Potrebbero piacerti anche
- 4th Sem 651 Occupational ProfileDocumento19 pagine4th Sem 651 Occupational Profileapi-291545292100% (1)
- Occt630 Occupational Profile InterventionDocumento19 pagineOcct630 Occupational Profile Interventionapi-290880850Nessuna valutazione finora
- 630 Occupational Profile AssignmentDocumento13 pagine630 Occupational Profile Assignmentapi-201999002Nessuna valutazione finora
- 630 Submitted Occupational Profile and AnalysisDocumento21 pagine630 Submitted Occupational Profile and Analysisapi-310815315Nessuna valutazione finora
- Occupational Profile and Analysis Final EditedDocumento14 pagineOccupational Profile and Analysis Final Editedapi-233645719Nessuna valutazione finora
- Occt 651 - Occupational Profile PaperDocumento20 pagineOcct 651 - Occupational Profile Paperapi-293243330Nessuna valutazione finora
- New Intervention PlanDocumento17 pagineNew Intervention Planapi-282753416Nessuna valutazione finora
- Kristen Kincaid Occupational Analysis & Intervention PlanDocumento23 pagineKristen Kincaid Occupational Analysis & Intervention Planapi-282525755100% (1)
- Immuno Part CsDocumento15 pagineImmuno Part CsCecilia TesoreroNessuna valutazione finora
- Social Worker or Caesmanager or Mental Health CounselorDocumento3 pagineSocial Worker or Caesmanager or Mental Health Counselorapi-77565760Nessuna valutazione finora
- Initial TemplateDocumento8 pagineInitial TemplateZuj PayNessuna valutazione finora
- CC StrokeDocumento13 pagineCC Strokeapi-436090845100% (1)
- Occupational Profile and Intervention PlanDocumento18 pagineOccupational Profile and Intervention Planapi-282525755Nessuna valutazione finora
- Dickson Occupational ProfileDocumento18 pagineDickson Occupational Profileapi-255001706Nessuna valutazione finora
- Occupational Profile M Viveros FinalDocumento19 pagineOccupational Profile M Viveros Finalapi-293258738Nessuna valutazione finora
- Occt 651 - Occupational Profile and Intervention PlanDocumento22 pagineOcct 651 - Occupational Profile and Intervention Planapi-279916752Nessuna valutazione finora
- Occupational Analysis Intervention Plan PDFDocumento20 pagineOccupational Analysis Intervention Plan PDFapi-293182319Nessuna valutazione finora
- Eval Soap Note 2Documento9 pagineEval Soap Note 2api-435763096Nessuna valutazione finora
- Artifact 5 Soap NoteDocumento3 pagineArtifact 5 Soap Noteapi-517998988Nessuna valutazione finora
- Dick, Elisa - Occupational ProfileDocumento10 pagineDick, Elisa - Occupational Profileapi-234536968Nessuna valutazione finora
- Occupational Profile Intervention PlanDocumento17 pagineOccupational Profile Intervention Planapi-264481356Nessuna valutazione finora
- Soap NoteDocumento2 pagineSoap Noteapi-285542134Nessuna valutazione finora
- Occt 630 - Occupational Profile and Intervention Plan - PortfolioDocumento21 pagineOcct 630 - Occupational Profile and Intervention Plan - Portfolioapi-279916752Nessuna valutazione finora
- Artfact 3 Occupational Therapy Discharge SummaryDocumento4 pagineArtfact 3 Occupational Therapy Discharge Summaryapi-517998988Nessuna valutazione finora
- Community Client Discharge SummaryDocumento3 pagineCommunity Client Discharge Summaryapi-271980676Nessuna valutazione finora
- Critique Form For Critical Appraisal Students Name: - Date: - DirectionsDocumento6 pagineCritique Form For Critical Appraisal Students Name: - Date: - DirectionsEsther BrooksNessuna valutazione finora
- Case Study Paper FinalDocumento19 pagineCase Study Paper Finalapi-240832658Nessuna valutazione finora
- Occupational Profile & Intervention PlanDocumento20 pagineOccupational Profile & Intervention Planapi-262531856Nessuna valutazione finora
- Soap 11Documento4 pagineSoap 11api-436429414Nessuna valutazione finora
- NHM 340 Writing Assignment 2Documento3 pagineNHM 340 Writing Assignment 2api-309055256Nessuna valutazione finora
- Discharge ReportDocumento3 pagineDischarge Reportapi-383274221Nessuna valutazione finora
