Life Science
Recent Innovations
Ca asel ae]
nt .
Breer eats i
Dr. Shaon Ray Chaudhuri
rece nee rat EI
Research Publication House
Dr. Shaon Ray Chaudhuri did her PhD (2001) from Department of
Biophysics, Molecular Biology and Genetics, Calcutta University
after finishing the bachelors (1994) and Masters (1996) in Physiology
from Calcutta University. She worked as DBT PDF in Life Sciences at
Jadaypur University (2001-2003). She received the young scientist
award under the DST fast track scheme in 2003 and continued to work
at Jadavpur University till she joined West Bengal University of
Technology on November 2004. She did post-doctoral training at Technical
University of Munich, Germany as well as Humboldt University, Berlin.
} Between November 2004 and August 2015 she setup the Microbial Technology
| ere renron eta neey orange Mer Tang Qe ticKOM satel enccr mma nce Tate tt
Technology and Management from Ministry of Human Resource and Development,
Cerone re OM aR Ct Menta it DSS MCs errs mE MRS epee TT pe Cari
| (Gro nee are lommeeroneU ye ter ae teecstrtn ee htmccace ni) Grate ON CN SASS
| has 46 papers while 10 book chapters. Five scholars have obtained their PhD, two
COU nee Tie AG Te Tot Team ETT Coote OS TaST Leyes (Ore Coes la eHectcemgnicle(ecs RCO}
submit their thesis in 2016 while four others are currently working in the group under
i her guidance. She has obtained extramural grants to the tune of Rs 5.828 Crores from
different granting agency {ill March 2016. She moved to Tripura University as
| PRS se ed uO Dragana Mem UN ec esy mer Mee scenes e) UTE
is instrumental in obtaining the first faculty grants for the department, signing of
MoU with industry and institutes as well as syllabus revision for the existing MSe
Coe h ie arue ones etsmcrsr pent ice reste tomes
ionensan
International
Research Publication House
Head Office: B-2/84, Ground Floor,
Rohini Sector-16, Delhi-110089, INDIA
Fax No.: +91-11-27297815
TeurrieenoChrss ite ckcory
Donia a mtn tetencon|
Published by
International Research Publication House
Head Office: B-2/84, Ground Floor,
Rohini Sector-16, Dethi-110089, INDIA
Fax No.: +91-11-27297815
Email: info@irphouse.com
Website: www.irphouse.com
© 2016 International Research Publication House
Printing of books passes through many stages - writing, composing,
proof reading, printing etc. We try our level best to make the book
error free. If any mistake has inadvertently crept in, we regret it and
would be deeply indebted to those who point it out. We do not take
any legal responsibility.
No part of this book may be reproduced, stored in any retrieval system
or transmitted in any form by any means ~ electronic, mechanical
photocopying, recording or otherwise without the prior written
permission of the Author and Publishers.
Book Proposal No.: 1403
ISBN: 978-93-84443-53-5
Price: Within India: Rs. 500
Outside India: US$ 25
‘Typeset by IRPH INFORMATION SERVICES
B-2/84, Ground Floor, Rohini Sector-16, Delhi-1 10089 INDIA
Printed in India
CONTENTS
Preface
Acknowledgement
ag earner
Chapter No//Title/Authors's Name Page No.
