Potrebbero piacerti anche
- Good Health in the Tropics: Advice to Travellers and SettlersDa EverandGood Health in the Tropics: Advice to Travellers and SettlersNessuna valutazione finora
- USMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsDa EverandUSMLE Step 3 Lecture Notes 2021-2022: Internal Medicine, Psychiatry, EthicsValutazione: 5 su 5 stelle5/5 (9)
- Adult ScheduleDocumento3 pagineAdult ScheduledrmanojvimalNessuna valutazione finora
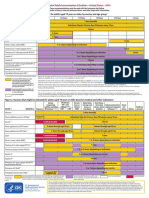
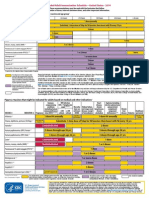
- Recommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Documento2 pagineRecommended Immunization - Canadian Immunization Guide - Seventh Edition - 2006Maja MudriNessuna valutazione finora
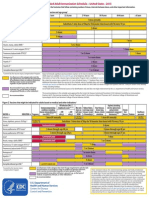
- States, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDocumento7 pagineStates, 2011 United Recommended Childhood and Adolescent Immunization SchedulesDolores KilpatrickNessuna valutazione finora
- Adult Immunization ScheduleDocumento3 pagineAdult Immunization ScheduleBryan Mae H. DegorioNessuna valutazione finora
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocumento2 pagineFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNessuna valutazione finora
- Current Presumptive Immunization SchedulesDocumento4 pagineCurrent Presumptive Immunization SchedulesPedro Julian Tenorio ApesteguiNessuna valutazione finora
- Adult Combined ScheduleDocumento5 pagineAdult Combined SchedulelcmurilloNessuna valutazione finora
- Adult Combined ScheduleDocumento5 pagineAdult Combined ScheduleAwal Safar MNessuna valutazione finora
- Indian Academy of Pediatrics (IAP) Recommended Immunization Schedule For Children Aged 0 Through 18 Years - India, 2014 and Updates On ImmunizationDocumento16 pagineIndian Academy of Pediatrics (IAP) Recommended Immunization Schedule For Children Aged 0 Through 18 Years - India, 2014 and Updates On Immunizationkrishna615Nessuna valutazione finora
- Recommend Ations: S GK, SS, S M, K C, S A, S K D, S V, A KS, S S, S K, H K P, SB, B JP, GVB, P GDocumento11 pagineRecommend Ations: S GK, SS, S M, K C, S A, S K D, S V, A KS, S S, S K, H K P, SB, B JP, GVB, P Ga hNessuna valutazione finora
- IZSchedule0 6yrsDocumento1 paginaIZSchedule0 6yrsKaty ForemanNessuna valutazione finora
- Pharmacology Assessment No. 10Documento5 paginePharmacology Assessment No. 10Joy GarciaNessuna valutazione finora
- 07 Childschd 6x4.5 1-Page PRDocumento2 pagine07 Childschd 6x4.5 1-Page PRSteluta GalbenusNessuna valutazione finora
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocumento8 pagineTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For Childrenfadityo1Nessuna valutazione finora
- Vacunas 2012Documento7 pagineVacunas 2012dr.alexisleon9124Nessuna valutazione finora
- Adult Pocafeket SizeDocumento2 pagineAdult Pocafeket SizedadfNessuna valutazione finora
- Cdi 2106 CDocumento2 pagineCdi 2106 CVerdi LeonardoNessuna valutazione finora
- PIDSP Polio Guidance 2019Documento3 paginePIDSP Polio Guidance 2019Jessica MarianoNessuna valutazione finora
- What's New On The Child and Adolescent Immunization SchedulesDocumento30 pagineWhat's New On The Child and Adolescent Immunization SchedulesMark ReinhardtNessuna valutazione finora
