Potrebbero piacerti anche
- Management of Tuberculosis: A guide for clinicians (eBook edition)Da EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Nessuna valutazione finora
- Cleft Lip PalateDocumento37 pagineCleft Lip PalateMuhammad Hamid Muktashim100% (1)
- Craniotomy Case StudyDocumento14 pagineCraniotomy Case StudyHoney Semafranca PlatolonNessuna valutazione finora
- Case Study - Balanced Skeletal TractionDocumento1 paginaCase Study - Balanced Skeletal Tractionzeverino castillo50% (2)
- Geriatric For JustineDocumento28 pagineGeriatric For JustineJaylord VerazonNessuna valutazione finora
- Cleft Lip and PalateDocumento20 pagineCleft Lip and Palatejapzee1988100% (1)
- MS 3 Case Analysis DownloadableDocumento1 paginaMS 3 Case Analysis DownloadableCharissa Magistrado De LeonNessuna valutazione finora
- Nasal PolypsDocumento20 pagineNasal PolypsPauleenNessuna valutazione finora
- Periop QuizesDocumento9 paginePeriop QuizesAnonymous ZQ4gHahzNessuna valutazione finora
- CraniotomyDocumento6 pagineCraniotomychaSephNessuna valutazione finora
- TahbsoDocumento4 pagineTahbsomichZ_13Nessuna valutazione finora
- NCPDocumento10 pagineNCPCristina L. JaysonNessuna valutazione finora
- Lesson 1 POST TEST Maternal FrameworkDocumento1 paginaLesson 1 POST TEST Maternal FrameworkAnnalisa TellesNessuna valutazione finora
- Thyroidectomy 2 DDocumento35 pagineThyroidectomy 2 DKim Jun-myeonNessuna valutazione finora
- Skin Grafting Surgical NursingDocumento21 pagineSkin Grafting Surgical NursingHEMMA100% (1)
- Uterine Rupture: Mariano Marcos StateDocumento10 pagineUterine Rupture: Mariano Marcos StateSalvaje CaballeroNessuna valutazione finora
- Open Cholecystectomy ReportDocumento7 pagineOpen Cholecystectomy ReportjosephcloudNessuna valutazione finora
- Core CompetencyDocumento9 pagineCore CompetencyCharm BarinosNessuna valutazione finora
- Ahmed Copd Case StudyDocumento6 pagineAhmed Copd Case StudyAhmad BaolayyanNessuna valutazione finora
- Case Study - Toxic GoiterDocumento22 pagineCase Study - Toxic GoiterJohn Matley Caampued100% (2)
- Craniotomy Case ReportDocumento19 pagineCraniotomy Case ReportElizar MercadoNessuna valutazione finora
- Case Study Medical WardDocumento4 pagineCase Study Medical WardFrancis Antonio Llenaresas QuijanoNessuna valutazione finora
- USC Case 04 - SinusitisDocumento9 pagineUSC Case 04 - SinusitisDisti Damelia SebayangNessuna valutazione finora
- Post Op Case Studies StudentsDocumento19 paginePost Op Case Studies StudentsRenie SerranoNessuna valutazione finora
- TracheostomyDocumento4 pagineTracheostomySuchismita SethiNessuna valutazione finora
- Posterior Mold: PurposeDocumento3 paginePosterior Mold: PurposeSheryl Ann Barit PedinesNessuna valutazione finora
- A Case Study About Cleft Lip and Cleft PalateDocumento12 pagineA Case Study About Cleft Lip and Cleft PalateMaegan Pearl83% (6)
- Appendectomy O.R. Write UpDocumento11 pagineAppendectomy O.R. Write UpJessica Christine Datuin GustiloNessuna valutazione finora
- Impetigo PathophysiologyDocumento1 paginaImpetigo PathophysiologyCesar Arada100% (1)
- Pathophysiology AbrasionDocumento3 paginePathophysiology AbrasionVito VitoNessuna valutazione finora
- ColorectalCancer - Case StudyDocumento28 pagineColorectalCancer - Case StudyColeen Mae CamaristaNessuna valutazione finora
