Potrebbero piacerti anche
- Dr. Seuss UnitDocumento13 pagineDr. Seuss Unitgoobers51Nessuna valutazione finora
- Hormonal Physiology of Childbearing PDFDocumento248 pagineHormonal Physiology of Childbearing PDFRosemaryCastro100% (1)
- FREESchool Supply LabelsDocumento1 paginaFREESchool Supply LabelsRosemaryCastroNessuna valutazione finora
- Scrabble Words Lips PageDocumento1 paginaScrabble Words Lips PageRosemaryCastroNessuna valutazione finora
- OB ReviewDocumento257 pagineOB ReviewRosemaryCastro100% (1)
- Neonatal Resuscitation Program DiagramDocumento1 paginaNeonatal Resuscitation Program DiagramRosemaryCastroNessuna valutazione finora
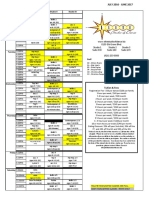
- EliteSchedule16 17mar172017 PDFDocumento1 paginaEliteSchedule16 17mar172017 PDFRosemaryCastroNessuna valutazione finora
- Hormonal Physiology of Childbearing PDFDocumento248 pagineHormonal Physiology of Childbearing PDFRosemaryCastro100% (1)
- Bathroom SuperheroDocumento6 pagineBathroom SuperheroRosemaryCastroNessuna valutazione finora
- SrableDocumento39 pagineSrableYatza Sanches SanchesNessuna valutazione finora
- Obstetrics ReviewDocumento257 pagineObstetrics ReviewRosemaryCastroNessuna valutazione finora
- SrableDocumento39 pagineSrableYatza Sanches SanchesNessuna valutazione finora
- Resuscitation and Support of Transition of Babies at Birth PDFDocumento11 pagineResuscitation and Support of Transition of Babies at Birth PDFRosemaryCastroNessuna valutazione finora
- IV Solutions CheatsheetDocumento1 paginaIV Solutions CheatsheetRosemaryCastroNessuna valutazione finora
- NRP GeneralDocumento1 paginaNRP GeneralRosemaryCastroNessuna valutazione finora
- Taylor 2008 The STABLER Program Postresuscitation Pretransport Stabilization Care of Sick Infants PDFDocumento7 pagineTaylor 2008 The STABLER Program Postresuscitation Pretransport Stabilization Care of Sick Infants PDFRosemaryCastroNessuna valutazione finora
- ABG ROME FlowchartDocumento1 paginaABG ROME FlowchartRosemaryCastroNessuna valutazione finora
- Loan Forgiveness For Nurses Application NeedsDocumento5 pagineLoan Forgiveness For Nurses Application NeedsRosemaryCastroNessuna valutazione finora
- BrainSheet 3patientDocumento2 pagineBrainSheet 3patientRosemaryCastroNessuna valutazione finora
- SIM Lab Sign UpsDocumento3 pagineSIM Lab Sign UpsRosemaryCastroNessuna valutazione finora
- Monthly Shot-March 2016Documento7 pagineMonthly Shot-March 2016RosemaryCastroNessuna valutazione finora
- Where Have I Been While in NURSING SCHOOL?: Résumé Worksheet Belonging To - Save MeDocumento2 pagineWhere Have I Been While in NURSING SCHOOL?: Résumé Worksheet Belonging To - Save MeRosemaryCastroNessuna valutazione finora
- Monthly Shot January 2016Documento7 pagineMonthly Shot January 2016RosemaryCastroNessuna valutazione finora
- National Wear Red Day newsletterDocumento4 pagineNational Wear Red Day newsletterRosemaryCastroNessuna valutazione finora
- PHN SAMPLE AppDocumento3 paginePHN SAMPLE AppRosemaryCastroNessuna valutazione finora
- NCLEX Nursing Exam Cram SheetDocumento9 pagineNCLEX Nursing Exam Cram SheetJodie OrangeNessuna valutazione finora
- National Travel Fund Application1Documento2 pagineNational Travel Fund Application1RosemaryCastroNessuna valutazione finora
- Exam Cram Cheet SheetDocumento2 pagineExam Cram Cheet SheetSheila Stenson-Roberts100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)