Potrebbero piacerti anche
- Ada Aha Management of Dental Problems in PX With Cardiovascular Disease 1964Documento10 pagineAda Aha Management of Dental Problems in PX With Cardiovascular Disease 1964api-265532519Nessuna valutazione finora
- Ada Aha Management of Dental Problems in PX With Cardiovascular Disease 1964Documento10 pagineAda Aha Management of Dental Problems in PX With Cardiovascular Disease 1964api-265532519Nessuna valutazione finora
- Composition and Functions: BloodDocumento86 pagineComposition and Functions: BloodYeyeh SantosNessuna valutazione finora
- 1-2 Hemostasis PhysiologyDocumento48 pagine1-2 Hemostasis PhysiologyHussein Al Saedi100% (2)
- Dental Trauma Guidelines II Avulsion - Flores Anderson AndreassenDocumento7 pagineDental Trauma Guidelines II Avulsion - Flores Anderson Andreassenapi-265532519Nessuna valutazione finora
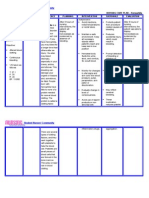
- NURSING CARE PLAN - HemophiliaDocumento2 pagineNURSING CARE PLAN - Hemophiliaderic91% (11)
- Hemostasis, Hemorrhagic Disorders and ThrombosisDocumento114 pagineHemostasis, Hemorrhagic Disorders and ThrombosisZeeNessuna valutazione finora
- Hemostasis, Clotting Disorder and AnticoagulantsDocumento87 pagineHemostasis, Clotting Disorder and AnticoagulantsSomit Jain100% (1)
- Dental Trauma Guidelines I Fractures and Luxations - Flores Anderson AndreassenDocumento6 pagineDental Trauma Guidelines I Fractures and Luxations - Flores Anderson Andreassenapi-265532519Nessuna valutazione finora
- Hemostasis: The Big PictureDocumento23 pagineHemostasis: The Big PictureJoce Maripangui100% (1)
- Perioperative Laboratorytesting - The ClinicsDocumento6 paginePerioperative Laboratorytesting - The Clinicsapi-265532519Nessuna valutazione finora
- ThrombosisDocumento15 pagineThrombosisMichelle HutahurukNessuna valutazione finora
- Biology of HemostasisDocumento20 pagineBiology of HemostasisVeronica TomaselloNessuna valutazione finora
- Saudi Council Exams For Laboratory TechnologistDocumento33 pagineSaudi Council Exams For Laboratory TechnologistMhmd Abdel-Ghany92% (36)
- Disseminated Intravascular CoagulationDocumento37 pagineDisseminated Intravascular CoagulationhipoclaudioNessuna valutazione finora
- HemophiliaDocumento27 pagineHemophiliaDorothy Pearl Loyola Palabrica100% (1)
- Blood MCQ New 5Documento21 pagineBlood MCQ New 5Omar HNessuna valutazione finora
- Model SOP for PlasmapheresisDocumento13 pagineModel SOP for PlasmapheresisBALAJI100% (1)
- Evaluation of Third MolarsDocumento6 pagineEvaluation of Third Molarsapi-265532519Nessuna valutazione finora
- Stroke: Dr. Fidha Rahmayani, M.SC, SP.S Fakultas Kedokteran Universitas Lampung RS Abdul MulukDocumento45 pagineStroke: Dr. Fidha Rahmayani, M.SC, SP.S Fakultas Kedokteran Universitas Lampung RS Abdul Mulukdhea nadhiaNessuna valutazione finora
- Understanding the Mechanism of HemostasisDocumento7 pagineUnderstanding the Mechanism of HemostasisArmella AzzahraNessuna valutazione finora
- Bleeding Disorder: HaemostasisDocumento15 pagineBleeding Disorder: Haemostasisجعفر عباس سعد عليNessuna valutazione finora
- Essentials of Anticoagulation in Hemodialysis: Core CurriculumDocumento12 pagineEssentials of Anticoagulation in Hemodialysis: Core CurriculumKavidu KeshanNessuna valutazione finora
