Potrebbero piacerti anche
- Book List PDFDocumento6 pagineBook List PDFRowena Furog Baduya EmpanadoNessuna valutazione finora
- DepEd Presentation On K To 12 - HandoutDocumento29 pagineDepEd Presentation On K To 12 - HandoutKhristine Tan0% (1)
- Learning Readiness TestDocumento7 pagineLearning Readiness TestJonathan Araya100% (1)
- Short Stories - PrintDocumento6 pagineShort Stories - PrintNasreen HakimNessuna valutazione finora
- Kindergarten Name Writing-RubricDocumento2 pagineKindergarten Name Writing-Rubricapi-300158509Nessuna valutazione finora
- Position Paper Standardized TestingDocumento2 paginePosition Paper Standardized Testingapi-307248240Nessuna valutazione finora
- Bullying in The ClassroomDocumento12 pagineBullying in The ClassroomCj ReyesNessuna valutazione finora
- Teenage-Parent Relationship WorksheetDocumento11 pagineTeenage-Parent Relationship WorksheetJayRAj67% (3)
- G2Q3 - ENG - Animal Band and The Bird Flies - 033016 - FINALDocumento20 pagineG2Q3 - ENG - Animal Band and The Bird Flies - 033016 - FINALMee Ling AcederaNessuna valutazione finora
- SPED - Non-Graded (Primary Level II) Mathematics Q4 - W4Documento10 pagineSPED - Non-Graded (Primary Level II) Mathematics Q4 - W4Eat Pray WorkNessuna valutazione finora
- Course 1Documento59 pagineCourse 1Leilani BacayNessuna valutazione finora
- Item Analysis 2nd Quarter Gr. 32018-2019Documento42 pagineItem Analysis 2nd Quarter Gr. 32018-2019Jenalyn Talosa Nicolas UrmanitaNessuna valutazione finora
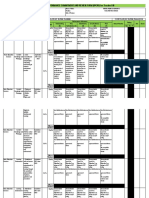
- Contextualized-Assessment-Tool-in-English-6-Fourth-Quarter - Mangino-Elementary-School (Revised)Documento11 pagineContextualized-Assessment-Tool-in-English-6-Fourth-Quarter - Mangino-Elementary-School (Revised)Ma'am Lenna PaguioNessuna valutazione finora
- MELC Kinder toSHSDocumento579 pagineMELC Kinder toSHSFerdie TarayaNessuna valutazione finora
- English Lesson Plans For Grade 2: Lessons in This SectionDocumento14 pagineEnglish Lesson Plans For Grade 2: Lessons in This SectionBane LazoNessuna valutazione finora
- Sample Puppet Child Scripts 4 9 20Documento8 pagineSample Puppet Child Scripts 4 9 20saadhana elangovanNessuna valutazione finora
- Region Memo Asd 16 Reinforcement of Guidelines and Process Flow On Reclassification of Teaching PersonnelDocumento7 pagineRegion Memo Asd 16 Reinforcement of Guidelines and Process Flow On Reclassification of Teaching PersonnelJuan LorenzoNessuna valutazione finora
- Family Resources and Needs and Sources of Family IncomeDocumento12 pagineFamily Resources and Needs and Sources of Family IncomeGenalyn Tambiao AchanzarNessuna valutazione finora
- DLL Mapeh 6 Whole YearDocumento154 pagineDLL Mapeh 6 Whole YearJordan Cruz100% (1)
- Task 1 (Reflective Journal Entry No. 2)Documento1 paginaTask 1 (Reflective Journal Entry No. 2)bernadeth alvarezNessuna valutazione finora
- Mathematics G6 Activity Sheets Q1 W1Documento11 pagineMathematics G6 Activity Sheets Q1 W1Dharl Carrera CatungalNessuna valutazione finora
- Kindergarten Homeroom GuidanceDocumento2 pagineKindergarten Homeroom GuidanceBeth Gomez LiwagNessuna valutazione finora
- Kindergarten Lesson Plan Week 7Documento29 pagineKindergarten Lesson Plan Week 7Ronalyn Rodriguez0% (1)
