Potrebbero piacerti anche
- DeclarationOfLivingMan MHTDocumento3 pagineDeclarationOfLivingMan MHTRachel Rey100% (3)
- Basic Life Support (BLS) Provider HandbookDa EverandBasic Life Support (BLS) Provider HandbookValutazione: 5 su 5 stelle5/5 (2)
- Journal Reading AminophyllineDocumento76 pagineJournal Reading AminophyllinePandhu Suprobo100% (1)
- HFpEF MeDocumento28 pagineHFpEF MeRidwan YasinNessuna valutazione finora
- Krisis Tiroid FixDocumento38 pagineKrisis Tiroid FixVita DesriantiNessuna valutazione finora
- Theodore G. Bilbo - Take Your Choice - Separation or Mongrelization (1946)Documento227 pagineTheodore G. Bilbo - Take Your Choice - Separation or Mongrelization (1946)gibmedat100% (1)
- MMN Pulmo Full Rezy PDFDocumento102 pagineMMN Pulmo Full Rezy PDFmataNessuna valutazione finora
- University of San Carlos V CADocumento1 paginaUniversity of San Carlos V CATrisha Dela RosaNessuna valutazione finora
- Contoh Soal PPDS Anak (Sub Kardiologi)Documento3 pagineContoh Soal PPDS Anak (Sub Kardiologi)rezkadehaNessuna valutazione finora
- Liver Cirrhosis: Review HepatologyDocumento71 pagineLiver Cirrhosis: Review HepatologyAstri Arri FebriantiNessuna valutazione finora
- DR Dicky L Tahapary SPPD PhD-Hyperglycemic Crises IMELS PDFDocumento38 pagineDR Dicky L Tahapary SPPD PhD-Hyperglycemic Crises IMELS PDFDemograf27Nessuna valutazione finora
- IPD - Kardiologi PDFDocumento114 pagineIPD - Kardiologi PDFAnnisa Rahmadhania100% (1)
- Soal Juni Beserta KunciDocumento76 pagineSoal Juni Beserta Kuncirsiamb100% (1)
- TROMBOSISDocumento49 pagineTROMBOSISAgung WistaraNessuna valutazione finora
- Soal2 EkgDocumento64 pagineSoal2 Ekgaandaku100% (1)
- P-00092 SecurityOfficerHandbook 1012Documento31 pagineP-00092 SecurityOfficerHandbook 1012Yscha MacedaNessuna valutazione finora
- Steps EchoDocumento2 pagineSteps EchoBagus Andi PramonoNessuna valutazione finora
- DIC - IMELS (Compatibility Mode)Documento30 pagineDIC - IMELS (Compatibility Mode)Astri Arri FebriantiNessuna valutazione finora
- Antony Eastmon, Ed - Byzantium's Other Empire TrebizondDocumento264 pagineAntony Eastmon, Ed - Byzantium's Other Empire TrebizondborjaNessuna valutazione finora
- Final Cardiovascular Unhas 2013Documento18 pagineFinal Cardiovascular Unhas 2013Habi Septiati MusinNessuna valutazione finora
- AscitesDocumento31 pagineAscitesHans NatanaelNessuna valutazione finora
- Edgar Cokaliong Vs UCPB - Sealand Service Inc. Vs IACDocumento2 pagineEdgar Cokaliong Vs UCPB - Sealand Service Inc. Vs IAC001nooneNessuna valutazione finora
- BORANGDocumento33 pagineBORANGDewi WangsaNessuna valutazione finora
- Krisis Tiroid: Diagnosis Dan TatalaksanaDocumento24 pagineKrisis Tiroid: Diagnosis Dan TatalaksanaEpifani Angelina ChandraNessuna valutazione finora
- (Mantap) Slide Materi Interna-1 Batch 3 2018Documento235 pagine(Mantap) Slide Materi Interna-1 Batch 3 2018MeidyNessuna valutazione finora
- Sindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Documento68 pagineSindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Dafhina Store100% (1)
- Kegawatan Jantung - MeDocumento41 pagineKegawatan Jantung - MeNam Min BinNessuna valutazione finora
- Atrial Fibrilation (AF) : Moh Gilang Fajriansyah Nohu (C11110285)Documento38 pagineAtrial Fibrilation (AF) : Moh Gilang Fajriansyah Nohu (C11110285)GilankNessuna valutazione finora