re
CHAPTER -1
RECENT ADVANCES IN CLINICAL ONCOLOGY 1-16
Radhashvee Maitra
CHAPTER -2
A GLIMPSE ON TUBERCULOSIS AND SCOPE OF INHALABLE ANTI 17-32
TUBERCULAR THERAPY
Vishnu Vardhan Reddy Beeram &Venkata Nadh Ratnakaram
CHAPTER -3
REACTIVE OXYGEN SPECIES: CHEMISTRY AND BIOLOGY 33-48
Timir B Samanta
CHAPTER -4
BIOFILMS AND ANTIMICROBIAL DRUG DISCOVERY 49-68
Sangeeta Raut
CHAPTER -5
AN UPDATE ON THE MICROBIOLOGICAL TECHNIQUES INVOLVE IN 69-79
DETECTION OF BIOFILM FORMATION
Purnita Bhattacharyya, Madhurankhi Goswami,
Bannhi Das, Shiny C. Thomas and Prosun Tribedi
CHAPTER -6
QUANTITATIVE CHARACTERIZATION OF SULPHATE REDUCTION DATA 81-102
OBTAINED FROM A BIOFILM BASED BIOREACTOR - PART-I
Indranil Mukherjee, Amal Giri, Chitrakalpa Sen,
Riga Sebait and Parthasarathi Barat
CHAPTER -7
QUANTITATIVE CHARACTERIZATION OF SULPHATE REDUCTION DATA 103-120
OBTAINED FROM A BIOFILM BASED BIOREACTOR - PART Il
Indranil Mukherjee, Amal Givi and Parthasarathi Barat
CHAPTER -8
UNDERSTANDING PLANT MICROBE INTERACTION ON THE LEAF 121-151
SURFACE
Sourav Ghosh; Livia Eliza Alex, Farha Khan, Jhumki Das,
Tethi Biswas, Sohini Basu, Pritam Basak, Ankita Nag,
Ashoke Ranjan Thakur, M. Sudarshan, Christian Ulrich,
Inga Mewis and Shaon Ray Chaudhuri
CHAPTER -9
COMPARISON OF THE RESPONSE OF ALBICANS AND NON ALBICANS —153-180
GROUP OF CANDIDA ISOLATED FROM DIFFERENT PARTS OF WEST
BENGAL, INDIA UPON EXPOSURE TO SEVERAL STRESSES
Anirban Mukherjee and Shaon Ray Chaudhuri
CHAPTER -10
EVALUATION OF THE EFFECTIVENESS OF PHYTOCHEMICALS AND ITS 181-199
COMBINATION WITH SYNTHETIC DRUGS AGAINST CANDIDA SPECIES
AND ITS SECRETED ASPARTYLE PROTEASE AS AN ALTERNATIVE
APPROACH TO ELIMINATE THE RESISTANT OPPORTUNISTIC YEAST
PATHOGENS ISOLATED FROM NATURAL RESERVOIR
Anirban Mukherjee
CHAPTER -11
ROLE OF MICRIOBAL AGENTS IN INSECT PEST MANAGEMENT 201-240
Showket Ahmad Dar, Sajad Husan Wani,
Shahid Ahmad Padder and Shahid A. Akber
CHAPTER -12
A POLYPHASIC APPROACH OF SPECIES IDENTIFICATION FOR GENUS 241-269
BACILLUS
Madhurima Ghosh, Amrita Saha, Kamlesh Jangid,
Amaraja Abhay Joshi and Shaon Ray Chaudhuri
CHAPTER -13
COMPARATIVE STRUCTURAL ANALYSIS OF SpoOF AND Spo0B LIKE
PROTEIN INVOLVED IN PHOSPHOTRANSFER PATHWAY IN New
Bacterial Species MCC0008
Sandhayaa S., Sujata Roy and Ashoke Ranjan Thakur
CHAPTER -14
PHOTOBACTERIUM LEIOGNATHI CMB_001: NEW-GENERATION OXYGEN
DETECTION BIOSENSOR FOR ENVIRONMENTAL QUALITY MONITORING.
Sourav Ghosh, Subhadeep Ghosh, Amrita Saha,
Ashoke Ranjan Thakur, Debabrata Datta,
Indranil Mukherjee, and Shaon Ray Chaudhuri
CHAPTER -15
COMPUTATIONAL TECHNIQUE FOR UNCERTAINTY ASSESSMENT OF
BIOKINETIC MODEL OF STRONTIUM
D. Datta
CHAPTER -16
‘THE CULTIVATION AND PEST MANAGEMENT OF RICE IN KASHMIR
Showket Ahmad Dar, Ghulam Mohmmad Mir,
Manzoor Ahmad Parry, Shahid Ahmad Padder
& Sajad Hussain Mir
CHAPTER -17
POTENTIAL OF PHEROMONE TECHNOLOGY IN THE MANAGEMENT OF
INSECT PESTS OF APPLE
Showket Ahmad Dar
CHAPTER -18
SUCCESSFUL TECHNOLOGY TRANSFER OF WASTE WATER FED
AQUACULTURE FROM INDIA TO BANGLADESH: A CASE STUDY
Sufia Khanam, Indranil Mukherjee, Ashoke Ranjan Thakur
and Shaon Ray Chaudhuri
271-286
287-299
301-321
323-349
351-363
365-382
CHAPTER - 2
A GLIMPSE ON TUBERCULOSIS AND SCOPE
OF INHALABLE ANTI TUBERCULAR
THERAPY
‘Vishnu Vardhan Reddy Beeram! and Venkata Nadh Ratnakaram2*
‘Pulse Advanced Research Centre, Nacharam, Hyderabad-500076, India,
E-mail: srivyshu.pharma@ gmail.com;
° GITAM University - Bengaluru Campus, Karnataka — 561203, India,
E-mail: doctornadh @ yahoo.co.in; Ph.No: +91-9902632733
Abstract
Tuberculosis (TB), is an airborne and notorious disease caused by
Mycobacterium tuberculosis. Despite the technological advances, the
tubercle bacillus continues to threaten humans. Most patients are
noncompliant towards current modes of treatment due to resistance of
bacilli for single or multiple drugs. The usual treatment duration ranges