- Ashley M Occt 651 Occupational ProfileDocumento11 pagineAshley M Occt 651 Occupational Profileapi-25080062950% (2)
- Ebp PaperDocumento16 pagineEbp Paperapi-583545759Nessuna valutazione finora
- StrokeDocumento5 pagineStrokeapi-261670650Nessuna valutazione finora
- Position Paper OT For People With LDDocumento10 paginePosition Paper OT For People With LDLytiana WilliamsNessuna valutazione finora
- Case Map #7 Documentation PDFDocumento15 pagineCase Map #7 Documentation PDFSarah LaytonNessuna valutazione finora
- Strategies Used by Occupational Therapy To Maximize ADL IndependenceDocumento53 pagineStrategies Used by Occupational Therapy To Maximize ADL IndependenceNizam lotfiNessuna valutazione finora
- Fieldwork Case Study Treatment Plan AssignmentDocumento11 pagineFieldwork Case Study Treatment Plan Assignmentapi-398892840Nessuna valutazione finora
- Occupation Analysis in PracticeDa EverandOccupation Analysis in PracticeLynette MackenzieNessuna valutazione finora
- Occupational Identity Disruption After Traumatic Brain Injury - An Approach To Occupational Therapy Evaluation and TreatmentDocumento13 pagineOccupational Identity Disruption After Traumatic Brain Injury - An Approach To Occupational Therapy Evaluation and Treatmentapi-234120429Nessuna valutazione finora
- Self Assessment PDT 2 1Documento1 paginaSelf Assessment PDT 2 1api-518497061Nessuna valutazione finora
- Hazley Jarrett Jordan-Final Cimt Systematic Review AltDocumento14 pagineHazley Jarrett Jordan-Final Cimt Systematic Review Altapi-518986604Nessuna valutazione finora
- Soap NoteDocumento1 paginaSoap Noteapi-519577267Nessuna valutazione finora
- Occupational TherapyDocumento5 pagineOccupational TherapyZahra IffahNessuna valutazione finora
- Occupations Profile & Intervention PlanDocumento20 pagineOccupations Profile & Intervention Planapi-282223043Nessuna valutazione finora
- Cognitive Decline And/orDocumento17 pagineCognitive Decline And/orDinusha Saminda SirisenaNessuna valutazione finora
- MOHOST InformationDocumento1 paginaMOHOST InformationRichard FullertonNessuna valutazione finora
- Occupational AdaptationDocumento5 pagineOccupational AdaptationVASH12345100% (1)
- Ota Group ProtocolDocumento26 pagineOta Group Protocolapi-318685839Nessuna valutazione finora
- Occupational JusticeDocumento4 pagineOccupational JusticeHardeep Singh BaliNessuna valutazione finora
- Occupational Therapy and Mental Health 1Documento18 pagineOccupational Therapy and Mental Health 1Roman -Nessuna valutazione finora
- Home Environmental AssessmentDocumento2 pagineHome Environmental AssessmentSelvi Puspa SariNessuna valutazione finora
- Soap Discharge 8 1Documento2 pagineSoap Discharge 8 1api-436040430Nessuna valutazione finora
- Wrist Hand OrthosisDocumento3 pagineWrist Hand OrthosisKhageswar SamalNessuna valutazione finora
- Occupational Profile Intervention Plan-Danielle PalmerDocumento20 pagineOccupational Profile Intervention Plan-Danielle Palmerapi-292894327Nessuna valutazione finora
- Occupations Across The LifespanDocumento6 pagineOccupations Across The LifespanMary Elizabeth JoyceNessuna valutazione finora
- Aus Occup Therapy J - 2002 - Wilcock - Reflections On Doing Being and BecomingDocumento11 pagineAus Occup Therapy J - 2002 - Wilcock - Reflections On Doing Being and BecomingMelissa CroukampNessuna valutazione finora
- Occupation in Occupational Therapy PDFDocumento26 pagineOccupation in Occupational Therapy PDFa_tobarNessuna valutazione finora
- Instrumental Activities Daily Living: Try ThisDocumento11 pagineInstrumental Activities Daily Living: Try ThisbalryoNessuna valutazione finora
- Babcock HomeassessmentDocumento8 pagineBabcock Homeassessmentapi-238107777Nessuna valutazione finora
- Babcock&perea Evidence PaperDocumento9 pagineBabcock&perea Evidence Paperapi-238107777Nessuna valutazione finora
- Running Head: Qualitative Research Paper 1Documento12 pagineRunning Head: Qualitative Research Paper 1api-238107777Nessuna valutazione finora
