Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Clinical ReflectionDocumento4 pagineClinical Reflectionapi-316342033Nessuna valutazione finora
- Patho 2 MaternityDocumento1 paginaPatho 2 Maternityapi-316342033Nessuna valutazione finora
- Ureter Stent PlacementDocumento1 paginaUreter Stent Placementapi-316342033Nessuna valutazione finora
- Thailand Traditions and BeliefsDocumento6 pagineThailand Traditions and Beliefsapi-316342033100% (1)
- Community Resource n320Documento4 pagineCommunity Resource n320api-316342033Nessuna valutazione finora
- The Minor Ethical Dilemma-Forced Chemotherapy On A TeenDocumento6 pagineThe Minor Ethical Dilemma-Forced Chemotherapy On A TeenNaomi MasudaNessuna valutazione finora
- PDP Template 1Documento2 paginePDP Template 1api-316342033Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Inventory ManagementDocumento24 pagineInventory ManagementMohamed LaghyatiNessuna valutazione finora
- List of Doctors Certified To Recommend Pot To PatientsDocumento22 pagineList of Doctors Certified To Recommend Pot To PatientsLashawn McQueenNessuna valutazione finora
- Practical Cardio-Oncology (2019, CRC Press)Documento261 paginePractical Cardio-Oncology (2019, CRC Press)Anitei GabrielaNessuna valutazione finora
- The Aspects of Gene TherapyDocumento15 pagineThe Aspects of Gene TherapyLaleth Mendoza Ojales0% (1)
- Emt Schedule 2014-15 RVD 10-27-14Documento3 pagineEmt Schedule 2014-15 RVD 10-27-14api-257829824Nessuna valutazione finora
- The Exotic Pet Consultation: History TakingDocumento3 pagineThe Exotic Pet Consultation: History TakingDavid PGNessuna valutazione finora
- NCP of Fever and HypertensionDocumento2 pagineNCP of Fever and HypertensionDayan CabrigaNessuna valutazione finora
- Adolescent Substance AbuseDocumento47 pagineAdolescent Substance AbuseIssa Thea BolanteNessuna valutazione finora
- Health 10 4th QDocumento4 pagineHealth 10 4th QLeonilo C. Dumaguing Jr.Nessuna valutazione finora
- MD India Forms & Policy DocumentDocumento42 pagineMD India Forms & Policy DocumentYagantiGaneshRaghuveerNessuna valutazione finora
- Nursing Process: Mrs. Sumaira Noreen Senior Nursing InstructorDocumento40 pagineNursing Process: Mrs. Sumaira Noreen Senior Nursing InstructorSumaira NoreenNessuna valutazione finora
- Neutral Zone Concept and Its Technique at Impression Stage PDFDocumento7 pagineNeutral Zone Concept and Its Technique at Impression Stage PDFgeneral generalNessuna valutazione finora
- Prevalence and Recurrence Rate of Perianal Abscess - A Population-Based Study, Sweden 1997 - 2009Documento5 paginePrevalence and Recurrence Rate of Perianal Abscess - A Population-Based Study, Sweden 1997 - 2009Ridha Aswina DalimuntheNessuna valutazione finora
- Mental StatusDocumento6 pagineMental StatusIgor Oliveira100% (1)
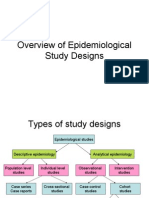
- Overview of Epidemiological Study DesignsDocumento16 pagineOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- VSRDocumento12 pagineVSRDrkrunal badaniNessuna valutazione finora
- Problem PrioritizationDocumento2 pagineProblem PrioritizationRegie GonzagaNessuna valutazione finora
- Form Self Assesment Diagnosa Non Spesialistik Luaran Aplikasi HfisDocumento8 pagineForm Self Assesment Diagnosa Non Spesialistik Luaran Aplikasi HfisEverly Christian CorputtyNessuna valutazione finora
- History of LaparosDocumento27 pagineHistory of LaparosDr. Sanjay KolteNessuna valutazione finora
- Medical Tourism Consultants in IndiaDocumento11 pagineMedical Tourism Consultants in IndiaHealth NirvaanaNessuna valutazione finora
- ConnectiCare Bronze StandardDocumento98 pagineConnectiCare Bronze Standardalex647Nessuna valutazione finora
- Obstetric History and Physical Examination (Ina Irabon)Documento49 pagineObstetric History and Physical Examination (Ina Irabon)Benjamin Gabriel100% (1)
- Rcse9702 115 s1Documento1 paginaRcse9702 115 s1WayyuNessuna valutazione finora
- ERF IMC3 IMC4 Evaluation ENGDocumento4 pagineERF IMC3 IMC4 Evaluation ENGNsabimana PatrickNessuna valutazione finora
- Hyperthermia HIV NURSING CARE PLAN FLODocumento4 pagineHyperthermia HIV NURSING CARE PLAN FLOMicaela CrisostomoNessuna valutazione finora
- Health Care Delivery System 1Documento21 pagineHealth Care Delivery System 1Carson BirthNessuna valutazione finora
- Interview - Test - Educazione ServiziDocumento4 pagineInterview - Test - Educazione ServiziRounak BasuNessuna valutazione finora
- AAO UveitisDocumento39 pagineAAO UveitisSafa Abdualrahaman Ali HamadNessuna valutazione finora
- As A General Goal, Aim For at Least 30 Minutes of Moderate Physical Activity Every Specific Fitness Goals, You May Need To Exercise MoreDocumento5 pagineAs A General Goal, Aim For at Least 30 Minutes of Moderate Physical Activity Every Specific Fitness Goals, You May Need To Exercise MoreJessa Briones100% (1)
- Prostho-Perio-Restorative Interrelationship ADocumento6 pagineProstho-Perio-Restorative Interrelationship AAlipio GarcíaNessuna valutazione finora