- The Sinovac VaccineDocumento4 pagineThe Sinovac VaccineMontasir BalambagNessuna valutazione finora
- Adult ScheduleDocumento3 pagineAdult SchedulelcmurilloNessuna valutazione finora
- Pre-Registration Nursing Information For Prospective StudentsDocumento4 paginePre-Registration Nursing Information For Prospective StudentsbthangarajNessuna valutazione finora
- Splenectomy: DisclaimerDocumento5 pagineSplenectomy: DisclaimerMimi FatinNessuna valutazione finora
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocumento7 pagineTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenKrishnendu PramanikNessuna valutazione finora
- Recommended Immunizations FS enDocumento2 pagineRecommended Immunizations FS enirfanmajeed1987Nessuna valutazione finora
- Catchup Schedule PRDocumento1 paginaCatchup Schedule PRJesus A. Pineda GarciaNessuna valutazione finora
- Atagi Recommendations On The Use of A Booster Dose of Covid 19 VaccineDocumento9 pagineAtagi Recommendations On The Use of A Booster Dose of Covid 19 VaccinenickjoshNessuna valutazione finora
- Week 4 Peer ResponseDocumento3 pagineWeek 4 Peer ResponseMayumi BalmesNessuna valutazione finora
- Immunization Routine Table1Documento9 pagineImmunization Routine Table1MeeKo VideñaNessuna valutazione finora
- Expanded Program On ImmunuzationDocumento37 pagineExpanded Program On ImmunuzationRose AnnNessuna valutazione finora
- Adult Schedule 11x17Documento2 pagineAdult Schedule 11x17lcmurilloNessuna valutazione finora
- Adult Combined ScheduleDocumento6 pagineAdult Combined ScheduleAstrid Elaine RosalesNessuna valutazione finora
- Immunization Review GPDocumento46 pagineImmunization Review GPKishore ChandkiNessuna valutazione finora
- 1 CombineDocumento726 pagine1 CombineSong Hành Vạn KiếpNessuna valutazione finora
- Community Health Nursing (Learning Feedback Diary (LFD #25)Documento3 pagineCommunity Health Nursing (Learning Feedback Diary (LFD #25)Angelica Malacay RevilNessuna valutazione finora
- Tentang PCVDocumento12 pagineTentang PCVJanuwar LukitaNessuna valutazione finora
- Adult Immunization: It's Your Best Shot!Documento40 pagineAdult Immunization: It's Your Best Shot!minerva_stanciuNessuna valutazione finora
- F1 - Frequently Asked Questions On Immunization DVLMDocumento25 pagineF1 - Frequently Asked Questions On Immunization DVLMMAHAMMAD ANWAR ALINessuna valutazione finora
- IZSchedule0 6yrsDocumento1 paginaIZSchedule0 6yrsgeany2911Nessuna valutazione finora
- 0 6yrs Schedule BWDocumento1 pagina0 6yrs Schedule BWRyan ArdyantoNessuna valutazione finora
- Office of The Secretary: Pneumococcal Conjugate Vaccines (PCV) Reassessment in The PhilippinesDocumento17 pagineOffice of The Secretary: Pneumococcal Conjugate Vaccines (PCV) Reassessment in The Philippinesbandicot21Nessuna valutazione finora
- Adult Combined Schedule VaccineDocumento33 pagineAdult Combined Schedule VaccinehatsuneNessuna valutazione finora
- WHO Immunization Schedule ChildrenDocumento9 pagineWHO Immunization Schedule Childrenashchua21Nessuna valutazione finora
- Immunization EPI Huda 201212Documento5 pagineImmunization EPI Huda 201212Aerish TupazNessuna valutazione finora
- Document From DR Abhay ShahDocumento20 pagineDocument From DR Abhay ShahRavikiran SuryanarayanamurthyNessuna valutazione finora
