Potrebbero piacerti anche
- 2018 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesDa Everand2018 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesValutazione: 4.5 su 5 stelle4.5/5 (2)
- Chicago Review Press NCLEX-PN Practice Test and ReviewDa EverandChicago Review Press NCLEX-PN Practice Test and ReviewValutazione: 4 su 5 stelle4/5 (4)
- Nursing Fluids and ElectrolytesDocumento14 pagineNursing Fluids and Electrolytesaga1028100% (18)
- 2020 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesDa Everand2020 NCLEX-PN Test Prep. Questions and Answers with Explanations: Study Guide to Pass the License Exam Effortlessly - Exam Review for Practical NursesValutazione: 1 su 5 stelle1/5 (1)
- Fluid and Electrolytes for Nursing StudentsDa EverandFluid and Electrolytes for Nursing StudentsValutazione: 5 su 5 stelle5/5 (12)
- FUNDAMENTALS OF NURSING: Passbooks Study GuideDa EverandFUNDAMENTALS OF NURSING: Passbooks Study GuideValutazione: 5 su 5 stelle5/5 (1)
- A Handbook for Student Nurses, 201617 edition: Introducing key issues relevant for practiceDa EverandA Handbook for Student Nurses, 201617 edition: Introducing key issues relevant for practiceValutazione: 4 su 5 stelle4/5 (1)
- FOUNDATIONS OF NURSING: Passbooks Study GuideDa EverandFOUNDATIONS OF NURSING: Passbooks Study GuideNessuna valutazione finora
- 140 Must Know Meds Demolish Nursing PharmacologyDa Everand140 Must Know Meds Demolish Nursing PharmacologyValutazione: 4 su 5 stelle4/5 (18)
- Medical Surgical Nursing Review NotesDocumento75 pagineMedical Surgical Nursing Review Notesstuffednurse92% (146)
- Nursing management The Ultimate Step-By-Step GuideDa EverandNursing management The Ultimate Step-By-Step GuideNessuna valutazione finora
- PSYCHIATRIC AND MENTAL HEALTH NURSE: Passbooks Study GuideDa EverandPSYCHIATRIC AND MENTAL HEALTH NURSE: Passbooks Study GuideNessuna valutazione finora
- Dimensional Analysis For Nursing StudentsDa EverandDimensional Analysis For Nursing StudentsNessuna valutazione finora
- Unit 8 Med Surg Study Guide NursingDocumento5 pagineUnit 8 Med Surg Study Guide Nursingatl_nurse_student100% (7)
- Schaum's Outline of Critical Care Nursing: 250 Review QuestionsDa EverandSchaum's Outline of Critical Care Nursing: 250 Review QuestionsValutazione: 5 su 5 stelle5/5 (1)
- MEDICAL SURGICAL NURSING: Passbooks Study GuideDa EverandMEDICAL SURGICAL NURSING: Passbooks Study GuideNessuna valutazione finora
- Nursing Study Guide: Your Nursing Assistant To Do Well In SchoolDa EverandNursing Study Guide: Your Nursing Assistant To Do Well In SchoolValutazione: 3 su 5 stelle3/5 (2)
- A Simplified Guide to Nursing Mnemonics (2022 Edition)Da EverandA Simplified Guide to Nursing Mnemonics (2022 Edition)Nessuna valutazione finora
- Medical Surgical Nursing Cardio Vascular System ClassDocumento15 pagineMedical Surgical Nursing Cardio Vascular System Classvallal100% (2)
- Medical Surgical Nursing PinoyDocumento67 pagineMedical Surgical Nursing Pinoyalfred31191% (23)
- The Basics: A Comprehensive Outline of Nursing School ContentDa EverandThe Basics: A Comprehensive Outline of Nursing School ContentValutazione: 5 su 5 stelle5/5 (3)
- Medical Surgical NursingDocumento10 pagineMedical Surgical NursingFreeNursingNotes50% (16)
- Fundamentals of NursingDocumento16 pagineFundamentals of NursingFreeNursingNotes85% (26)
- Schaum's Outline of Emergency Nursing: 242 Review QuestionsDa EverandSchaum's Outline of Emergency Nursing: 242 Review QuestionsValutazione: 4.5 su 5 stelle4.5/5 (3)
- Nursing Care Plans: Nursing Diagnosis and Assessment, Nursing Interventions GuideDa EverandNursing Care Plans: Nursing Diagnosis and Assessment, Nursing Interventions GuideValutazione: 5 su 5 stelle5/5 (4)
