Potrebbero piacerti anche
- Powerpoint: Colorectal Polyps and Colorectal CarcinomaDocumento68 paginePowerpoint: Colorectal Polyps and Colorectal Carcinomaj.doe.hex_87100% (5)
- Powerpoint: Anal and Perianal DisordersDocumento66 paginePowerpoint: Anal and Perianal Disordersj.doe.hex_8780% (5)
- Anatomy of OesophagusDocumento25 pagineAnatomy of OesophagusRabi SyedNessuna valutazione finora
- CT of Colorectal CancerDocumento35 pagineCT of Colorectal CancerNader ElSayedNessuna valutazione finora
- Hepatic Surgical AnatomyDocumento23 pagineHepatic Surgical Anatomyyacine26Nessuna valutazione finora
- Vascular Diseases (1 of 3)Documento4 pagineVascular Diseases (1 of 3)Doctor GeneralNessuna valutazione finora
- Powerpoint: Liver Surgical DiseasesDocumento95 paginePowerpoint: Liver Surgical Diseasesj.doe.hex_8792% (12)
- Lung CancerDocumento19 pagineLung Cancerj.doe.hex_87Nessuna valutazione finora
- SURGERY 2018-2008 Regular+Supplementary Chapter Wise Question Papers WBUHSDocumento16 pagineSURGERY 2018-2008 Regular+Supplementary Chapter Wise Question Papers WBUHSBcBaba 007100% (1)
- CP Intestinal Obstruction PathoPhysiologyDocumento4 pagineCP Intestinal Obstruction PathoPhysiologyKatherine 'Chingboo' Leonico LaudNessuna valutazione finora
- Mylo Anal StenosisDocumento8 pagineMylo Anal StenosisCarmen DiazNessuna valutazione finora
- Colorectal Screening AlgorithmDocumento12 pagineColorectal Screening Algorithmsavvy_as_98Nessuna valutazione finora
- Anorectal AnatomyDocumento14 pagineAnorectal Anatomypologro100% (5)
- Colorectal CaDocumento55 pagineColorectal CasuperjaxxxonNessuna valutazione finora
- Anorectal Abscess: Principles of Internal Medicine, 18E. New York, Ny: Mcgraw-Hill 2012Documento7 pagineAnorectal Abscess: Principles of Internal Medicine, 18E. New York, Ny: Mcgraw-Hill 2012Irene SohNessuna valutazione finora
- Diagnosis Problem of DefecationDocumento36 pagineDiagnosis Problem of DefecationMico Ga Bisa Gendut100% (1)
- Diseases of The Anus Rev#1CDocumento77 pagineDiseases of The Anus Rev#1C2012Nessuna valutazione finora
- Anorectal Surgery PDFDocumento33 pagineAnorectal Surgery PDFLuminitaDumitriuNessuna valutazione finora
- Powerpoint: Chronic Inflammatory DisordesDocumento55 paginePowerpoint: Chronic Inflammatory Disordesj.doe.hex_87Nessuna valutazione finora
- Running A Colorectal Surgery ServiceDocumento21 pagineRunning A Colorectal Surgery ServicebloodsphereNessuna valutazione finora
- Semiology of The IntestineDocumento37 pagineSemiology of The Intestinebear dianaNessuna valutazione finora
- Operative Surgery Manual (2003) (UnitedVRG)Documento221 pagineOperative Surgery Manual (2003) (UnitedVRG)andreea_paraschivNessuna valutazione finora
- Colorectal Cancer: Dr. Gil VillanuevaDocumento41 pagineColorectal Cancer: Dr. Gil VillanuevaNick GaralagaNessuna valutazione finora
- Fascial Spaces in The HandDocumento20 pagineFascial Spaces in The Handveegeer80% (5)
- Anorectal Anatomy & Surgical ManagementDocumento164 pagineAnorectal Anatomy & Surgical Managementsgod34Nessuna valutazione finora
- Surgical Disease of Spleen Part 2Documento52 pagineSurgical Disease of Spleen Part 2Rashed ShatnawiNessuna valutazione finora
- Wilms TumorDocumento11 pagineWilms TumorChichi Basar67% (3)
- HemangiomaDocumento15 pagineHemangiomaGrace Febryanti Toding0% (1)
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocumento28 pagineOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNessuna valutazione finora