- English 2 Q2 FDocumento46 pagineEnglish 2 Q2 FMichelle BandalesNessuna valutazione finora
- Individual Performance Commitment and Review Form (Ipcrf) For Teacher I-IiiDocumento8 pagineIndividual Performance Commitment and Review Form (Ipcrf) For Teacher I-IiiAPO-BARLIN ALUMNI ASSOCIATIONNessuna valutazione finora
- AP 3 Summative Test 1st GradingDocumento5 pagineAP 3 Summative Test 1st GradingERLYN DELOS SANTOS100% (1)
- Products of 3 Digit Numbers by 2 Digit Week 2 L1Documento14 pagineProducts of 3 Digit Numbers by 2 Digit Week 2 L1CitieNessuna valutazione finora
- English3 q2 Mod9 YouSpell v2Documento23 pagineEnglish3 q2 Mod9 YouSpell v2Karrel Joy Dela CruzNessuna valutazione finora
- Republic of The Philippines Department of Education: Region Xiii-Caraga Schools Division of Agusan Del NorteDocumento2 pagineRepublic of The Philippines Department of Education: Region Xiii-Caraga Schools Division of Agusan Del NorteChrisnaliam FelisildaNessuna valutazione finora
- SPED Thesis SLUDocumento9 pagineSPED Thesis SLUremegelbristolNessuna valutazione finora
- Grade 4 English Most Essential Learning Competencies MELCsDocumento4 pagineGrade 4 English Most Essential Learning Competencies MELCsminguin myouiNessuna valutazione finora
- The Domains of Literacy: Beginning Reading Stage: Felicitas E. Pado, PHDDocumento40 pagineThe Domains of Literacy: Beginning Reading Stage: Felicitas E. Pado, PHDRhea AcupidoNessuna valutazione finora
- Article X - THE TEACHERS & BUSINESSDocumento5 pagineArticle X - THE TEACHERS & BUSINESSAngela ReverezaNessuna valutazione finora
- CARREER SKILLS PACKAGE - DOs21Documento6 pagineCARREER SKILLS PACKAGE - DOs21MA Vic100% (1)
- Chapter IV-Principles and Conditions of Learning and The CurriculumDocumento9 pagineChapter IV-Principles and Conditions of Learning and The CurriculumJennifer PagatpatanNessuna valutazione finora
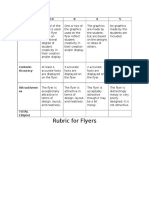
- Flyer RubricDocumento1 paginaFlyer Rubricapi-310819642Nessuna valutazione finora
- Passed 678-13-21MELCS Apayao Ang Mga Simbolo at Sagisag NG Mga Lalawigan at Lungsod Sa Sariling RehiyonDocumento30 paginePassed 678-13-21MELCS Apayao Ang Mga Simbolo at Sagisag NG Mga Lalawigan at Lungsod Sa Sariling Rehiyonjsvilla22Nessuna valutazione finora
- Rubrics of Awards2Documento9 pagineRubrics of Awards2Jared AlexanderNessuna valutazione finora
- Color Your InterestsDocumento2 pagineColor Your InterestsMyrrh Tagurigan Train100% (1)
- Grade 3 - Science Grade 6: MAPEH (P.E.)Documento40 pagineGrade 3 - Science Grade 6: MAPEH (P.E.)Jm magoNessuna valutazione finora
- Module 1 Lesson1Documento21 pagineModule 1 Lesson1Ricardo S.BlancoNessuna valutazione finora
- Learning Management Plan For Carly Seda 2014Documento3 pagineLearning Management Plan For Carly Seda 2014api-298785195Nessuna valutazione finora
- Study Notebook Module 2 TINAROSE IA O. DE GUZMANDocumento10 pagineStudy Notebook Module 2 TINAROSE IA O. DE GUZMANRames Ely GJNessuna valutazione finora
- Child 210 SyllabusDocumento3 pagineChild 210 Syllabusapi-518483960Nessuna valutazione finora
- Kindergarten DLL MELC Q1 Week 5 AsfDocumento7 pagineKindergarten DLL MELC Q1 Week 5 AsfireenNessuna valutazione finora