- Nursing Fundamentals DeMYSTiFieD, Second EditionDa EverandNursing Fundamentals DeMYSTiFieD, Second EditionValutazione: 2 su 5 stelle2/5 (2)
- The Chicago Review Press NCLEX-RN Practice Test and ReviewDa EverandThe Chicago Review Press NCLEX-RN Practice Test and ReviewValutazione: 4 su 5 stelle4/5 (20)
- Easy Nursing Notes For The Registered Nurse.Da EverandEasy Nursing Notes For The Registered Nurse.Valutazione: 4 su 5 stelle4/5 (6)
- Anatomy of a Super Nurse: The Ultimate Guide to Becoming NurseyDa EverandAnatomy of a Super Nurse: The Ultimate Guide to Becoming NurseyValutazione: 5 su 5 stelle5/5 (3)
- Psychiatric-Mental Health Nursing: Scope and Standards of PracticeDa EverandPsychiatric-Mental Health Nursing: Scope and Standards of PracticeValutazione: 4.5 su 5 stelle4.5/5 (6)
- Psychiatric and Mental Health Nursing DemystifiedDa EverandPsychiatric and Mental Health Nursing DemystifiedValutazione: 5 su 5 stelle5/5 (1)
- 150 Tips and Tricks for New Nurses: Balance a hectic schedule and get the sleep you need…Avoid illness and stay positive…Continue your education and keep up with medical advancesDa Everand150 Tips and Tricks for New Nurses: Balance a hectic schedule and get the sleep you need…Avoid illness and stay positive…Continue your education and keep up with medical advancesValutazione: 3 su 5 stelle3/5 (6)
- Exam Facts NCLEX PN Nursing Study GuideDa EverandExam Facts NCLEX PN Nursing Study GuideValutazione: 3.5 su 5 stelle3.5/5 (6)
- The Everything New Nurse Book, 2nd Edition: Gain confidence, manage your schedule, and be ready for anything!Da EverandThe Everything New Nurse Book, 2nd Edition: Gain confidence, manage your schedule, and be ready for anything!Valutazione: 5 su 5 stelle5/5 (1)
- Medical-Surgical Nursing Demystified, Second EditionDa EverandMedical-Surgical Nursing Demystified, Second EditionNessuna valutazione finora
- Neurologic NursingDocumento14 pagineNeurologic Nursingtheglobalnursing100% (6)
- A Guide for the Nurse Entrepreneur: Make a DifferenceDa EverandA Guide for the Nurse Entrepreneur: Make a DifferenceNessuna valutazione finora
- Nursing Mnemonics: The Ultimate Tips and Notes For NursesDa EverandNursing Mnemonics: The Ultimate Tips and Notes For NursesValutazione: 5 su 5 stelle5/5 (1)
- Maternal-Newborn Nursing DeMYSTiFieD: A Self-Teaching GuideDa EverandMaternal-Newborn Nursing DeMYSTiFieD: A Self-Teaching GuideNessuna valutazione finora
- Obstetrical NursingDocumento36 pagineObstetrical NursingFreeNursingNotes100% (7)
- Lewiss Medical Surgical Nursing 5th Australian Brown Test BankDocumento8 pagineLewiss Medical Surgical Nursing 5th Australian Brown Test Banksonyaaaq50% (2)
- Nursing: Scope and Standards of PracticeDa EverandNursing: Scope and Standards of PracticeValutazione: 5 su 5 stelle5/5 (2)
- Medical Surgical Nursing QuizDocumento9 pagineMedical Surgical Nursing Quizapi-3718174100% (27)
- Nursing Laboratory and Diagnostic Tests Demystified, Second EditionDa EverandNursing Laboratory and Diagnostic Tests Demystified, Second EditionNessuna valutazione finora
- NATIONAL COUNCIL LICENSURE EXAMINATION FOR REGISTERED NURSES (NCLEX-RN): Passbooks Study GuideDa EverandNATIONAL COUNCIL LICENSURE EXAMINATION FOR REGISTERED NURSES (NCLEX-RN): Passbooks Study GuideNessuna valutazione finora
- Fundamentals of NursingDocumento18 pagineFundamentals of NursingFreeNursingNotes78% (9)
- 101 Ways to Score Higher on your NCLEX: What You Need to Know About the National Council Licensure Examination Explained SimplyDa Everand101 Ways to Score Higher on your NCLEX: What You Need to Know About the National Council Licensure Examination Explained SimplyValutazione: 3.5 su 5 stelle3.5/5 (10)