- IV Insulin Infusion Protocol TexasDocumento2 pagineIV Insulin Infusion Protocol TexasJohb CaballeroNessuna valutazione finora
- The Treatment of The Jews of Bukovina by The Soviet and Romanian Administrations in 1940-1944 - V.SolonariDocumento32 pagineThe Treatment of The Jews of Bukovina by The Soviet and Romanian Administrations in 1940-1944 - V.SolonariMoldova.since.1359100% (2)
- 4.krisis Hipertensi IMELS 15Documento41 pagine4.krisis Hipertensi IMELS 15putusanggraNessuna valutazione finora
- SS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFDocumento34 pagineSS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFWisnu Yudho HNessuna valutazione finora
- Krisis Hipertensi IMELSDocumento43 pagineKrisis Hipertensi IMELSrinadi_aNessuna valutazione finora
- Materi 12 IMELS - Trombosis Emboli Paru, Iskemik Tungkai Akut - KritisDocumento64 pagineMateri 12 IMELS - Trombosis Emboli Paru, Iskemik Tungkai Akut - KritismaharyadyNessuna valutazione finora
- PERDICIDocumento31 paginePERDICIDeya PrastikaNessuna valutazione finora
- Sindroma Vena Cava SuperiorDocumento25 pagineSindroma Vena Cava SuperiorJinan Nailun NadaNessuna valutazione finora
- Tatalaksana Kegawatan Di UGD Dan Faskes PrimerDocumento52 pagineTatalaksana Kegawatan Di UGD Dan Faskes PrimerBudiman BahagiaNessuna valutazione finora
- Penatalaksanaan DSSDocumento29 paginePenatalaksanaan DSSTugas HeinzNessuna valutazione finora
- Cruz Vs FilipinasDocumento1 paginaCruz Vs FilipinasJan Christopher Elmido100% (1)
- Tatalaksana Krisis HipertensiDocumento38 pagineTatalaksana Krisis HipertensiDr Edi HidayatNessuna valutazione finora
- (INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Documento10 pagine(INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Yolanda FitrianiNessuna valutazione finora
- CHF FC III Ec Mitral StenosisDocumento36 pagineCHF FC III Ec Mitral Stenosisbroken18bear100% (1)
- JNC 6 Vs 7Documento2 pagineJNC 6 Vs 7Diwan AyuNessuna valutazione finora
- CVP Guided Deresuscitation in Managing Overload in Icu PDFDocumento57 pagineCVP Guided Deresuscitation in Managing Overload in Icu PDFJonathan Hamm100% (1)
- Konsensus GERD PGI PDFDocumento44 pagineKonsensus GERD PGI PDFMirza ZakaNessuna valutazione finora
- Formula Pintar IcuDocumento4 pagineFormula Pintar Icufitri renovitaNessuna valutazione finora
- Catetan Dekya Radiologi - 20190506102535Documento129 pagineCatetan Dekya Radiologi - 20190506102535BakingpancakesNessuna valutazione finora
- Stewart and Buffer Base.Documento69 pagineStewart and Buffer Base.Yohanes George100% (1)
- Eimed 2Documento6 pagineEimed 2Herik Hamzah0% (4)
- Braunwald Textbook of Cardiovascular Heart Disease 9th - CHM - 00Documento4 pagineBraunwald Textbook of Cardiovascular Heart Disease 9th - CHM - 00Teguh RahNessuna valutazione finora
- Acs TrombolitikDocumento55 pagineAcs TrombolitikDiana IswardhaniNessuna valutazione finora
- Original Research Abstract AFCC ASMIHA 2019Documento82 pagineOriginal Research Abstract AFCC ASMIHA 2019Program Studi Kardiologi100% (1)
- Protap NTG DripDocumento4 pagineProtap NTG DripAinil MardiahNessuna valutazione finora
- CHF LapsusDocumento27 pagineCHF Lapsuseno46Nessuna valutazione finora
- SDL Obat EmergencyDocumento26 pagineSDL Obat EmergencyfarhantunichiaNessuna valutazione finora
- Reguler: Periode Februari 2018Documento2 pagineReguler: Periode Februari 2018ghifarihaikal0% (1)