from 6-9 months for drug susceptible TB; 18-24 months for multidrug
resistant TB. However the long term treatment posses adverse events. To
avoid the adverse events and improve the efficacy, alternative modes of
drug delivery systems are desired. Among them, the nanotechnology
overcomes the limitations of conventional therapy and improves the
efficacy. The nanocarriers can be considered for pulmonary application by
virtue of their potential advantages. However, nanoparticles meant for
lung delivery poses certain challenges such as difficulty in
characterization and the extent of utility towards practical applications. It
must be noted that the development of nanocarriers for pulmonary
application requires an in depth knowledge of the lung, both in its healthy
and disease state. Recent developments include in vitro models based on
cell line cultures. The present paper describes the development and
characterization aspects for inhalable drug delivery systems for the
targeted and slow delivery of antitubercular drugs.
Life Science: Recent Innovations & Research 18
Keywords: Tuberculosis, Mycobacterium tuberculosis, Drug delivery
systems, Inhalable drug delivery system, Targeted delivery, Anti-TB
drugs
INTRODUCTION
Hippocrates (460-377 BC) identified the process, phthisis (or consumption). It is
the process where the substance is completely destroyed and was the most
widespread and lethal disease of its time (Soled, 1991). The tubercular decay was
found in 3000 B.C in Egyptian mummies (Zink et al., 2003) and further evidence
that tuberculosis (TB) has accompanied mankind for a very long time. During the
18th and 19th centuries the disease ravaged Europe and North America earning
the nickname “Captain among these men of death”. The Europeans and Americans
during 18" and 19" centuries began to understand the pathophysiology of the
disease (Daniel, 2006). Robert Koch identified Mycobacterium tuberculosis as the
causative agent for TB in 1882 (Koch and Pinner, 1932). About 40 years later,
Albert Calmette and Camille Guerin had developed a vaccine (BCG) by serial
passage of the closely related species Mycobacterium bovis (Calmette, 1928).
About four new frontline anti TB-drugs (ATDs) were introduced during 1952-
1961, the drugs when used in combination has shown success rate of up to 87%
(Global Tuberculosis Report, 2012). Eventually the research on TB has grown and
at present, 11 new vaccines and several TB-drugs are available. Some drugs are in
clinical trials and under regulatory review. Despite the continual effort to develop
tools against the disease, about 9 million people are reported to have TB. About
1.5 million people were died due to TB, and among them 360,000 people were
HIV positive (Global Tuberculosis Report, 2012). Furthermore, it is estimated that
about one third of the world’s population is latently infected with TB (Enarson and
Ait-Khaled, 1996). The review describes the fundamentals of infection and its
development, inhalable drug delivery systems based on nanoparticles and their
characterization.
INITIAL INFECTION
The TB is an airborne disease, initially spread from the infected host by coughing
or sneezing in the form of droplets containing the bacilli upon inhalation (Turner
and Bothamley, 2015; Aliabadi et al., 2011; Tuberculosis fact sheet, 2012). The
bacilli reach the site of gas exchange, the alveoli, and a void being trapped in the
mucosal layers of the upper respiratory tract. The professional phagocytes,
alveolar macrophages engulf the bacilli (Dannenberg, 1993) (Fig-1) and prevent
the infection in general. However the bacilli dominate and spread the disease in
susceptible individual. There exists an involvement of diverse receptors for the
uptake of the bacteria that include Toll-like receptors (TLR), cluster of
differentiation 14 (CD14), complement, mannose, SPA and scavenger receptors.