- Disorders of HaemostasisDocumento4 pagineDisorders of HaemostasisdeblackaNessuna valutazione finora
- HEMOSTASIS AND COAGULATION PATHWAYSDocumento4 pagineHEMOSTASIS AND COAGULATION PATHWAYSJemmy FandriNessuna valutazione finora
- Anticoagulation - An Overview Anaesthesia Tutorial of The Week 143 20 JULY 2009Documento9 pagineAnticoagulation - An Overview Anaesthesia Tutorial of The Week 143 20 JULY 2009Daniel MartinezNessuna valutazione finora
- Haemocompatibility of Blood Contacting Devices Repaired)Documento16 pagineHaemocompatibility of Blood Contacting Devices Repaired)Sinéad LyonsNessuna valutazione finora
- Bleeding Disdrdelrs: L. Roy Eversole, DDS, MSD, MADocumento7 pagineBleeding Disdrdelrs: L. Roy Eversole, DDS, MSD, MASurendra Reddy MunnangiNessuna valutazione finora
- Hematologic EmergenciesDocumento38 pagineHematologic EmergenciesKhaled JudehNessuna valutazione finora
- Anticoagulation - An Overview Anaesthesia Tutorial of The Week 143 20 JULY 2009Documento9 pagineAnticoagulation - An Overview Anaesthesia Tutorial of The Week 143 20 JULY 2009Echo WhyNessuna valutazione finora
- Overview of the coagulation systemDocumento9 pagineOverview of the coagulation systemaksinuNessuna valutazione finora
- Pharmacology Review Drugs That Alter Blood Coagulation PDFDocumento6 paginePharmacology Review Drugs That Alter Blood Coagulation PDFyouyayuNessuna valutazione finora
- Chapter 146excessive Bleeding and BruisingDocumento7 pagineChapter 146excessive Bleeding and BruisinghgpNessuna valutazione finora
- University of Mosul College of Medicine Department of Obstetrics and Gynecological 2019/2020Documento6 pagineUniversity of Mosul College of Medicine Department of Obstetrics and Gynecological 2019/2020سيرين عمار عبدالرحمنNessuna valutazione finora
- Secondary HemostasisDocumento9 pagineSecondary HemostasisMedicah Simon PeligrinoNessuna valutazione finora
- Hemostasis Basics Programmed Learner: TopicDocumento19 pagineHemostasis Basics Programmed Learner: TopicAahsan Iqbal احسن اقبالNessuna valutazione finora
- Hematologic Principles SGD PDFDocumento5 pagineHematologic Principles SGD PDFJolaine ValloNessuna valutazione finora
- HP SeminarDocumento10 pagineHP Seminarishrathjalal1999Nessuna valutazione finora
- Centralnervoussystem Complicationsof Hemorrhagicandcoagulation DisordersDocumento21 pagineCentralnervoussystem Complicationsof Hemorrhagicandcoagulation DisordersAdrian KhomanNessuna valutazione finora
- Anatomy and Physiological AssignmentDocumento23 pagineAnatomy and Physiological Assignmentbill chaiwaNessuna valutazione finora
- Admin, 32551Documento14 pagineAdmin, 32551Buthaina HusseinNessuna valutazione finora
- Disseminated Intravascular Coagulopathy Disseminated Intravascular Coagulation (DIC) Is A PathologicalDocumento6 pagineDisseminated Intravascular Coagulopathy Disseminated Intravascular Coagulation (DIC) Is A PathologicalValarmathiNessuna valutazione finora
- Bleeding DisordersDocumento27 pagineBleeding DisordersIliana América AlarcónNessuna valutazione finora
- Control Pelvic Bleeding SurgeryDocumento44 pagineControl Pelvic Bleeding SurgeryKasamapon Oak ChawanachitNessuna valutazione finora
- Chap 4 Blood HemoDocumento23 pagineChap 4 Blood HemoDianne GalangNessuna valutazione finora
- Hemostatic Complications of Solid OrganDocumento18 pagineHemostatic Complications of Solid OrganWael AlkhiaryNessuna valutazione finora