- Routine Schedule of ImmunizationDocumento3 pagineRoutine Schedule of ImmunizationIvyNessuna valutazione finora
- Binational Schedule Immunization USA MEXICODocumento2 pagineBinational Schedule Immunization USA MEXICOfernando_morales_15Nessuna valutazione finora
- Vaccinations For Preteens and Teens, Age 11-19 Years: Vaccine Do You Need It?Documento1 paginaVaccinations For Preteens and Teens, Age 11-19 Years: Vaccine Do You Need It?Phan303Nessuna valutazione finora
- Pneumococcal Conjugate: VaccineDocumento2 paginePneumococcal Conjugate: VaccineJenny TaylorNessuna valutazione finora
- Over-All Goal: To Reduce The Morbidity and Mortality Among Children Against The Most Common Vaccine-Preventable Diseases. Specific GoalDocumento9 pagineOver-All Goal: To Reduce The Morbidity and Mortality Among Children Against The Most Common Vaccine-Preventable Diseases. Specific GoalMark Raymunstine TamposNessuna valutazione finora
- World Immunization Week 2023 PPA EPIDocumento42 pagineWorld Immunization Week 2023 PPA EPIMuhammad ShafiNessuna valutazione finora
- Expanded Program For Immunization CHD ReportDocumento12 pagineExpanded Program For Immunization CHD ReportCristalPagcaliwangan0% (1)
- Recommended Immunization Schedule For Persons Aged 0-6 YearsDocumento3 pagineRecommended Immunization Schedule For Persons Aged 0-6 YearsAlvaro FloresNessuna valutazione finora
- WHO 2019 NCoV Vaccines SAGE Recommendation Sinovac CoronaVac 2021.1 EngDocumento7 pagineWHO 2019 NCoV Vaccines SAGE Recommendation Sinovac CoronaVac 2021.1 EngMartha Gatica GuevaraNessuna valutazione finora
- Expanded Program On ImmunizationDocumento4 pagineExpanded Program On ImmunizationJUANJOSEFOXNessuna valutazione finora
- Immunisation ScheduleDocumento3 pagineImmunisation SchedulejegathesmsjsNessuna valutazione finora
- The Routine Immunisation ScheduleDocumento10 pagineThe Routine Immunisation ScheduleJamesWaitonNessuna valutazione finora
- Vaccinations For Infants and Children, Age 0-10 Years: Vaccine Is Your Child Up To Date?Documento1 paginaVaccinations For Infants and Children, Age 0-10 Years: Vaccine Is Your Child Up To Date?mailraffiqNessuna valutazione finora
- IZZ - PiodermaDocumento51 pagineIZZ - PiodermavivilmNessuna valutazione finora
- TaeniasisDocumento23 pagineTaeniasisMardoni Efrijon33% (3)
- Sti WorksheetDocumento2 pagineSti Worksheetapi-401570635Nessuna valutazione finora
- Hepatitis Serology Cheat SheetDocumento4 pagineHepatitis Serology Cheat SheetNi Putu YPNessuna valutazione finora
- Systemic Lupus Erythematosus: XXX DCEM2 Toulouse Purpan Medical School January 7 2009Documento3 pagineSystemic Lupus Erythematosus: XXX DCEM2 Toulouse Purpan Medical School January 7 2009Bren OlivaNessuna valutazione finora
- Histo Lab Exercise #12Documento8 pagineHisto Lab Exercise #12Gela ReyesNessuna valutazione finora
- Antibiotics Khan AcademyDocumento4 pagineAntibiotics Khan AcademyZaina ImamNessuna valutazione finora
- Lesson 7Documento56 pagineLesson 7Keddie OneJhereNessuna valutazione finora
- Childrens FBC Reference Ranges PDFDocumento1 paginaChildrens FBC Reference Ranges PDFmfaddhilNessuna valutazione finora
- Keratitis PPT 1 SUB ENGLISHDocumento33 pagineKeratitis PPT 1 SUB ENGLISHarif rhNessuna valutazione finora