ence: Recent Innovations & Research 19
tion, next target of bacilli include Fe receptors after onset of adaptive
anity (Emst, 1998; Dunne et al., 1994). It was believed that the macrophages
@ the engulfed bacilli into sub lying epithelial cells causing a local
=fammation (Ulrichs and Kaufmann, 2006). The inflammation eventually show
af towards the mononuclear cells from the nearest blood vessels, thus
ding a new environment of host cells for enhancing the bacterial population
s and Ramakrishnan, 2009) thus the disease is further expanded. The early
form the mucosa for eventually develop into tubercle or granuloma, the
mark structure of TB (Adams, 1976). Alternatively, the bacilli transported to
st lymph via dendritic cells (DC) for activation of the adaptive immune
-m (Wolf et al., 2007). It was believed that the lymphohematogenous route
the path for the establishment of secondary TB lesions (Cooper, 2009).
er form, miliary tuberculosis is lethal-as the mortality rate is high and it
mostly affects the young children and patients with immunodeficiency (Harries,
2004), is 30% even when treated (Hussain et al., 2004). However the prime
‘on of the infection in most of patients (80-85%) is the respiratory tissue
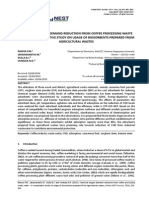
nand Zumla, 2011). The life cycle of Mycobacterium tuberculosis is shown
ure-1.
Oo
ok
a
RO
Figure 1- The life cycle of Mycobacterium tuberculosis showing the bacteria
uptake followed by granuloma formation, accumulation of necrotic cell and
granuloma rupture (David et al., 2009).
Life Science: Recent Innovations & Research 20
‘The occurrence of initial infection is as follows
Primary progressive TB: Forty percent of infections are associated with the
primary active TB, in which the immune system of the host is unable to destabilize
the bacilli (Parrish et al., 1998) (Fig-2). The initial infection gradually expands and
causes infections eventually results in complete destruction of the infected organ
(Harbitz, 1922). When the disease is left untreated, the mortality rate of
progressive TB is about 66% (Global Tuberculosis Report 2012).
Latent TB: The latent TB is a state of latency, a non transmissible form in which
clinical signs of disease are absent (Russell et al., 2010) and it persists in about
60% of cases, It is estimated that one third of the world’s population carry this
latent version of TB (Enarson and Ait-Khaled, 1996). The majority of patients live
their lives without ever knowing that they carry the disease. However some (2 to
23% lifetime risk) of them will experience the reactivation of the infection to
secondary active TB, The number of cases (5-10% annual risk) is relatively high
in the people with compromised immunity due to HIV/AIDS or the use of
immunosuppressant (Gedde-Dahl, 1952).
=
canes
Figure 2: Outcomes associated with exposure to Mycobacterium Tuberculosis
(Davies, 2001)
NOVEL AND MODIFIED RELEASE DELIVERY SYSTEMS
TB has been a leading killer disease globally and a multiple of first-line ATDs
must be administered regularly for at least 6 months to relieve the disease, The use
of antimycobacterials since decades is in practice. However the control with
hepatotoxicity,
he inadequate modes of dru;
challenge for drug delivery technolog;
formulation scientists (du Toit et al.,
mycobacterial chemotherapy is a tricky and arduous task
‘he therapy involves long term administration, (ii) poor permeability and thus less
ailability of antimycobacterial drugs at target site,
ccugs are highly toxic,
medicines is observed e:
the therapy associated
titubercular drugs
21
inly because (i)
(ii) all antimycobacterial
and (iv) significant patient noncompliance to prescribed
‘specially due to the length of the therapy and also due to
severe side effects. Numerous side effects are reported for
(Table 1 and 2). The dangerous side effects include
neurotoxicity and ocular toxicity. Most of the side effects are
ig administration and thus present a great
'y and for the scientific community including
2006). To overcome, the limitations of
conventional modes of drug delivery alternative modes of drug delivery systems
and their administration would be desired,
Table 1: Side effects of first line Antituberculosis drugs
Drug Major adverse effects Rare adverse effects
Peripheral neuropathy, skin rash, | Convulsions, psychosis,
Isoniazid " y
hepatitis, sleepiness and tethargy | arthralgia, anemia
Abdominal pain, nausea, vomiting, | Osteomalacia, pseudo-
: membranous colitis, pseudo-
/ hepatitis, generalized cutaneous
Rifampin adrenal crisis, severe renal
reactions, thrombocytopenic
stoppage, hemolytic blood
purpura P
paucity
Arthralgia, hepatitis,
ve | 8 i : ction, siderobla
Pyrazinamide | £88tintestinal problems.eg, Cutaneous reaction, sideroblastic
stomach upset, nausea, poor
appetite and abdominal pain
anemia
| Sweptomycin
Vestibular and auditory nerve