- Blood Coagulation and HaemostasisDocumento76 pagineBlood Coagulation and HaemostasisArun MamachanNessuna valutazione finora
- Bleeding DisordersDocumento10 pagineBleeding Disorderslyli Star AngeloNessuna valutazione finora
- A Cell-Based Model of Coagulation and The Role of Factor VIIa - Blood Review 2003Documento5 pagineA Cell-Based Model of Coagulation and The Role of Factor VIIa - Blood Review 2003Oscar Echeverría OrellanaNessuna valutazione finora
- SEED No 1 - COAG - Principles of HaemostasisDocumento4 pagineSEED No 1 - COAG - Principles of HaemostasisM Yusuf Ali RNessuna valutazione finora
- Basic Principles of Platelet Biology and Clinical ImplicationsDocumento11 pagineBasic Principles of Platelet Biology and Clinical ImplicationsIsmael Rivera DiazNessuna valutazione finora
- Literature AbdoDocumento20 pagineLiterature AbdothestaffforpediatricptNessuna valutazione finora
- Key Terms: Chapter 19: Coagulation DisordersDocumento16 pagineKey Terms: Chapter 19: Coagulation DisordersDarryl Betts100% (1)
- Blood Coagulation: Hemostasis and Thrombin RegulationDocumento14 pagineBlood Coagulation: Hemostasis and Thrombin RegulationQariahMaulidiahAminNessuna valutazione finora
- Basic HemostasisDocumento4 pagineBasic HemostasisMarvin SimbulanNessuna valutazione finora
- Labmed33 0948Documento6 pagineLabmed33 0948VKTNNessuna valutazione finora
- Bleeding Disorders1Documento81 pagineBleeding Disorders1DrMuskan AroraNessuna valutazione finora
- Coagulation and Bleeding Disorders: Review and Update: Douglas A. TriplettDocumento10 pagineCoagulation and Bleeding Disorders: Review and Update: Douglas A. TriplettSherlockHolmesSezNessuna valutazione finora
- Disorders of Hemostasis Associated in Chronic Kidney DiseaseDocumento7 pagineDisorders of Hemostasis Associated in Chronic Kidney DiseaseSandi AuliaNessuna valutazione finora
- Thrombosis Embolism InfarctionDocumento64 pagineThrombosis Embolism InfarctionDontoNessuna valutazione finora
- Anemia Evaluation and Transfusion GuidelinesDocumento4 pagineAnemia Evaluation and Transfusion GuidelinesGisselle PauloNessuna valutazione finora
- Jurnal PendarahanDocumento15 pagineJurnal Pendarahanイアン リムホト ザナガNessuna valutazione finora
- Fourth Stage HemostasisDocumento9 pagineFourth Stage HemostasisAli MONessuna valutazione finora
- Jurnal Gangguan TrombositDocumento13 pagineJurnal Gangguan TrombositkaynabilNessuna valutazione finora
- Chapter 4 Hemostasis, Surgical Bleeding, and Transfusion 35Documento13 pagineChapter 4 Hemostasis, Surgical Bleeding, and Transfusion 35Vladimir OstriaNessuna valutazione finora
- Antiplatelet Therapy Role in AtherothrombosisDocumento11 pagineAntiplatelet Therapy Role in Atherothrombosishiran.reisNessuna valutazione finora
- App'ch To The BLEEDING CHILDDocumento30 pagineApp'ch To The BLEEDING CHILDduoltut11Nessuna valutazione finora
- Cascadeeee KoagulasiDocumento3 pagineCascadeeee Koagulasiv noviantihyNessuna valutazione finora
- Dis IcDocumento11 pagineDis IcyeandunNessuna valutazione finora
- CoagulationDocumento3 pagineCoagulationHerho-nyl CesNessuna valutazione finora
- Hemostasis and Blood CoagulationDocumento11 pagineHemostasis and Blood CoagulationRinta MoonNessuna valutazione finora
