Potrebbero piacerti anche
- ENVR1401 - Lab 12 - Solid Waste Wastewater Exercise - 2021 PDFDocumento8 pagineENVR1401 - Lab 12 - Solid Waste Wastewater Exercise - 2021 PDFCasey AngellNessuna valutazione finora
- Open Cholecystectomy ReportDocumento7 pagineOpen Cholecystectomy ReportjosephcloudNessuna valutazione finora
- Burn - Concept MapDocumento1 paginaBurn - Concept MapAaron RafaelNessuna valutazione finora
- NCP For Pre-Op Incision CaseDocumento8 pagineNCP For Pre-Op Incision CaseFAt TyNessuna valutazione finora
- 1st Week Reflection - EditedDocumento2 pagine1st Week Reflection - EditedAmrit Acharya100% (1)
- 6 Hysterectomy/TAHBSO Nursing Care Plans: Low Self-EsteemDocumento5 pagine6 Hysterectomy/TAHBSO Nursing Care Plans: Low Self-Esteemonlyone_unik50% (2)
- Exploratory LaparotomyDocumento13 pagineExploratory LaparotomyCj Atto100% (1)
- Goals & Objectives: I. Patient CareDocumento4 pagineGoals & Objectives: I. Patient CareBhawna PandhuNessuna valutazione finora
- Transurethral Resection of The ProstateDocumento48 pagineTransurethral Resection of The Prostateralf_dolanNessuna valutazione finora
- Dano - Rle CeraeDocumento2 pagineDano - Rle CeraeEloisa DanoNessuna valutazione finora
- Ranitidine Tramadol Ketorolac Ampicillin Paracetamol Drug StudyDocumento10 pagineRanitidine Tramadol Ketorolac Ampicillin Paracetamol Drug StudyMarco MoralesNessuna valutazione finora
- Amniotic Fluid EmbolismDocumento30 pagineAmniotic Fluid EmbolismDonmer Ibañez Juan100% (1)
- Clinical Portrait Pertinent DataDocumento9 pagineClinical Portrait Pertinent DataGermin CesaNessuna valutazione finora
- NCP Close Complete Fracture AnxietyDocumento2 pagineNCP Close Complete Fracture AnxietyArt Christian RamosNessuna valutazione finora
- AppendectomyDocumento4 pagineAppendectomyKyre LandinginNessuna valutazione finora
- Cancer Nursing Care Plan (NCP) - Risk For InfectionDocumento2 pagineCancer Nursing Care Plan (NCP) - Risk For InfectionAngie MandeoyaNessuna valutazione finora
- Job Application Letter For NurseDocumento2 pagineJob Application Letter For Nursenur aisyahNessuna valutazione finora
- NCP 1Documento7 pagineNCP 1Roldan VidadNessuna valutazione finora
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDocumento4 pagineTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNessuna valutazione finora
- Nifedipine Drug StudyDocumento2 pagineNifedipine Drug StudyMary Shane MoraldeNessuna valutazione finora
- LOSARTANDocumento3 pagineLOSARTANReinell GoNessuna valutazione finora
- Surgical Ward JournalDocumento6 pagineSurgical Ward JournalMa Genille Samporna SabalNessuna valutazione finora
- NURSING DIAGNOSIS (2) On Pregnant Woman Knowledge DeficitDocumento2 pagineNURSING DIAGNOSIS (2) On Pregnant Woman Knowledge Deficitanon_168410816Nessuna valutazione finora
- Nursing Care Plan ColostomyDocumento5 pagineNursing Care Plan ColostomyCarissa Mae Tapec EstradaNessuna valutazione finora
- COURSE OBJECTIVES or NursingDocumento5 pagineCOURSE OBJECTIVES or NursingFil AquinoNessuna valutazione finora
- Er Journal HgeDocumento3 pagineEr Journal HgeKit LaraNessuna valutazione finora
- NCP (Or) ThyroidectomyDocumento3 pagineNCP (Or) ThyroidectomyChiz CorreNessuna valutazione finora