damage renal breakage, cutaneous
allergic reaction
Pain, rash at injection site,
numbness around the mouth and
tingling soon after the injection
| Thiacetazone
Skin rash that sometimes has
mucosal involvement
Liver failure, dermatological
disorders
Table 2: Side effects of second line Antituberculosis drugs
[Drug Major adverse effects Rare adverse effects
: Vestibular (vertigo) and . a
| Kanamycin anditorynemse aenee Cutaneous hypersensitivity
| Amikacin Vestibular damage (vertigo) | Cat renal failure
| and auditory nerve damage
| Capreomycin’ Nephrotoxicity
Life Science: Recent Innovations & Research 22
Gastrointestinal anorexia,
nausea, diarthea, abdominal
pain, hepatotoxicity
Ethionamide:
(prothionamide)
Convulsions, mental symptoms,
impotence, gynecomastia
Anxiety, dizziness, headache,
convulsions, rupture of the
Achilles tendon
Gastrointestinal anorexia,
Fluoroquinolones
nausea, vomiting
Dizziness, headache,
Cycloserine depression, psychosis,
convulsions
Suicide, generalized
hypersensitivity, hepatitis
Gastrointestinal anorexia,
Para amino salicylic | nausea, vomiting, Hypothyroidism, hematological
acid hypersensitivity reactions | reactions
(fever, rash, pruritus)
Nanotechnology is the promising technology and has been a boon to current
pharmacology and biopharmaceutical enhancement of drug performance. It is
possible to design drug delivery systems capable of targeting phagocytic cells that
are infected by intracellular pathogens, such as mycobacteria. The delivery
systems based on nanotechnology offer wide opportunities for improving therapy
efficacy for a wide range of diseases including TB (Fig-1). Therefore alternative
modes of delivery is required to develop the devices for the enhancement of
bioavailability and site specific targeting of first line ATD therapeutics to avoid
development of drug resistance (Schatz et al., 2005). The bioavailability can be
enhanced by bypassing the barriers that hinder the bioavailability. Diverse
approaches for the development of nanoparticles have been reported for the
exclusive delivery of chemotherapeutic agents to target sites. This helps in
improving the therapeutic index of the drug by stringently localizing its
pharmacological action to the target site or organ. Thus it may be said that the
nanoparticulate drug delivery systems help in improving the tolerance for toxic
chemotherapeutics a part from the bioavailability enhancement (Shegokar et al.,
2011)
INHALABLE DRUG DELIVERY
Lungs are an attractive target for the pulmonary administration of therapeutic
moieties in the form of various drug delivery systems (Azarmi et al., 2008; Jaafar-
Maalej et al., 2012). Additionally, the pulmonary route offers advantages over per
oral route that include high surface area with rapid absorption due to high
vascularization and avoidance of first pass effect (Sung et al., 2007). This
selectivity allows targeted drug delivery and, hence, reduces the side effects (Beck-
Broichsitter et al., 2009: Beck-Broichsitter et al., 2012). Colloidal drug delivery
systems have extensively been investigated as drug carrier systems for the
application of different drugs via different routes of administration. Solid lipid
Science: Recent Innovations & Research 23
particles (SLN) are one of the most interesting colloidal systems that have
ed for more than a decade ‘ (Mueller, 2000; Mueller, 2008)]. SLN are
scale suspensions composed of phospholipids and triglycerides with
ological tolerability (Morimoto et al., 2013; Nassimi et al., 2009). Apart from
\, biodegradable polymeric nanoparticles are also attaining importance due to
‘Se sustained release properties. The SLNs are ideal drug carriers for drugs with
poor aqueous solubility and high lipophilicity. The increased solubility in
pophilic matrix adds a positive effect in terms of improved pharmacokinetics and
cy. Nanoparticle based drug carriers open up new initiatives such as
mosification of physical properties. The parameters include enhancing drug
bility; drug loading capacity and surface modification to modulate the drug
selease behavior (Paranjpe et al., 2013; Menon et al., 2014). Certain nanosystems
So possess toxic effects apart from their therapeutic effects. The toxicological
testing of naoparticulate systems is necessary to assess the safety of nanoparticles
zing in vitro, ex vivo and in vivo cell culture models. The testing is essential to
assess the risk potential of nanoparticulate systems. The choice of the inhalation
ice in a specific patient population also plays a vital role in nanoparticle-
ediated drug delivery systems. Various parameters and their relationship shall be
considered in the development of nanoparticles as illustrated in Figure 3,
Figure 3: Additional details Figure 3: Complex interplay of parameters in
to support the utility of the research and development of pulmonary
nanoparticles in TB drug delivery systems.