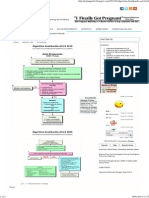
- Algorithm For Management of Acute Pulmonary Oedema PDFDocumento1 paginaAlgorithm For Management of Acute Pulmonary Oedema PDFDewi Rabiatul AkhzamiNessuna valutazione finora
- Lapsus Dr. DodyDocumento36 pagineLapsus Dr. DodyPriscilla Christina NatanNessuna valutazione finora
- Pemasangan Dan Interpretasi EKGDocumento117 paginePemasangan Dan Interpretasi EKGaulianadanisya100% (2)
- Algoritma Bradikardi AclsDocumento2 pagineAlgoritma Bradikardi AclsBangun SasongkoNessuna valutazione finora
- Hipertensi Emergensi (Herbesser)Documento41 pagineHipertensi Emergensi (Herbesser)riski novika100% (1)
- Presentasi Dr. Basuki Rachmad, Sp. An. KICDocumento39 paginePresentasi Dr. Basuki Rachmad, Sp. An. KICinstalasi kamar bedah RSMINessuna valutazione finora
- Pembahasan UKDI CLINIC 1 Batch Mei 2016Documento535 paginePembahasan UKDI CLINIC 1 Batch Mei 2016William Hartanto RusliNessuna valutazione finora
- 2 DHF InternaDocumento59 pagine2 DHF Internasaladass 2Nessuna valutazione finora
- Stemi Acute Coronary Syndrome: Dr. Muh A Sungkar, SPPD, SPJP, KKVDocumento35 pagineStemi Acute Coronary Syndrome: Dr. Muh A Sungkar, SPPD, SPJP, KKVCoass BonamNessuna valutazione finora
- Deresuscitation ARDSDocumento28 pagineDeresuscitation ARDSSudaryadiNessuna valutazione finora
- Anti Angina (Hany)Documento51 pagineAnti Angina (Hany)Angga AhadiyatNessuna valutazione finora
- Basic Life Support Perubahan Guideline AHA 2005-2010Documento22 pagineBasic Life Support Perubahan Guideline AHA 2005-2010Momoh AlkaffNessuna valutazione finora
- CPR LectureDocumento9 pagineCPR LecturejacnpoyNessuna valutazione finora
- Emergencies in MalignacyDocumento33 pagineEmergencies in MalignacyAstri Arri FebriantiNessuna valutazione finora
- Acute Kidney Injury (Aki) ImelsDocumento37 pagineAcute Kidney Injury (Aki) ImelsedoNessuna valutazione finora
- Durchschein Et Al. - 2016 - Diet Therapy For Inflammatory Bowel Diseases TheDocumento17 pagineDurchschein Et Al. - 2016 - Diet Therapy For Inflammatory Bowel Diseases TheAstri Arri FebriantiNessuna valutazione finora
- Management of Patients With Hepatitis C Infection and Renal DiseaseDocumento14 pagineManagement of Patients With Hepatitis C Infection and Renal DiseaseAstri Arri FebriantiNessuna valutazione finora
- 2016 Article 420Documento23 pagine2016 Article 420Astri Arri FebriantiNessuna valutazione finora
- Hematologic Malignancies: SMF Hematologi-Onkologi Medik Ilmu Penyakit DalamDocumento72 pagineHematologic Malignancies: SMF Hematologi-Onkologi Medik Ilmu Penyakit DalamAstri Arri FebriantiNessuna valutazione finora
- Emergencies in MalignacyDocumento33 pagineEmergencies in MalignacyAstri Arri FebriantiNessuna valutazione finora
- Flowcytometry Dna Analysis in CancerDocumento36 pagineFlowcytometry Dna Analysis in CancerAstri Arri FebriantiNessuna valutazione finora
- Winer 1Documento70 pagineWiner 1Astri Arri FebriantiNessuna valutazione finora
- Basic Principles Chemoteraphy MartinDocumento48 pagineBasic Principles Chemoteraphy MartinAstri Arri FebriantiNessuna valutazione finora
- Bodyfluids New 101020230204 Phpapp02Documento29 pagineBodyfluids New 101020230204 Phpapp02Astri Arri FebriantiNessuna valutazione finora