- Chapter 1 Overview of IsDocumento35 pagineChapter 1 Overview of IsNathalie PortugalNessuna valutazione finora
- Pathology Associated With Third MolarsDocumento10 paginePathology Associated With Third Molarsapi-265532519Nessuna valutazione finora
- Cocero Anticoagulantes Orales Directos y Comorbilidades Marzo 2019Documento8 pagineCocero Anticoagulantes Orales Directos y Comorbilidades Marzo 2019api-265532519Nessuna valutazione finora
- Dodson Asymtomatic Disease Free Wisdom TeethDocumento8 pagineDodson Asymtomatic Disease Free Wisdom Teethapi-265532519Nessuna valutazione finora
- Pototski Dental Management of PX Receiving Anticoag Antiplatelet TX 2007Documento6 paginePototski Dental Management of PX Receiving Anticoag Antiplatelet TX 2007api-265532519Nessuna valutazione finora
- Medical Management of Patient Undergoing Dentoalveolar SDocumento8 pagineMedical Management of Patient Undergoing Dentoalveolar Sapi-265532519Nessuna valutazione finora
- Wound Healing and Perioperative Care - Vol 18 Issue 1 Feb 2006 OmfsDocumento7 pagineWound Healing and Perioperative Care - Vol 18 Issue 1 Feb 2006 Omfsapi-265532519Nessuna valutazione finora
- Internal Derangements of TMD - Vol 20 Issue 2 May 2008Documento10 pagineInternal Derangements of TMD - Vol 20 Issue 2 May 2008api-265532519Nessuna valutazione finora
- Pototski Dental Management of PX Receiving Anticoag Antiplatelet TX 2007Documento6 paginePototski Dental Management of PX Receiving Anticoag Antiplatelet TX 2007api-265532519Nessuna valutazione finora
- Laskin The Use of Prophylactic AntibioticsDocumento6 pagineLaskin The Use of Prophylactic Antibioticsapi-265532519Nessuna valutazione finora
- Patel Et Al-2014-Oral Surgery OpioidsDocumento7 paginePatel Et Al-2014-Oral Surgery Opioidsapi-265532519Nessuna valutazione finora
- Bailey Et Al-2014-Oral Surgery NsaidsDocumento10 pagineBailey Et Al-2014-Oral Surgery Nsaidsapi-265532519Nessuna valutazione finora
- Dental Trauma Guidelines III Primary Teeth - Flores Anderson AndreassenDocumento7 pagineDental Trauma Guidelines III Primary Teeth - Flores Anderson Andreassenapi-265532519Nessuna valutazione finora
- Coulthard Et Al-2014-Oral Surgery ParecetamolDocumento6 pagineCoulthard Et Al-2014-Oral Surgery Parecetamolapi-265532519Nessuna valutazione finora
- Impacted Canine and First MolarsDocumento10 pagineImpacted Canine and First Molarsapi-265532519Nessuna valutazione finora
- Medication Related Osteonecrosis of The JawDocumento26 pagineMedication Related Osteonecrosis of The Jawapi-265532519100% (1)
- Tooth Extraction in The Presence of Acute InfectionDocumento5 pagineTooth Extraction in The Presence of Acute Infectionapi-265532519Nessuna valutazione finora
- Cardiovascular Response To EpinephrineDocumento7 pagineCardiovascular Response To Epinephrineapi-265532519Nessuna valutazione finora
- Parameters of Care Dentoalveolar Surgery 2012Documento22 pagineParameters of Care Dentoalveolar Surgery 2012api-265532519Nessuna valutazione finora
- Coagulation DisordersDocumento26 pagineCoagulation DisordersLia pramita0% (1)
- Lighting the Way with Diagnostics Analyser InnovationsDocumento8 pagineLighting the Way with Diagnostics Analyser InnovationsOo Kenx OoNessuna valutazione finora