- Case Study 1Documento16 pagineCase Study 1api-238107777Nessuna valutazione finora
- Effects of Anxiety LevelsDocumento9 pagineEffects of Anxiety Levelsapi-238107777Nessuna valutazione finora
- Babcock ResumeDocumento2 pagineBabcock Resumeapi-238107777Nessuna valutazione finora
- PTSD PresentationDocumento26 paginePTSD Presentationapi-238107777100% (1)
- FW 2 AevalDocumento6 pagineFW 2 Aevalapi-238107777Nessuna valutazione finora
- 2 Bone Growth and DevelopmentDocumento76 pagine2 Bone Growth and DevelopmentEman AhmadNessuna valutazione finora
- Safety Measures in Using Farm Tools According To Job RequirementDocumento2 pagineSafety Measures in Using Farm Tools According To Job RequirementJan IcejimenezNessuna valutazione finora
- ISMT12 - Day 112 - Fardhian - Physical and Neurologic ExaminationDocumento26 pagineISMT12 - Day 112 - Fardhian - Physical and Neurologic Examinationbosnia agusNessuna valutazione finora
- Gage-Planaria LabDocumento4 pagineGage-Planaria Labapi-407905262Nessuna valutazione finora
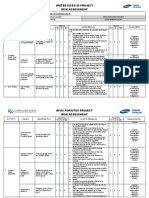
- Apoc Risk Assessment Format - Sesa-Bfim-Ra-Cs-001Documento11 pagineApoc Risk Assessment Format - Sesa-Bfim-Ra-Cs-001Abdul WasayNessuna valutazione finora
- Neurosurgery Report Tuesday, January 11, 2022: Penanggung Jawab MandiriDocumento66 pagineNeurosurgery Report Tuesday, January 11, 2022: Penanggung Jawab MandiribobirfansyahputraNessuna valutazione finora
- Analysis of Posture - 3rd Sem PDFDocumento112 pagineAnalysis of Posture - 3rd Sem PDFShibila ShirinNessuna valutazione finora
- Win BackDocumento15 pagineWin BackrekadarkoNessuna valutazione finora
- Professional Meeting Reflection - GracDocumento3 pagineProfessional Meeting Reflection - Gracapi-540011183Nessuna valutazione finora
- Block FigureDocumento9 pagineBlock FigureTarun MehrotraNessuna valutazione finora
- Fracture of PatellaDocumento22 pagineFracture of Patellaabdul azizNessuna valutazione finora
- Booklet Intermediate 2023Documento129 pagineBooklet Intermediate 2023Rosario SassiNessuna valutazione finora
- First AidDocumento48 pagineFirst AidshodhanNessuna valutazione finora
- Musculos ParaproteticosDocumento63 pagineMusculos Paraproteticosestefania100% (2)
- The Lucky One ChordsDocumento3 pagineThe Lucky One ChordshardiangkaNessuna valutazione finora
- Autologous Platelet-Rich Plasma inDocumento6 pagineAutologous Platelet-Rich Plasma innoor hidayahNessuna valutazione finora
- HUBS1105 Glenohumeral Joint and Muscles of The Shoulder Region Lectures CombinedDocumento7 pagineHUBS1105 Glenohumeral Joint and Muscles of The Shoulder Region Lectures CombinedChloe HeuchanNessuna valutazione finora
- 6 Page Example Pitch ReportDocumento7 pagine6 Page Example Pitch ReportFrank Colabella IIINessuna valutazione finora
- Blue Book SampleDocumento8 pagineBlue Book Sampleemme_lopez9081100% (3)
- ScoliosisDocumento18 pagineScoliosisMj EnofnaNessuna valutazione finora
- Anatomy Trains OverviewDocumento20 pagineAnatomy Trains OverviewDennis Chiu Mee100% (5)
- Gravaboi Codes and NumbersDocumento18 pagineGravaboi Codes and NumbersHenrii Arias0% (1)
- PMR2014Documento122 paginePMR2014Jacob DoughertyNessuna valutazione finora
- Basic First Aid PWR Point PresentationDocumento38 pagineBasic First Aid PWR Point PresentationFiras Azrul AffendyNessuna valutazione finora
- Home Safety ChecklistDocumento4 pagineHome Safety Checklistapi-316177677Nessuna valutazione finora
- TCCC Handbook Fall 2013Documento192 pagineTCCC Handbook Fall 2013AMG_IA100% (4)
- HemophiliaDocumento20 pagineHemophiliamuhirwa SamuelNessuna valutazione finora
- AO Trauma Course - Basic Principles of Fracture Management Syllabus For FacultyDocumento27 pagineAO Trauma Course - Basic Principles of Fracture Management Syllabus For FacultyPablo GerardoNessuna valutazione finora
- Ma Gui Ba Gua Sample Exercise DocumentDocumento14 pagineMa Gui Ba Gua Sample Exercise Documentshmoopiebear50% (2)
- Hobbs News-SunDocumento1 paginaHobbs News-SunRob NikolewskiNessuna valutazione finora