- GAT NCP Surgery WardDocumento4 pagineGAT NCP Surgery WardDon Richard0% (1)
- Drug Study - CaseDocumento9 pagineDrug Study - CaseMay EvelynNessuna valutazione finora
- CefuroximeDocumento11 pagineCefuroximeAlmira Ballesteros CestonaNessuna valutazione finora
- Pneumo HemothoraxDocumento126 paginePneumo HemothoraxLyra Jan Roo100% (1)
- Discharge PlanDocumento4 pagineDischarge PlanVillanueva NiñaNessuna valutazione finora
- Final Eb ReflectionDocumento2 pagineFinal Eb Reflectionapi-238460511Nessuna valutazione finora
- NCP Skin IntegrityDocumento3 pagineNCP Skin IntegrityAlfie Ayro50% (2)
- ThyroidectomyDocumento11 pagineThyroidectomySherina W. EddingNessuna valutazione finora
- Discharge Plan Post SeizureDocumento2 pagineDischarge Plan Post SeizureVecky TolentinoNessuna valutazione finora
- ENALAPRIL Drug StudyDocumento2 pagineENALAPRIL Drug StudyAjay SupanNessuna valutazione finora
- LFDDocumento3 pagineLFDVhince Norben PiscoNessuna valutazione finora
- I. LearningsDocumento5 pagineI. LearningsMarie Kelsey Acena MacaraigNessuna valutazione finora
- Risk For InfectionDocumento5 pagineRisk For InfectionVianah Eve EscobidoNessuna valutazione finora
- Liceo de Cagayan University College of NursingDocumento29 pagineLiceo de Cagayan University College of Nursingchin41686Nessuna valutazione finora
- Vitamin KDocumento2 pagineVitamin KMuvs RazonNessuna valutazione finora
- RRLDocumento2 pagineRRLbunso padillaNessuna valutazione finora
- Related Learning Experience: Learning Outcomes Day ProceduresDocumento2 pagineRelated Learning Experience: Learning Outcomes Day ProceduresGee RidadNessuna valutazione finora
- Post Open Reduction Internal Fixation PathophysiologyDocumento3 paginePost Open Reduction Internal Fixation PathophysiologyRizalyn QuindipanNessuna valutazione finora
- Impaired Physical MobilityDocumento2 pagineImpaired Physical MobilityJayson OlileNessuna valutazione finora
- Journal ReadingDocumento3 pagineJournal ReadingRachelle Anne LetranNessuna valutazione finora
- Pre-Operative (Incision & Drainage of Abscess)Documento6 paginePre-Operative (Incision & Drainage of Abscess)Eunice MañalacNessuna valutazione finora
- NCP OsteosarcomaDocumento6 pagineNCP OsteosarcomaNiksNessuna valutazione finora
- BSN 215 Reflection Essay - LagoDocumento2 pagineBSN 215 Reflection Essay - LagoAlliahkherzteen LagoNessuna valutazione finora
- Drug Study RifampicinDocumento1 paginaDrug Study RifampicinEphraim MaravillaNessuna valutazione finora
- Nursing Care Plan D-CDocumento2 pagineNursing Care Plan D-CGian MonillaNessuna valutazione finora
- Service Quality of Hospital Outpatient Departments: Patients' PerspectiveDocumento2 pagineService Quality of Hospital Outpatient Departments: Patients' Perspectivelouie john abilaNessuna valutazione finora
- Intravenous Pyelography: Week 5Documento2 pagineIntravenous Pyelography: Week 5Shaina Angelique SaliNessuna valutazione finora
- J.Paquit NCP ECCEDocumento7 pagineJ.Paquit NCP ECCEJon Gab Paquit100% (1)
- Discharge Plan Methods InstructionsDocumento5 pagineDischarge Plan Methods InstructionsKirk CabasaNessuna valutazione finora
- Laparatomi EksplorasiDocumento12 pagineLaparatomi EksplorasiYuda ArifkaNessuna valutazione finora