Life Science: Recent Innovations & Research 24
a
Physicochemical Characterization
Particle size and charge measurements
Particle size and charge (zeta potential) measurements are important for the
characterization of nanoparticles in order to ensure the optimal particle size
distribution and polydispersity index (PDI). Photon correlation spectroscopy
(PCS) and laser diffraction (LD) are widely used method for the estimation of
Particle size. PCS measures the particles ranging from few nanometers to
maximum of 3 um, A beam of light is passed on the nanoparticles dispersion (Lim
et al., 2013). The scattered light from the nanoparticles is measured, amplified and
correlated to size. PCS can also measure the PDI, which determines the uniformity
of the particles. A higher value of PDI (50.2) normally indicates multiple sizes of
particles in the given formulation, thus smaller PDI is desirable for uniform
distribution of particles. The LD technique measures particles with a bigger size
and is based on the measurement of the diffraction angle depending on the particle
size. LD measures particles from the nanometer to a few millimeter size ranges
(Kelly, 2004; Tena and Clara, 2012). It is recommended to use both techniques
simultaneously. The zeta potential measurements are essential for understanding
the stability behavior. The high values of zeta potential contribute for repulsion
and make the particles to less aggregate. In addition, the uniform sized particles
show good stability,
Differential Scanning Calorimetry (DSC)
DSC is used to detect the polymorphic changes if any in the lipid matrix. The
structural changes in the lipid matrix provide information about the instability of
delivery system. Melting and recrystallization curves are appropriate parameters
to determine polymorphic changes of the lipids, Bunjes er al (2010; 2011) reported
the detailed analysis of the use of DSC in lipid-based systems.
X-ray diffraction
X-ray diffraction studies analyze the crystal structure in terms of spaces in the lipid
lattice. The presence of drug in lipid matrix influences the lipid/polymer structure
and thus the lattice spaces. The method can be used along with DSC, analyzes the
patterns of the spaces over time. Hence, both techniques are recommended to use
for the assessment of orsytalinitiy in lipid-based formulations (Bunjes, 2007).
Other techniques
More advanced methods, nuclear magnetic resonance (NMR), Raman
spectroscopy and infrared spectroscopy are used for physicochemical evaluation,
The techniques characterize specifically mixed systems associated with co-
existence of micelles, liposomes and liquid crystals.
L ‘ience: Recent Innovations & Research 25
Techniques for particle morphology
morphology of the nanoparticles can be examined by using transmission
ron microscopy utilizing different techniques suitable for specific particles.
fracture, negative staining and cryogenic-transmission methods can be
d according to the type of delivery system. The morphological
cmination is required to understand the structure, shape and alignment of the
cles (Bunjes, 2011).