- Proinflammatory Cytokines (IL-6, IL-8), Cytokine Inhibitors (IL-6sR, sTNFRII) and Anti-Inflammatory Cytokines (IL-10, IL-13) in The Pathogenesis of Sepsis in Newborns and InfantsDocumento6 pagineProinflammatory Cytokines (IL-6, IL-8), Cytokine Inhibitors (IL-6sR, sTNFRII) and Anti-Inflammatory Cytokines (IL-10, IL-13) in The Pathogenesis of Sepsis in Newborns and InfantsAstri Arri FebriantiNessuna valutazione finora
- 11 Humss Challenges Encountered by Probationers in CommunityDocumento61 pagine11 Humss Challenges Encountered by Probationers in Communitycashew.3199914Nessuna valutazione finora
- UNOPS General Conditions Goods ENDocumento12 pagineUNOPS General Conditions Goods ENMohammedNessuna valutazione finora
- (CD) Aguilar vs. CA - G.R. No. 76351 - October 29, 1993 - AZapantaDocumento1 pagina(CD) Aguilar vs. CA - G.R. No. 76351 - October 29, 1993 - AZapantaAmiel Gian Mario ZapantaNessuna valutazione finora
- Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDocumento13 pagineSunday Monday Tuesday Wednesday Thursday Friday SaturdayAudrey50% (2)
- CrimDocumento1 paginaCrimEdwin VillaNessuna valutazione finora
- Bharat Sanchar Nigam Limited: Form For Fiber Based Services New Connection Companies/ Organizations IndividualsDocumento4 pagineBharat Sanchar Nigam Limited: Form For Fiber Based Services New Connection Companies/ Organizations IndividualsChander MohanNessuna valutazione finora
- New DissertationDocumento105 pagineNew Dissertationkuldeep_chand10100% (3)
- Contemporary Legal TheoriesDocumento18 pagineContemporary Legal Theoriesapi-241505258Nessuna valutazione finora
- Plaint Dissolution of MarriageDocumento3 paginePlaint Dissolution of MarriageAmina AamerNessuna valutazione finora
- PenguinDocumento4 paginePenguinAngela FernandezNessuna valutazione finora
- Barangan CtsDocumento2 pagineBarangan CtsMary Ann PateñoNessuna valutazione finora
- Report On The Amendment of The Rules of Procedure of The Parliament of UgandaDocumento46 pagineReport On The Amendment of The Rules of Procedure of The Parliament of UgandaAfrican Centre for Media ExcellenceNessuna valutazione finora
- Report of The African Court On Human and Peoples Rights in The Protection of Human Rights in Africa FinalDocumento10 pagineReport of The African Court On Human and Peoples Rights in The Protection of Human Rights in Africa FinalRANDAN SADIQNessuna valutazione finora
- Original Sin 2001 - Google SearchDocumento1 paginaOriginal Sin 2001 - Google Searchlusinda ÇullhajNessuna valutazione finora
- Airfreight 2100, Inc.Documento2 pagineAirfreight 2100, Inc.ben carlo ramos srNessuna valutazione finora
- Dap An Part 3 Mozil - Actual Test 9Documento5 pagineDap An Part 3 Mozil - Actual Test 9Đoàn Thị Thanh HoaNessuna valutazione finora
- SF2 August 11 Humss Ngilay SHSDocumento3 pagineSF2 August 11 Humss Ngilay SHSTaj NgilayNessuna valutazione finora
- 1st Test QADocumento19 pagine1st Test QAKiran AmateNessuna valutazione finora
- Hollywood Reloaded PDFDocumento16 pagineHollywood Reloaded PDFΚώσταςΣταματόπουλοςNessuna valutazione finora
- DocuDocumento105 pagineDocuKhryss Paula BaldonadoNessuna valutazione finora
- Detailed Lesson Plan Health 9Documento4 pagineDetailed Lesson Plan Health 9REA JOYNessuna valutazione finora
- Crime Scene Investigation: College of CriminologyDocumento4 pagineCrime Scene Investigation: College of CriminologyMmk CameroNessuna valutazione finora