- Acute PancreatitisDocumento46 pagineAcute PancreatitisLew NianNessuna valutazione finora
- Anal CanalDocumento129 pagineAnal CanalPalanki GopalNessuna valutazione finora
- BreastDocumento49 pagineBreastcryphonexyNessuna valutazione finora
- Billiary SystemDocumento60 pagineBilliary SystemDONALD UNASHENessuna valutazione finora
- The Rectum & Anal CanalDocumento28 pagineThe Rectum & Anal Canalapi-19916399Nessuna valutazione finora
- Colorectal CA CME-CVLDocumento32 pagineColorectal CA CME-CVLAbu ZidaneNessuna valutazione finora
- Congenital Cystic Masses of The NeckDocumento48 pagineCongenital Cystic Masses of The NeckEsraa El ShemeNessuna valutazione finora
- Erb's PointDocumento14 pagineErb's PointRohit SharmaNessuna valutazione finora
- Sinus, FistulaDocumento46 pagineSinus, Fistulaalia0% (1)
- Dr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliDocumento25 pagineDr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliKarem Maali100% (1)
- General Surgery SMALL INTESTINES-Dr MendozaDocumento101 pagineGeneral Surgery SMALL INTESTINES-Dr MendozaMedisina101Nessuna valutazione finora
- Cholesteatoma PDFDocumento28 pagineCholesteatoma PDFazadutNessuna valutazione finora
- Skin and Subcutaneous TissueDocumento138 pagineSkin and Subcutaneous TissueNirav CHOVATIYANessuna valutazione finora
- Foley Catheter CareDocumento6 pagineFoley Catheter Carefreddie27Nessuna valutazione finora
- Anal ProblemsDocumento35 pagineAnal ProblemsSandip VaghelaNessuna valutazione finora
- Development of MesentryDocumento28 pagineDevelopment of MesentryimmmiNessuna valutazione finora
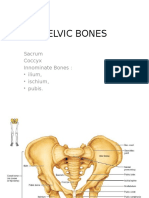
- Pelvic BoneDocumento15 paginePelvic BoneYoanneveline TanakNessuna valutazione finora
- Surgery of PancreasDocumento30 pagineSurgery of PancreasmackieccNessuna valutazione finora
- Excision of Branchial Cleft CystsDocumento10 pagineExcision of Branchial Cleft Cystssjs315Nessuna valutazione finora
- Neoplastic Thyroid Disease - Thyroid Nodules Goiter and Thyroid CancerDocumento57 pagineNeoplastic Thyroid Disease - Thyroid Nodules Goiter and Thyroid CancerNavya SreeNessuna valutazione finora
- Tracheobronchial Tree (TBT) : by DR HottorDocumento33 pagineTracheobronchial Tree (TBT) : by DR HottorChris ZantiraNessuna valutazione finora
- Laparoscopic Repair of Inguinal HerniaDocumento12 pagineLaparoscopic Repair of Inguinal Herniawadhe omara100% (1)
- The Pathophysiology of CholesteatomaDocumento17 pagineThe Pathophysiology of Cholesteatomaapi-19500641Nessuna valutazione finora
- Vascular Anomalies: Mehtab Ahmed Plastic Surgery LNHDocumento62 pagineVascular Anomalies: Mehtab Ahmed Plastic Surgery LNHZeeshan Ali BawaNessuna valutazione finora
- CA OesophagusDocumento47 pagineCA OesophagusAnsif KNessuna valutazione finora
- Imaging in Vascular SurgeryDocumento33 pagineImaging in Vascular Surgerydrzalie70100% (1)
- 7.30.08 Volk. Mesenteric IschemiaDocumento16 pagine7.30.08 Volk. Mesenteric Ischemiaowcordal7297Nessuna valutazione finora
- Curs Pelvis PerineuDocumento101 pagineCurs Pelvis PerineuCiprianTeodorulNessuna valutazione finora
- Peptic Ulcers: DR Yotham Phiri Mmed (Surg)Documento46 paginePeptic Ulcers: DR Yotham Phiri Mmed (Surg)Emmanuel MukukaNessuna valutazione finora
- Surgery Illustrated - Surgical Atlas: Laparoscopic Transvesical DiverticulectomyDocumento13 pagineSurgery Illustrated - Surgical Atlas: Laparoscopic Transvesical DiverticulectomyIrma Suriani DarwisNessuna valutazione finora