- Suspected Adverse Reactions To COVID 19 Vaccination and Safety of SoHODocumento11 pagineSuspected Adverse Reactions To COVID 19 Vaccination and Safety of SoHOVevveNessuna valutazione finora
- Adult Transfusion GuidelinesDocumento18 pagineAdult Transfusion GuidelinesConnor ScanlonNessuna valutazione finora
- Blood Transfusion & ComponentsDocumento56 pagineBlood Transfusion & Componentsadithya polavarapuNessuna valutazione finora
- Blood Functions: Presented by Dr. Khaled Ezam PHD PhysiologyDocumento34 pagineBlood Functions: Presented by Dr. Khaled Ezam PHD PhysiologyShrouk EldakroryNessuna valutazione finora
- BT 633-Human Biology & Diseases: Blood Patho-PhysiologyDocumento11 pagineBT 633-Human Biology & Diseases: Blood Patho-PhysiologySriMounicaKalidasuNessuna valutazione finora
- CASE REPORT COMPETITION With Identifying FeaturesDocumento12 pagineCASE REPORT COMPETITION With Identifying FeaturesJoel Cesar AtinadoNessuna valutazione finora
- Circulatory System: Heart, Blood Vessels & Their FunctionsDocumento17 pagineCirculatory System: Heart, Blood Vessels & Their FunctionskangaanushkaNessuna valutazione finora
- Naga College Foundation, Inc.: Case Study On AnemiaDocumento66 pagineNaga College Foundation, Inc.: Case Study On AnemiaAnnie Lou AbrahamNessuna valutazione finora
- Huether: Understanding Pathophysiology, 6th EditionDocumento4 pagineHuether: Understanding Pathophysiology, 6th EditionTecsh DeckgirlNessuna valutazione finora
- COVID-19 Hypercoagulability Mechanisms ReviewDocumento13 pagineCOVID-19 Hypercoagulability Mechanisms ReviewMartha OktaviaNessuna valutazione finora
- Literature Review On Blood GroupDocumento7 pagineLiterature Review On Blood Groupaebvqfzmi100% (1)
- Hema 2 - Prelim Topic 3 - Platelet Disorders and Laboratory TestsDocumento8 pagineHema 2 - Prelim Topic 3 - Platelet Disorders and Laboratory TestsLowenstein JenzenNessuna valutazione finora
- The Human Digestive System: A Concise Overview of its Key Components and FunctionsDocumento257 pagineThe Human Digestive System: A Concise Overview of its Key Components and FunctionsAyushNessuna valutazione finora
- Lab, Drug, NCPDocumento19 pagineLab, Drug, NCPRhodora LozanoNessuna valutazione finora
- A Case Report On Glanzmann's ThrombastheniaDocumento4 pagineA Case Report On Glanzmann's ThrombastheniaBaru Chandrasekhar RaoNessuna valutazione finora
- Leukemias: Care SettingDocumento11 pagineLeukemias: Care SettingTinNessuna valutazione finora
- 10 0000@th Schattauer de@generic-18AB3E84DCB5Documento12 pagine10 0000@th Schattauer de@generic-18AB3E84DCB5Ricardo GomezNessuna valutazione finora
- MLS 306 Blood Bank Anticoagulants and Preservatives: AKINBO D.B. Lecture SeriesDocumento27 pagineMLS 306 Blood Bank Anticoagulants and Preservatives: AKINBO D.B. Lecture SeriesFredNessuna valutazione finora
- Human Biology Concepts and Current Issues 8th Edition Johnson Test Bank DownloadDocumento31 pagineHuman Biology Concepts and Current Issues 8th Edition Johnson Test Bank DownloadJustin Hunter100% (35)
- "Sticky Bone" Use in Implant Dentistry: Zirconia Full Arch Implant RestorationDocumento64 pagine"Sticky Bone" Use in Implant Dentistry: Zirconia Full Arch Implant RestorationJuan David Torres CanoNessuna valutazione finora
- SURGERY A: SYSTEMIC INFLAMMATORY RESPONSEDocumento4 pagineSURGERY A: SYSTEMIC INFLAMMATORY RESPONSEAisha Al JenaibiNessuna valutazione finora