Cell and animal based studies
ral studies are reported (Ehrhardt et al., 2004) for the toxicity assessment
lizing various models that include cell lines, tissue and animal models. Toxicity
dies are required to determine the lethal dose and the therapeutic window of the
-loaded nanocarriers. Studies to demonstrate the therapeutic efficacy have
-
Potrebbero piacerti anche
- Kinetics of Ruthenium (III) Catalysed and Uncatalysed Oxidation of Monoethanolamine by N-BromosuccinimideDocumento6 pagineKinetics of Ruthenium (III) Catalysed and Uncatalysed Oxidation of Monoethanolamine by N-BromosuccinimideHeidi HughesNessuna valutazione finora
- A Novel Reversed Phase Liquid Chromatographic Method For The Simultaneously Determination of Potential Impurities of Bisoprolol Fumarate and Hydrochlorothiazide in A Fixed Dosage FormDocumento31 pagineA Novel Reversed Phase Liquid Chromatographic Method For The Simultaneously Determination of Potential Impurities of Bisoprolol Fumarate and Hydrochlorothiazide in A Fixed Dosage FormHeidi HughesNessuna valutazione finora
- Shift of Reaction Pathway by Added Chloride Ions in The Oxidation of Aromatic Ketones by Dichloroisocyanuric Acid-A Kinetic StudyDocumento8 pagineShift of Reaction Pathway by Added Chloride Ions in The Oxidation of Aromatic Ketones by Dichloroisocyanuric Acid-A Kinetic StudyHeidi HughesNessuna valutazione finora
- Mucoadhesive Targeted Pulmonary Delivery of Nanoparticulated Dry Powder Insufflators - A Revolt in TB TherapyDocumento8 pagineMucoadhesive Targeted Pulmonary Delivery of Nanoparticulated Dry Powder Insufflators - A Revolt in TB TherapyHeidi HughesNessuna valutazione finora
- Shift of Reaction Pathway by Added Chloride Ions in The Oxidation of Aromatic Ketones by Dichloroisocyanuric Acid-A Kinetic StudyDocumento8 pagineShift of Reaction Pathway by Added Chloride Ions in The Oxidation of Aromatic Ketones by Dichloroisocyanuric Acid-A Kinetic StudyHeidi HughesNessuna valutazione finora
- Novel Coumarin Isoxazoline Derivatives: Synthesis and Study of Antibaterial ActivitiesDocumento16 pagineNovel Coumarin Isoxazoline Derivatives: Synthesis and Study of Antibaterial ActivitiesHeidi HughesNessuna valutazione finora
- Coboloximes Reduction by Iron (II)Documento5 pagineCoboloximes Reduction by Iron (II)Heidi HughesNessuna valutazione finora
- Ruthenium (III) Catalyzed Oxidation of Sugar Alcohols by Dichloroisocyanuric Acid-A Kinetic StudyDocumento8 pagineRuthenium (III) Catalyzed Oxidation of Sugar Alcohols by Dichloroisocyanuric Acid-A Kinetic StudyHeidi HughesNessuna valutazione finora
- Antibacterial Activity of Some Newer 1,2,3 - Benzotriazole Derivatives Synthesized by Ultrasonication in Solvent - Free ConditionsDocumento6 pagineAntibacterial Activity of Some Newer 1,2,3 - Benzotriazole Derivatives Synthesized by Ultrasonication in Solvent - Free ConditionsHeidi HughesNessuna valutazione finora
- Green Approach Toward The Synthesis of N-Substituted Anilines Via Smile Rearrangement Using Amberlite IR-400 ResinDocumento6 pagineGreen Approach Toward The Synthesis of N-Substituted Anilines Via Smile Rearrangement Using Amberlite IR-400 ResinHeidi HughesNessuna valutazione finora
- A Validated RP-HPLC Method For The Determination of Bendamustine Hydrochloride in Tablet Dosage Form Using Gemcitabine Hydrochloride As Internal StandardDocumento8 pagineA Validated RP-HPLC Method For The Determination of Bendamustine Hydrochloride in Tablet Dosage Form Using Gemcitabine Hydrochloride As Internal StandardHeidi HughesNessuna valutazione finora
- Determination of Bendamustine Hydrochloride in Pure and Dosage Forms by Ion-Associative Complex FormationDocumento6 pagineDetermination of Bendamustine Hydrochloride in Pure and Dosage Forms by Ion-Associative Complex FormationHeidi HughesNessuna valutazione finora
- Chemical Oxygen Demand Reduction From Coffee Processing Waste Water - A Comparative Study On Usage of Biosorbents Prepared From Agricultural WastesDocumento10 pagineChemical Oxygen Demand Reduction From Coffee Processing Waste Water - A Comparative Study On Usage of Biosorbents Prepared From Agricultural WastesHeidi HughesNessuna valutazione finora
- Reactions of Enolisable Ketones With Dichloroisocyanuric Acid in Absence and Presence of Added Chloride Ions - A Kinetic StudyDocumento8 pagineReactions of Enolisable Ketones With Dichloroisocyanuric Acid in Absence and Presence of Added Chloride Ions - A Kinetic StudyHeidi HughesNessuna valutazione finora
- Kinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideDocumento9 pagineKinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideHeidi HughesNessuna valutazione finora
- Supercritical Fluid (CO2) Chromatography For Quantitative Determination of Selected Cancer Therapeutic Drugs in The Presence of Potential ImpuritiesDocumento6 pagineSupercritical Fluid (CO2) Chromatography For Quantitative Determination of Selected Cancer Therapeutic Drugs in The Presence of Potential ImpuritiesHeidi HughesNessuna valutazione finora
- Kinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideDocumento9 pagineKinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideHeidi HughesNessuna valutazione finora
- Kinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideDocumento9 pagineKinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideHeidi HughesNessuna valutazione finora
- Reactions of Enolisable Ketones With Dichloroisocyanuric Acid in Absence and Presence of Added Chloride Ions - A Kinetic StudyDocumento8 pagineReactions of Enolisable Ketones With Dichloroisocyanuric Acid in Absence and Presence of Added Chloride Ions - A Kinetic StudyHeidi HughesNessuna valutazione finora
- Role of Added Chloride Ions in Alteration of Reaction Pathway in The Oxidation of Cyclic Ketones by Dichloroisocyanuric Acid - A Kinetic Study1Documento8 pagineRole of Added Chloride Ions in Alteration of Reaction Pathway in The Oxidation of Cyclic Ketones by Dichloroisocyanuric Acid - A Kinetic Study1Heidi HughesNessuna valutazione finora
- Kinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideDocumento9 pagineKinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideHeidi HughesNessuna valutazione finora
- Green Approach Toward The Synthesis of N-Substituted Anilines Via Smile Rearrangement Using Amberlite IR-400 ResinDocumento6 pagineGreen Approach Toward The Synthesis of N-Substituted Anilines Via Smile Rearrangement Using Amberlite IR-400 ResinHeidi HughesNessuna valutazione finora
- Kinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideDocumento9 pagineKinetics and Mechanism of Ru (III) Catalysed and Uncatalysed Oxidation of DL-alanine by N-BromosuccinimideHeidi HughesNessuna valutazione finora
- Supercritical Fluid (CO2) Chromatography For Quantitative Determination of Selected Cancer Therapeutic Drugs in The Presence of Potential ImpuritiesDocumento6 pagineSupercritical Fluid (CO2) Chromatography For Quantitative Determination of Selected Cancer Therapeutic Drugs in The Presence of Potential ImpuritiesHeidi HughesNessuna valutazione finora
- Reactions of Enolisable Ketones With Dichloroisocyanuric Acid in Absence and Presence of Added Chloride Ions - A Kinetic StudyDocumento8 pagineReactions of Enolisable Ketones With Dichloroisocyanuric Acid in Absence and Presence of Added Chloride Ions - A Kinetic StudyHeidi HughesNessuna valutazione finora
- Role of Added Chloride Ions in Alteration of Reaction Pathway in The Oxidation of Cyclic Ketones by Dichloroisocyanuric Acid - A Kinetic Study1Documento8 pagineRole of Added Chloride Ions in Alteration of Reaction Pathway in The Oxidation of Cyclic Ketones by Dichloroisocyanuric Acid - A Kinetic Study1Heidi HughesNessuna valutazione finora
- Supercritical Fluid (CO2) Chromatography For Quantitative Determination of Selected Cancer Therapeutic Drugs in The Presence of Potential ImpuritiesDocumento6 pagineSupercritical Fluid (CO2) Chromatography For Quantitative Determination of Selected Cancer Therapeutic Drugs in The Presence of Potential ImpuritiesHeidi HughesNessuna valutazione finora
- Role of Added Chloride Ions in Alteration of Reaction Pathway in The Oxidation of Cyclic Ketones by Dichloroisocyanuric Acid - A Kinetic Study1Documento8 pagineRole of Added Chloride Ions in Alteration of Reaction Pathway in The Oxidation of Cyclic Ketones by Dichloroisocyanuric Acid - A Kinetic Study1Heidi HughesNessuna valutazione finora
- Supercritical Fluid (CO2) Chromatography For Quantitative Determination of Selected Cancer Therapeutic Drugs in The Presence of Potential ImpuritiesDocumento6 pagineSupercritical Fluid (CO2) Chromatography For Quantitative Determination of Selected Cancer Therapeutic Drugs in The Presence of Potential ImpuritiesHeidi HughesNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)