- Introduction To Gerontological Nursing: - Jerald I. Corpuz, RNDocumento16 pagineIntroduction To Gerontological Nursing: - Jerald I. Corpuz, RNjoyrena ochondra100% (1)
- Operating Room Nurses Knowledge and Practice of Sterile Technique 2167 1168.1000113Documento5 pagineOperating Room Nurses Knowledge and Practice of Sterile Technique 2167 1168.1000113mlbrown8Nessuna valutazione finora
- PYOMYOSITISDocumento12 paginePYOMYOSITISPaolo VillaNessuna valutazione finora
- Cast CareDocumento1 paginaCast CareCarmelita SaltNessuna valutazione finora
- HNP Case Scenario For Case StudyDocumento2 pagineHNP Case Scenario For Case StudyDeinielle Magdangal RomeroNessuna valutazione finora
- NCPs For ParotidectomyDocumento8 pagineNCPs For ParotidectomyAcohCChao100% (1)
- SinusitisDocumento6 pagineSinusitisRae Marie AquinoNessuna valutazione finora
- Oxygen TherapyDocumento3 pagineOxygen Therapymarie100% (3)
- Tahbso ArticleDocumento4 pagineTahbso ArticleAlianna Kristine OhNessuna valutazione finora
- Ongoing AppraisalDocumento2 pagineOngoing AppraisalLouisa Marie MirandaNessuna valutazione finora
- Related Learning Experience: Learning Outcomes Day ProceduresDocumento2 pagineRelated Learning Experience: Learning Outcomes Day ProceduresGee RidadNessuna valutazione finora
- Procedure - Gastric LavageDocumento2 pagineProcedure - Gastric LavageJose Paul RaderNessuna valutazione finora
- Acute TonsillopharyngitisDocumento17 pagineAcute TonsillopharyngitisRachel Haide NaravalNessuna valutazione finora
- Preoperative Skin PreparationDocumento16 paginePreoperative Skin PreparationSyahri DzikriNessuna valutazione finora
- Aetiology Heart Diasease in Children May Be Congenital or AcquiredDocumento23 pagineAetiology Heart Diasease in Children May Be Congenital or AcquiredkasondaNessuna valutazione finora
- Case Study Main OtDocumento56 pagineCase Study Main Otamier_s100% (1)
- P.A. 1Documento6 pagineP.A. 1SamSarah BongolanNessuna valutazione finora
- Cleft Lip and Cleft PalateDocumento8 pagineCleft Lip and Cleft PalateRAJU33% (3)
- Case Presentation Meyke Liechandra C11109130 Fracture ClavicleDocumento24 pagineCase Presentation Meyke Liechandra C11109130 Fracture ClavicleWahyunita IlhamNessuna valutazione finora
- Dissecting ForcepsDocumento9 pagineDissecting ForcepsYdynn Parejas GavinaNessuna valutazione finora
- CASE STUDY - Community Acquired Pneumonia With Pleural Effusion & UTIDocumento73 pagineCASE STUDY - Community Acquired Pneumonia With Pleural Effusion & UTIFrancis AdrianNessuna valutazione finora
- AppendicitisDocumento8 pagineAppendicitisAndini YusniaNessuna valutazione finora
- DM & DI ExamsDocumento11 pagineDM & DI ExamsTomzki CornelioNessuna valutazione finora
- Tension Pneumothorax: Modifiable FactorsDocumento3 pagineTension Pneumothorax: Modifiable FactorsJustin MaverickNessuna valutazione finora
- Assessment and Management of Patients With Hearing and Balance Disorders WebDocumento36 pagineAssessment and Management of Patients With Hearing and Balance Disorders Webmalinda0% (1)
- Intestinal Obstruction A Case StudyDocumento44 pagineIntestinal Obstruction A Case StudyikemasNessuna valutazione finora
