throwers TenDocumento11 pagineThrowers TenRui CunhaNessuna valutazione finora
- 7 Minute Rotator Cuff SolutionDocumento113 pagine7 Minute Rotator Cuff Solutioninstanoodles100% (6)
- Chondromalacia Patella: Causes, Tests, and Physical Therapy TreatmentsDocumento10 pagineChondromalacia Patella: Causes, Tests, and Physical Therapy TreatmentsAfifah NurNessuna valutazione finora
- Lesi MeniskusDocumento115 pagineLesi MeniskusHanif AhmadNessuna valutazione finora
- Biomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KDocumento46 pagineBiomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KGio BalisiNessuna valutazione finora
- Burrows and Moreton Prize0Documento4 pagineBurrows and Moreton Prize03nhu1100% (1)
- Physiotherapy MCQsDocumento12 paginePhysiotherapy MCQssurender_singh_4373% (11)
- Shoulder Rehabilitation Protocols PDFDocumento19 pagineShoulder Rehabilitation Protocols PDFCassie RodriguezNessuna valutazione finora
- Knee Injury Decision Tree FiguresDocumento1 paginaKnee Injury Decision Tree FigureslizNessuna valutazione finora
- Special Tests For WristDocumento13 pagineSpecial Tests For WristSaif Ahmed LariNessuna valutazione finora
- Dumbbell WorkoutsDocumento40 pagineDumbbell WorkoutsPrasanth Kurien Mathew100% (6)
- Pilates for Hip Joint Dysfunction: How Exercises Can Help RehabilitationDocumento14 paginePilates for Hip Joint Dysfunction: How Exercises Can Help RehabilitationHugo FigueroaNessuna valutazione finora
- Toribash MovesDocumento4 pagineToribash MovesJarrett StevensNessuna valutazione finora
- Common Cervical and Thoracic Counterstrain Tender PointsDocumento12 pagineCommon Cervical and Thoracic Counterstrain Tender PointsSafariDuckNessuna valutazione finora
- Chapter 8Documento40 pagineChapter 8s211151339Nessuna valutazione finora
- Lab 1 Anatomical Description Exs 397Documento10 pagineLab 1 Anatomical Description Exs 397api-476937064Nessuna valutazione finora
- Biomechanics of Elbow JointDocumento10 pagineBiomechanics of Elbow JointGeddam SnehalathaNessuna valutazione finora
- 6 Elbow MObilizationDocumento16 pagine6 Elbow MObilizationGautamNessuna valutazione finora
- Science Year 7 Cambridge Presentation Powerpoint Unit 1 Part 2Documento9 pagineScience Year 7 Cambridge Presentation Powerpoint Unit 1 Part 2ahmad sabryNessuna valutazione finora
- Upper Limb OrthosisDocumento83 pagineUpper Limb OrthosisAwaisNessuna valutazione finora
- TRX ® Hamstrings Curl: Step 1Documento13 pagineTRX ® Hamstrings Curl: Step 1Eric LemaireNessuna valutazione finora
- A Morphometric Study of Patella in Lucknow RegionDocumento10 pagineA Morphometric Study of Patella in Lucknow RegionIJAR JOURNALNessuna valutazione finora
- Meniscal Repair. Jaoos PDFDocumento10 pagineMeniscal Repair. Jaoos PDFkarenNessuna valutazione finora
- SCALE-Selective Control Assesment PDFDocumento3 pagineSCALE-Selective Control Assesment PDFjinil raj j.r.Nessuna valutazione finora
- 12 - Rehabilitation After Fractures of - 2018 - Clinical Orthopaedic Rehabilitat PDFDocumento7 pagine12 - Rehabilitation After Fractures of - 2018 - Clinical Orthopaedic Rehabilitat PDFTolo CantallopsNessuna valutazione finora
- Osteoarthritis Genu RehabilitationDocumento52 pagineOsteoarthritis Genu Rehabilitationwahyu_sitaNessuna valutazione finora