- Antistreptolysin o (Aso) Latex Slide TestDocumento5 pagineAntistreptolysin o (Aso) Latex Slide Testkiedd_04100% (1)
- Role of Antibiotics in Orthopedic InfectionsDocumento31 pagineRole of Antibiotics in Orthopedic InfectionsRakesh KumarNessuna valutazione finora
- Physician Certification FormDocumento2 paginePhysician Certification FormSachin Tukaram SalianNessuna valutazione finora
- Authors: Ibel Carri, María Marcela Barrio, Morten Nielsen: BackgroundDocumento1 paginaAuthors: Ibel Carri, María Marcela Barrio, Morten Nielsen: BackgroundrexNessuna valutazione finora
- 05 .Emerging and Re-Emerging - Covid - 19Documento43 pagine05 .Emerging and Re-Emerging - Covid - 19fajarNessuna valutazione finora
- SHE Assignment - Disease X Outbreak (Year 11)Documento5 pagineSHE Assignment - Disease X Outbreak (Year 11)Mary Elizabeth ValmoresNessuna valutazione finora
- (BMED66) HUMAN ANATOMY & PHYSIOLOGY WITH PATHOPHYSIOLOGY Laboratory Lecture The Lymphatic System Lesson 12Documento13 pagine(BMED66) HUMAN ANATOMY & PHYSIOLOGY WITH PATHOPHYSIOLOGY Laboratory Lecture The Lymphatic System Lesson 12Cerisse MaeNessuna valutazione finora
- What Is A Bone Marrow Transplant?Documento4 pagineWhat Is A Bone Marrow Transplant?Krisna AgustiniNessuna valutazione finora
- Soybean Glycine Max Allergy in Europe Gly M 5 Conglycinin and Gly M 6 Glycinin Are Potential Diagnostic Markers For Severe Allergic Reactions To Soy 2009 Journal of Allergy and CliDocumento11 pagineSoybean Glycine Max Allergy in Europe Gly M 5 Conglycinin and Gly M 6 Glycinin Are Potential Diagnostic Markers For Severe Allergic Reactions To Soy 2009 Journal of Allergy and CliDiva Silva FirminoNessuna valutazione finora
- Dermatology For The Small Animal PractitionerDocumento145 pagineDermatology For The Small Animal Practitionerсветлана бугаева100% (5)
- Rothia Mucilaginosa Is An Anti Inflammatory Bacterium in The Respiratory Tract of Patients With Chronic Lung DiseaseDocumento16 pagineRothia Mucilaginosa Is An Anti Inflammatory Bacterium in The Respiratory Tract of Patients With Chronic Lung DiseaseJan Xyrene DelloroNessuna valutazione finora
- 1 LeukopoiesisDocumento23 pagine1 LeukopoiesisJan Victor Elico100% (3)
- Department of Genetics: Covid-19 RT PCRDocumento1 paginaDepartment of Genetics: Covid-19 RT PCRMuhammed HadhiNessuna valutazione finora
- Obtained Value: Clinical Biochemistry Test Name Units Bio. Ref. Intervals (Age/Gender Specific) MethodDocumento1 paginaObtained Value: Clinical Biochemistry Test Name Units Bio. Ref. Intervals (Age/Gender Specific) MethodHarshit AmbeshNessuna valutazione finora
- CAP Accreditation Checklists - 2021 Edition: Checklists Subdisciplines Description of ContentsDocumento7 pagineCAP Accreditation Checklists - 2021 Edition: Checklists Subdisciplines Description of ContentsMARGITNessuna valutazione finora
- One Health: SciencedirectDocumento11 pagineOne Health: SciencedirectIsabella GriffithNessuna valutazione finora
- TB Flipchart RSDocumento30 pagineTB Flipchart RSMuhammad Hasbul100% (1)
- Pulmonary Tuberculosis 2016Documento17 paginePulmonary Tuberculosis 2016Nikka Moreen Dagdag100% (1)
- G VirusesDocumento334 pagineG VirusesLuana NicolaNessuna valutazione finora
- Public Health UnitDocumento2 paginePublic Health UnitMark Emil BautistaNessuna valutazione finora