- Compartment SynDocumento51 pagineCompartment SynFIYINFOLUWA ESTHER AYODELENessuna valutazione finora
- Carcinoma of The OesophagusDocumento15 pagineCarcinoma of The OesophagussharlvinieNessuna valutazione finora
- Pancreatic Cancer, Cystic Neoplasms and Endocrine Tumors: Diagnosis and ManagementDa EverandPancreatic Cancer, Cystic Neoplasms and Endocrine Tumors: Diagnosis and ManagementNessuna valutazione finora
- Scrotoscopic SurgeryDa EverandScrotoscopic SurgeryJinrui YangNessuna valutazione finora
- Lecture2c MdsyndromesDocumento2 pagineLecture2c Mdsyndromesj.doe.hex_87Nessuna valutazione finora
- Nutrition in InfantDocumento7 pagineNutrition in Infantj.doe.hex_87Nessuna valutazione finora
- Namaz - The Health BenefitsDocumento130 pagineNamaz - The Health Benefitsj.doe.hex_87100% (1)
- Aplastic Anemia, 2008Documento10 pagineAplastic Anemia, 2008j.doe.hex_87Nessuna valutazione finora
- Understanding The 12 - Lead ECG, Part IIDocumento11 pagineUnderstanding The 12 - Lead ECG, Part IIj.doe.hex_87Nessuna valutazione finora
- Svaritm 2010Documento26 pagineSvaritm 2010j.doe.hex_87Nessuna valutazione finora
- Atherosclerosis. Biochemical Modifications in Acute Coronary SyndromeDocumento12 pagineAtherosclerosis. Biochemical Modifications in Acute Coronary Syndromej.doe.hex_87Nessuna valutazione finora
- The Liver: Methods of ExaminationDocumento49 pagineThe Liver: Methods of Examinationj.doe.hex_87Nessuna valutazione finora
- Aplast AnDocumento9 pagineAplast Anj.doe.hex_87Nessuna valutazione finora
- Methods of ExaminationDocumento56 pagineMethods of Examinationj.doe.hex_87Nessuna valutazione finora
- Cardiac Imaging TechniquesDocumento86 pagineCardiac Imaging Techniquesj.doe.hex_87Nessuna valutazione finora
- Studies Suggest That Myocarditis Is A: Important Causes of MyocarditisDocumento11 pagineStudies Suggest That Myocarditis Is A: Important Causes of MyocarditisCristina Georgiana CoticăNessuna valutazione finora
- Understanding The 12 - Lead ECG, Part 1Documento9 pagineUnderstanding The 12 - Lead ECG, Part 1j.doe.hex_87Nessuna valutazione finora
- Hydatid Disease: or Iceberg SignDocumento53 pagineHydatid Disease: or Iceberg Signj.doe.hex_87Nessuna valutazione finora
- Water and Electrolytes DisturbancesDocumento63 pagineWater and Electrolytes Disturbancesj.doe.hex_87Nessuna valutazione finora
- Lionte Cor Pulmonale2010Documento11 pagineLionte Cor Pulmonale2010j.doe.hex_87Nessuna valutazione finora
- Radiology - Imaging of The ThoraxDocumento49 pagineRadiology - Imaging of The Thoraxj.doe.hex_87Nessuna valutazione finora
- Radiology - Imaging of The ThoraxDocumento49 pagineRadiology - Imaging of The Thoraxj.doe.hex_87Nessuna valutazione finora
- Powerpoint: Chronic Inflammatory DisordesDocumento55 paginePowerpoint: Chronic Inflammatory Disordesj.doe.hex_87Nessuna valutazione finora
- Lecture 1 Chest TraumaDocumento19 pagineLecture 1 Chest Traumaj.doe.hex_870% (1)
- Endocrinology Pharmacology: Hormone Agonists, Antagonists & ModulatorsDocumento151 pagineEndocrinology Pharmacology: Hormone Agonists, Antagonists & Modulatorsj.doe.hex_87100% (1)
- Powerpoint: Gall Stone Disease and Related DisordersDocumento70 paginePowerpoint: Gall Stone Disease and Related Disordersj.doe.hex_8767% (3)
- Peds1114 Neonatal VomitingDocumento24 paginePeds1114 Neonatal VomitingABDILLAHNessuna valutazione finora
- Lecture Notes On GastroenterologyDocumento6 pagineLecture Notes On GastroenterologyGyanendra KcNessuna valutazione finora