- Exploratory LaparotomyDocumento13 pagineExploratory LaparotomyFatima Medriza DuranNessuna valutazione finora
- Background - Docx PrintDocumento8 pagineBackground - Docx PrintMarjorie Joy DanzilNessuna valutazione finora
- Exp LapDocumento9 pagineExp LapShreeja SajitNessuna valutazione finora
- Indications: PeritonitisDocumento8 pagineIndications: PeritonitisIrene Soriano BayubayNessuna valutazione finora
- Dr. Edgar Gasco Anatomy LabDocumento3 pagineDr. Edgar Gasco Anatomy LabKris TejereroNessuna valutazione finora
- Ronel NaireDocumento4 pagineRonel NaireKris TejereroNessuna valutazione finora
- PCM (8) Test For Significance (Dr. Tante)Documento151 paginePCM (8) Test For Significance (Dr. Tante)Kris TejereroNessuna valutazione finora
- Histology RespiDocumento4 pagineHistology RespiKris TejereroNessuna valutazione finora
- Lab ANA Set 2Documento6 pagineLab ANA Set 2Kris TejereroNessuna valutazione finora
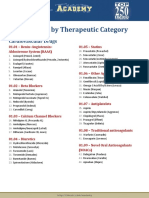
- Drug List by Therapeutic Category: Cardiovascular DrugsDocumento7 pagineDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346Nessuna valutazione finora
- School Stage RoofingDocumento12 pagineSchool Stage RoofingKris TejereroNessuna valutazione finora
- Area Inspection Palpation Auscultation Percussion: Physical AssessmentDocumento6 pagineArea Inspection Palpation Auscultation Percussion: Physical AssessmentKris TejereroNessuna valutazione finora
- Pharma Reviewer From VinnyDocumento16 paginePharma Reviewer From VinnyKris TejereroNessuna valutazione finora
- By: Kris Lyn L. TejereoDocumento30 pagineBy: Kris Lyn L. TejereoKris TejereroNessuna valutazione finora
- NCM 104 Cellular Aberration Lecture 2007Documento104 pagineNCM 104 Cellular Aberration Lecture 2007Kris TejereroNessuna valutazione finora
- Cellular AberrationDocumento71 pagineCellular AberrationKris TejereroNessuna valutazione finora
- Vaccine Minimum Age at 1st Dose Number of Doses Dose Minimum Interval Between Doses Route Site ReasonDocumento4 pagineVaccine Minimum Age at 1st Dose Number of Doses Dose Minimum Interval Between Doses Route Site ReasonKris TejereroNessuna valutazione finora
- Laboratory Studies: FecalysisDocumento2 pagineLaboratory Studies: FecalysisKris TejereroNessuna valutazione finora
- Algor Mortis - Cooling of The Body-: Antemortem Agonal Period Postmortem Postmortem ChangesDocumento13 pagineAlgor Mortis - Cooling of The Body-: Antemortem Agonal Period Postmortem Postmortem ChangesKris TejereroNessuna valutazione finora
- Process Recording WMCCDocumento3 pagineProcess Recording WMCCKris TejereroNessuna valutazione finora
- Nursing Care Plan: Name of Patient: - Age: - SexDocumento4 pagineNursing Care Plan: Name of Patient: - Age: - SexKris TejereroNessuna valutazione finora
- HIV DrugsDocumento31 pagineHIV DrugsKris TejereroNessuna valutazione finora
- FPGA-based System For Heart Rate Monitoring PDFDocumento12 pagineFPGA-based System For Heart Rate Monitoring PDFkishorechiyaNessuna valutazione finora
- Solar Grass Cutter MachDocumento21 pagineSolar Grass Cutter MachAnonymous I13s99Nessuna valutazione finora
- Complete Prerequisite Program v2Documento78 pagineComplete Prerequisite Program v2Ramasubramanian Sankaranarayanan100% (1)