- Journal of Cranio-Maxillo-Facial SurgeryDocumento6 pagineJournal of Cranio-Maxillo-Facial SurgeryKihyun YooNessuna valutazione finora
- Dento-Alveolar Development in Unilateral Cleft Lip, Alveolus and PalateDocumento5 pagineDento-Alveolar Development in Unilateral Cleft Lip, Alveolus and PalateLuiz Guilherme LoivosNessuna valutazione finora
- 2018 Timing of Furlow Palatoplasty For Patients With Submucous Cleft PalateDocumento7 pagine2018 Timing of Furlow Palatoplasty For Patients With Submucous Cleft PalateDimitris RodriguezNessuna valutazione finora
- Final ScheduleDocumento1 paginaFinal ScheduleSometwo C. HangalNessuna valutazione finora
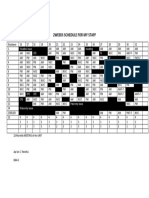
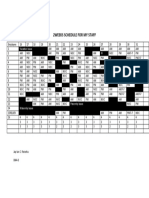
- 2weeks Schedule For My StaffDocumento1 pagina2weeks Schedule For My StaffSometwo C. HangalNessuna valutazione finora
- 2weeks Schedule For My StaffDocumento1 pagina2weeks Schedule For My StaffSometwo C. HangalNessuna valutazione finora
- 2weeks Schedule For My StaffDocumento1 pagina2weeks Schedule For My StaffSometwo C. HangalNessuna valutazione finora
- 2weeks Schedule For My StaffDocumento1 pagina2weeks Schedule For My StaffSometwo C. HangalNessuna valutazione finora
- Interview TAENESSDocumento2 pagineInterview TAENESSSometwo C. HangalNessuna valutazione finora
- The Key To Success Is Through HARD WORKDocumento1 paginaThe Key To Success Is Through HARD WORKSometwo C. HangalNessuna valutazione finora
- Perioperative of ORIFDocumento27 paginePerioperative of ORIFSometwo C. Hangal91% (11)
- Am No. 98-5-01-SC, Nov 9 1998 in Re Hon Mateo ValenzuelaDocumento9 pagineAm No. 98-5-01-SC, Nov 9 1998 in Re Hon Mateo Valenzuelaian clark MarinduqueNessuna valutazione finora
- Risk Management NotesDocumento27 pagineRisk Management NoteskomalNessuna valutazione finora
- Engineering Economics & Financial Accounting Two Mark Questions and AnswersDocumento15 pagineEngineering Economics & Financial Accounting Two Mark Questions and AnswerspothigaiselvansNessuna valutazione finora
- 2 BA British and American Life and InstitutionsDocumento3 pagine2 BA British and American Life and Institutionsguest1957Nessuna valutazione finora
- Scottish Myths and Legends (PDFDrive)Documento181 pagineScottish Myths and Legends (PDFDrive)VeraNessuna valutazione finora
- A Deep Dive Into 3D-NAND Silicon Linkage To Storage System Performance & ReliabilityDocumento15 pagineA Deep Dive Into 3D-NAND Silicon Linkage To Storage System Performance & ReliabilityHeekwan SonNessuna valutazione finora
- Cee 213 - Transport Principles in Environmental and Water Resources EngineeringDocumento3 pagineCee 213 - Transport Principles in Environmental and Water Resources EngineeringenjpetNessuna valutazione finora
- Current Trends in Teaching and Learning EFLDocumento13 pagineCurrent Trends in Teaching and Learning EFLyimigor100% (1)
- APPELANTDocumento30 pagineAPPELANTTAS MUNNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaBang UsopNessuna valutazione finora
- Data Flow DiagramDocumento21 pagineData Flow Diagrampredikat newsNessuna valutazione finora
- Critical Methodology Analysis: 360' Degree Feedback: Its Role in Employee DevelopmentDocumento3 pagineCritical Methodology Analysis: 360' Degree Feedback: Its Role in Employee DevelopmentJatin KaushikNessuna valutazione finora