- Models of Technology-Enhanced Instructional LessonsDocumento17 pagineModels of Technology-Enhanced Instructional LessonsRexson Dela Cruz Taguba0% (1)
- Lesson 6 Foundations of Curriculum DevelopmentDocumento30 pagineLesson 6 Foundations of Curriculum DevelopmentLecel MartinezNessuna valutazione finora
- Week 1 - 1st & 2nd DayDocumento2 pagineWeek 1 - 1st & 2nd DayNorhana SamadNessuna valutazione finora
- Banghay Kabanata 7 Suyuan Sa AsoteaDocumento2 pagineBanghay Kabanata 7 Suyuan Sa AsoteamaricelNessuna valutazione finora
- English: Quarter 1Documento40 pagineEnglish: Quarter 1Cynthia Marie Besa100% (1)
- Survey QuestionnaireDocumento1 paginaSurvey QuestionnaireRoland Paolo DiloyNessuna valutazione finora
- Reflection On Gifted and Talented in The First GradeDocumento5 pagineReflection On Gifted and Talented in The First Gradeapi-357042891Nessuna valutazione finora
- Finland vs. PhilippinesDocumento5 pagineFinland vs. PhilippinesFaith Joyrish DelgadoNessuna valutazione finora
- Kindergarten DLL Week 30Documento4 pagineKindergarten DLL Week 30jimmyboyjr100% (1)
- Lesson Plan For English Grade V Using Explicit InstructionDocumento3 pagineLesson Plan For English Grade V Using Explicit InstructionJune-Mark CruzNessuna valutazione finora
- Sworn Statement: Republic of The Philippines Department of Education Region VDocumento1 paginaSworn Statement: Republic of The Philippines Department of Education Region VDanilo LicupNessuna valutazione finora
- School Forms Checking Report TEMPLATEDocumento7 pagineSchool Forms Checking Report TEMPLATEjoan tomarong100% (1)
- Matrix of Curriculum Standards (Competencies), With Corresponding Recommended Flexible Learning Delivery Mode and Materials Per Grading PeriodDocumento3 pagineMatrix of Curriculum Standards (Competencies), With Corresponding Recommended Flexible Learning Delivery Mode and Materials Per Grading PeriodEvan Maagad LutchaNessuna valutazione finora
- Subject: ED 200 Subject Description: EDUCATIONAL PHILOSOPHYDocumento3 pagineSubject: ED 200 Subject Description: EDUCATIONAL PHILOSOPHYRichie MacasarteNessuna valutazione finora
- Immreq15 16Documento2 pagineImmreq15 16api-234991765Nessuna valutazione finora
- Summary of Recommendations For Adult Immunization: (Age 19 Years and Older)Documento5 pagineSummary of Recommendations For Adult Immunization: (Age 19 Years and Older)Hannah Caburian RemoNessuna valutazione finora
- Math ExponentsDocumento6 pagineMath ExponentsJayRAjNessuna valutazione finora
- WorksheetsDocumento69 pagineWorksheetsJayRAjNessuna valutazione finora
- Unit 2 - Ecosystems - Assessment PacketDocumento21 pagineUnit 2 - Ecosystems - Assessment PacketJayRAjNessuna valutazione finora
- Learning Styles WorksheetDocumento13 pagineLearning Styles WorksheetJayRAjNessuna valutazione finora
- Classical Conditioning WorksheetDocumento4 pagineClassical Conditioning WorksheetJayRAjNessuna valutazione finora
- The Brain and Learning WorksheetDocumento5 pagineThe Brain and Learning WorksheetJayRAjNessuna valutazione finora
- EPA For Kids Worksheet - Module 1 - Unit 1: NameDocumento1 paginaEPA For Kids Worksheet - Module 1 - Unit 1: NameJayRAjNessuna valutazione finora