- Small Bowel Obstruction - Clinical Diagnosis and TreatmentDocumento11 pagineSmall Bowel Obstruction - Clinical Diagnosis and TreatmentVigariooNessuna valutazione finora
- 2 Intestinal Obstruction. IntussusceptionDocumento28 pagine2 Intestinal Obstruction. IntussusceptionGede SubhagaNessuna valutazione finora
- Intestinal ObstructionDocumento157 pagineIntestinal ObstructionOmar SuleimanNessuna valutazione finora
- Pediatric Surgery Dr. A. IgamaDocumento6 paginePediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNessuna valutazione finora
- Contents - 2023 - Veterinary Clinics of North America Equine PracticeDocumento4 pagineContents - 2023 - Veterinary Clinics of North America Equine PracticediazsunshineNessuna valutazione finora
- 2.large Bowel ObstructionDocumento13 pagine2.large Bowel Obstructionurmila prajapatiNessuna valutazione finora
- Intestinal Obstruction PDFDocumento7 pagineIntestinal Obstruction PDFmist73Nessuna valutazione finora
- Ileus Obstruksi - Anggi Eka ForendaDocumento12 pagineIleus Obstruksi - Anggi Eka ForendaNadya ZahraNessuna valutazione finora
- Disturbances in Absorption and EliminationDocumento120 pagineDisturbances in Absorption and EliminationBeBs jai SelasorNessuna valutazione finora
- RX Protocol by DR - Anwarul Azim PDFDocumento120 pagineRX Protocol by DR - Anwarul Azim PDFGB Majumder100% (1)
- Guia de Bologna-2013Documento14 pagineGuia de Bologna-2013andreigustvNessuna valutazione finora
- Intestinal Malrotation and Volvulus: Luisa Ferrero, François Becmeur, and Olivier ReinbergDocumento15 pagineIntestinal Malrotation and Volvulus: Luisa Ferrero, François Becmeur, and Olivier ReinbergIván Castellares RojasNessuna valutazione finora
- Imaging in Acute Intestinal Obstruction 2019Documento8 pagineImaging in Acute Intestinal Obstruction 2019oktaviaNessuna valutazione finora
- Ebook Comprehensive Radiographic Pathology 6Th Edition Eisenberg Test Bank Full Chapter PDFDocumento46 pagineEbook Comprehensive Radiographic Pathology 6Th Edition Eisenberg Test Bank Full Chapter PDFsinapateprear4k100% (11)
- Anatomi Radiologi Foto Polos AbdomenDocumento64 pagineAnatomi Radiologi Foto Polos AbdomenDesy Nurul AzizahNessuna valutazione finora
- 03 - Neonatal Intestinal ObstructionDocumento28 pagine03 - Neonatal Intestinal Obstructionmahmoud khaledNessuna valutazione finora
- Imaging of Small Bowel and ColonDocumento69 pagineImaging of Small Bowel and ColonURo Kku100% (1)
- Surgery Pretest SummaryDocumento9 pagineSurgery Pretest SummaryPrince DuNessuna valutazione finora
- 2021 Article 2922Documento4 pagine2021 Article 2922AnirisulNessuna valutazione finora
- Gastric VolvulusDocumento6 pagineGastric VolvulusIosif SzantoNessuna valutazione finora
- An Approach To Paediatric Abdominal PainDocumento32 pagineAn Approach To Paediatric Abdominal PaindrsaleemNessuna valutazione finora
- Abdominal EmergenciesDocumento126 pagineAbdominal EmergencieskityamuwesiNessuna valutazione finora
- Approach To Plain AbdomenDocumento69 pagineApproach To Plain AbdomenKong Kong KongNessuna valutazione finora
- 7-Neonatal Surgical EmergenciesDocumento29 pagine7-Neonatal Surgical EmergenciesResti Rangga SusiloNessuna valutazione finora
- Health Cards G.O.176 PDFDocumento90 pagineHealth Cards G.O.176 PDFGowri ShankarNessuna valutazione finora
- Last Hour Review 2020 by Mci Gurukul DR Bhuoendra Armaan Chourasiya PDFDocumento49 pagineLast Hour Review 2020 by Mci Gurukul DR Bhuoendra Armaan Chourasiya PDFadiNessuna valutazione finora