- Travel To Egypt: Conversation Cheat SheetDocumento2 pagineTravel To Egypt: Conversation Cheat SheetNasima BegumNessuna valutazione finora
- A Natural Disaster Story: World Scout Environment BadgeDocumento4 pagineA Natural Disaster Story: World Scout Environment BadgeMurali Krishna TNessuna valutazione finora
- Batch Fed BatchDocumento60 pagineBatch Fed BatchAyesha RalliyaNessuna valutazione finora
- Cav PDFDocumento6 pagineCav PDFshandediaz1600Nessuna valutazione finora
- A Multivariate Model For Analyzing Crime Scene InformationDocumento26 pagineA Multivariate Model For Analyzing Crime Scene InformationNorberth Ioan OkrosNessuna valutazione finora
- Chraj 1Documento6 pagineChraj 1The Independent GhanaNessuna valutazione finora
- Technology Theatres, Plays and PerformanceDocumento48 pagineTechnology Theatres, Plays and PerformanceHannah Williams WaltonNessuna valutazione finora
- Programme Guide - PGDMCH PDFDocumento58 pagineProgramme Guide - PGDMCH PDFNJMU 2006Nessuna valutazione finora
- Scholars' Letter On SCOTUS Ethics CodeDocumento2 pagineScholars' Letter On SCOTUS Ethics CodeConcerned citizen50% (2)
- Digital Marketing - Scope Opportunities and Challenges - IntechOpen PDFDocumento31 pagineDigital Marketing - Scope Opportunities and Challenges - IntechOpen PDFPratsNessuna valutazione finora
- Dot Net TricksDocumento101 pagineDot Net TrickssathishmnmNessuna valutazione finora
- C5 Schematy 1 PDFDocumento294 pagineC5 Schematy 1 PDFArtur Arturowski100% (4)
- Prepositioncombinations PDFDocumento14 paginePrepositioncombinations PDFMichalisBenedictusNessuna valutazione finora
- Mao InoueDocumento9 pagineMao InoueNemanja IlicNessuna valutazione finora
- Coronavirus Disease (COVID-19) : Situation Report - 125Documento17 pagineCoronavirus Disease (COVID-19) : Situation Report - 125CityNewsTorontoNessuna valutazione finora
- Indian Entrepreneur Fund PresentationDocumento44 pagineIndian Entrepreneur Fund PresentationHARIHARAN ANessuna valutazione finora
- HR Awards PPT 2020 12.09.2020 FinalDocumento64 pagineHR Awards PPT 2020 12.09.2020 FinalLolo OhwNessuna valutazione finora
- Will's Red Coat: The Story of One Old Dog Who Chose to Live AgainDa EverandWill's Red Coat: The Story of One Old Dog Who Chose to Live AgainValutazione: 4.5 su 5 stelle4.5/5 (18)
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessDa EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessNessuna valutazione finora
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueDa EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueValutazione: 4.5 su 5 stelle4.5/5 (27)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueDa EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueValutazione: 5 su 5 stelle5/5 (3)
- An Eagle Named Freedom: My True Story of a Remarkable FriendshipDa EverandAn Eagle Named Freedom: My True Story of a Remarkable FriendshipNessuna valutazione finora
- The Dog Listener: Learn How to Communicate with Your Dog for Willing CooperationDa EverandThe Dog Listener: Learn How to Communicate with Your Dog for Willing CooperationValutazione: 4 su 5 stelle4/5 (37)
- Merle's Door: Lessons from a Freethinking DogDa EverandMerle's Door: Lessons from a Freethinking DogValutazione: 4 su 5 stelle4/5 (326)