- Real Time EvaluationDocumento3 pagineReal Time Evaluationأيوب علاءNessuna valutazione finora
- Ansi Asa S3.22 - 2014Documento54 pagineAnsi Asa S3.22 - 20147620383tlNessuna valutazione finora
- Improving Communication Skills of Pharmacy StudentDocumento13 pagineImproving Communication Skills of Pharmacy StudentAbdul QadirNessuna valutazione finora
- Reticular AbscessDocumento4 pagineReticular AbscessSasikala KaliapanNessuna valutazione finora
- ES9-62 Ingestive Cleaning PDocumento9 pagineES9-62 Ingestive Cleaning PIfran Sierra100% (1)
- Thai Cuisine: Reporters: Bantayan, Kenneth Samejon, Clarish Lovely Relevo, Mary GraceDocumento47 pagineThai Cuisine: Reporters: Bantayan, Kenneth Samejon, Clarish Lovely Relevo, Mary Gracemiralona relevoNessuna valutazione finora
- Draw-Through or Blow-Through: Components of Air Handling UnitDocumento23 pagineDraw-Through or Blow-Through: Components of Air Handling Unityousuff0% (1)
- 55 Gentle Ways To Take Care of Yourself When You're Busy Busy BusyDocumento7 pagine55 Gentle Ways To Take Care of Yourself When You're Busy Busy Busyvanjami100% (1)
- Assignment 4Documento4 pagineAssignment 4ShabihNessuna valutazione finora
- Aswani Construction R 07102013Documento3 pagineAswani Construction R 07102013Balaji RathinavelNessuna valutazione finora
- Corrosion Short Courses - Environmental CrackingDocumento8 pagineCorrosion Short Courses - Environmental CrackingMario SalayaNessuna valutazione finora
- Mechanical Pumps: N. HilleretDocumento12 pagineMechanical Pumps: N. HilleretAmrik SinghNessuna valutazione finora
- Ocean StarDocumento36 pagineOcean Starrobertshepard1967Nessuna valutazione finora
- BS Pharmacy - ProspectusDocumento9 pagineBS Pharmacy - ProspectusDomz BucadNessuna valutazione finora
- Tokyo Fact SheetDocumento17 pagineTokyo Fact Sheethoangnguyen2401Nessuna valutazione finora
- Norsok R 002Documento186 pagineNorsok R 002robson2015Nessuna valutazione finora
- Research Methods - Print - QuizizzDocumento5 pagineResearch Methods - Print - QuizizzpecmbaNessuna valutazione finora
- Amirtha ProjectDocumento18 pagineAmirtha Projectaeriel judson100% (1)
- Membrane AutopsyDocumento2 pagineMembrane AutopsyBiljana TausanovicNessuna valutazione finora
- Biecco Lawrie Ece Gec Reyrolle Burn Jyoti SwitchgearDocumento18 pagineBiecco Lawrie Ece Gec Reyrolle Burn Jyoti SwitchgearSharafat AliNessuna valutazione finora
- ENG 110-Task 4 (Unintended Messages)Documento2 pagineENG 110-Task 4 (Unintended Messages)Erika Noreen Dela RosaNessuna valutazione finora
- D435L09 Dental Trauma-2C Cracked Teeth - 26 Root FractureDocumento73 pagineD435L09 Dental Trauma-2C Cracked Teeth - 26 Root FractureD YasIr MussaNessuna valutazione finora
- @9negros Occidental Vs BezoreDocumento3 pagine@9negros Occidental Vs BezoreSimeon SuanNessuna valutazione finora
- Matter and Change 2008 Chapter 14Documento40 pagineMatter and Change 2008 Chapter 14cattmy100% (1)
- Chapter 2 - Alkanes PDFDocumento54 pagineChapter 2 - Alkanes PDFSITI NUR ALISSA BINTI AHMAD RASMANNessuna valutazione finora
- Bradycardia AlgorithmDocumento1 paginaBradycardia AlgorithmGideon BahuleNessuna valutazione finora