- The Dog Who Couldn't Stop Loving: How Dogs Have Captured Our Hearts for Thousands of YearsDa EverandThe Dog Who Couldn't Stop Loving: How Dogs Have Captured Our Hearts for Thousands of YearsNessuna valutazione finora
- Our Dogs, Ourselves: The Story of a Singular BondDa EverandOur Dogs, Ourselves: The Story of a Singular BondValutazione: 4 su 5 stelle4/5 (21)
- Dogland: Passion, Glory, and Lots of Slobber at the Westminster Dog ShowDa EverandDogland: Passion, Glory, and Lots of Slobber at the Westminster Dog ShowNessuna valutazione finora
- Your Dog Is Your Mirror: The Emotional Capacity of Our Dogs and OurselvesDa EverandYour Dog Is Your Mirror: The Emotional Capacity of Our Dogs and OurselvesValutazione: 4 su 5 stelle4/5 (31)
- Second Chances: A Marine, His Dog, and Finding RedemptionDa EverandSecond Chances: A Marine, His Dog, and Finding RedemptionNessuna valutazione finora
- Show Dog: The Charmed Life and Trying Times of a Near-Perfect PurebredDa EverandShow Dog: The Charmed Life and Trying Times of a Near-Perfect PurebredValutazione: 3.5 su 5 stelle3.5/5 (13)
- The Other End of the Leash: Why We Do What We Do Around DogsDa EverandThe Other End of the Leash: Why We Do What We Do Around DogsValutazione: 5 su 5 stelle5/5 (65)
- Come Back, Como: Winning the Heart of a Reluctant DogDa EverandCome Back, Como: Winning the Heart of a Reluctant DogValutazione: 3.5 su 5 stelle3.5/5 (10)
- Puppy Training 101: How to Train a Puppy, Training Your Own Psychiatric Service Dog, A Step-By-Step Program so your Pup Will Understand You!Da EverandPuppy Training 101: How to Train a Puppy, Training Your Own Psychiatric Service Dog, A Step-By-Step Program so your Pup Will Understand You!Valutazione: 5 su 5 stelle5/5 (85)
- Edward's Menagerie: Dogs: 50 canine crochet patternsDa EverandEdward's Menagerie: Dogs: 50 canine crochet patternsValutazione: 3 su 5 stelle3/5 (5)
- Inside of a Dog: What Dogs See, Smell, and KnowDa EverandInside of a Dog: What Dogs See, Smell, and KnowValutazione: 4 su 5 stelle4/5 (390)
- Lucky Dog Lessons: Train Your Dog in 7 DaysDa EverandLucky Dog Lessons: Train Your Dog in 7 DaysValutazione: 4.5 su 5 stelle4.5/5 (41)
- What Cats Want: An Illustrated Guide for Truly Understanding Your CatDa EverandWhat Cats Want: An Illustrated Guide for Truly Understanding Your CatValutazione: 4.5 su 5 stelle4.5/5 (13)
- Arthur: The Dog Who Crossed the Jungle to Find a HomeDa EverandArthur: The Dog Who Crossed the Jungle to Find a HomeValutazione: 4.5 su 5 stelle4.5/5 (20)
- How Dogs Think: What the World Looks Like to Them and Why They Act the Way They DoDa EverandHow Dogs Think: What the World Looks Like to Them and Why They Act the Way They DoValutazione: 4 su 5 stelle4/5 (46)
- Tamed and Untamed: Close Encounters of the Animal KindDa EverandTamed and Untamed: Close Encounters of the Animal KindValutazione: 3.5 su 5 stelle3.5/5 (32)
- How to Be Your Dog's Best Friend: A Training Manual for Dog ownersDa EverandHow to Be Your Dog's Best Friend: A Training Manual for Dog ownersValutazione: 4 su 5 stelle4/5 (120)
- Julia's Cats: Julia Child's Life in the Company of CatsDa EverandJulia's Cats: Julia Child's Life in the Company of CatsValutazione: 4.5 su 5 stelle4.5/5 (24)