- Pedia NotesDocumento7 paginePedia NotesFreeNursingNotes100% (1)
- Research NotesDocumento24 pagineResearch NotesFreeNursingNotes100% (1)
- Pneumonia Causative Agent: 1. Infectious - Bacteria (Streptococcus Pneumonia) Virus FungiDocumento2 paginePneumonia Causative Agent: 1. Infectious - Bacteria (Streptococcus Pneumonia) Virus FungiFreeNursingNotes100% (1)
- Pruritus PRURITIS Pruritis (Itching) Is One of The Most CommonDocumento2 paginePruritus PRURITIS Pruritis (Itching) Is One of The Most CommonFreeNursingNotesNessuna valutazione finora
- PERTUSSIS / Whooping Cough PERTUSSIS Causative Agent: Bordetella Pertussis ModeDocumento1 paginaPERTUSSIS / Whooping Cough PERTUSSIS Causative Agent: Bordetella Pertussis ModeFreeNursingNotesNessuna valutazione finora
- RABIES Causative Agent: Rhabdovirus Mode of Transmission: Bite of RabidDocumento1 paginaRABIES Causative Agent: Rhabdovirus Mode of Transmission: Bite of RabidFreeNursingNotes100% (1)
- Integumentary Communicable DiseasesDocumento4 pagineIntegumentary Communicable DiseasesFreeNursingNotesNessuna valutazione finora
- Musculoskeletal NotesDocumento4 pagineMusculoskeletal NotesFreeNursingNotes100% (1)
- Pedia Note1Documento38 paginePedia Note1FreeNursingNotes100% (1)
- MS InstrumentsDocumento3 pagineMS InstrumentsFreeNursingNotesNessuna valutazione finora
- Musculoskeletal Note1Documento34 pagineMusculoskeletal Note1FreeNursingNotes100% (4)
- Psychiatric Nursing NotesDocumento2 paginePsychiatric Nursing NotesFreeNursingNotes0% (1)
- NERVOUS SYSTEM Communicable Diseases LEPROSYDocumento3 pagineNERVOUS SYSTEM Communicable Diseases LEPROSYFreeNursingNotesNessuna valutazione finora
- Meningococcal / Meningitis Meningococcal/Meningitis Causative Agent: 1. Bacteria:Meningcoccus, Neisseria MeningitidesDocumento1 paginaMeningococcal / Meningitis Meningococcal/Meningitis Causative Agent: 1. Bacteria:Meningcoccus, Neisseria MeningitidesFreeNursingNotes100% (1)
- Appendicitis Nursing NotesDocumento2 pagineAppendicitis Nursing NotesFreeNursingNotes33% (3)
- Epididymitis Epididymitis Is An Infection of The Epididymis That UsuallyDocumento1 paginaEpididymitis Epididymitis Is An Infection of The Epididymis That UsuallyFreeNursingNotesNessuna valutazione finora
- Gastrointestinal Communicable DiseasesDocumento7 pagineGastrointestinal Communicable DiseasesFreeNursingNotes100% (1)
- Blood Disorders AnemiaDocumento6 pagineBlood Disorders AnemiaFreeNursingNotesNessuna valutazione finora
- CATARACT A Cataract Is An Opacity of The Eye's NormallyDocumento2 pagineCATARACT A Cataract Is An Opacity of The Eye's NormallyFreeNursingNotesNessuna valutazione finora
- Diptheria Causative Agent: Corynabacterium Diphtheriae (Klebs - Loeffler Bacilli) ModeDocumento1 paginaDiptheria Causative Agent: Corynabacterium Diphtheriae (Klebs - Loeffler Bacilli) ModeFreeNursingNotes100% (1)
- Renal NursingDocumento11 pagineRenal NursingFreeNursingNotes100% (10)
- Mental Health Is Defined AsDocumento34 pagineMental Health Is Defined AsFreeNursingNotes100% (2)
- Psychiatric NursingDocumento21 paginePsychiatric NursingFreeNursingNotes92% (38)
- Disorders of Urinary System Urinary CalculiDocumento5 pagineDisorders of Urinary System Urinary CalculiFreeNursingNotes100% (3)
- Bell's PalsyDocumento2 pagineBell's PalsyFreeNursingNotes100% (1)
- Prof Ad QuestionsDocumento8 pagineProf Ad QuestionsAdzwereh JambolawanNessuna valutazione finora
- Professional AdjustmentDocumento7 pagineProfessional AdjustmentFreeNursingNotes100% (1)
- Prof AdDocumento23 pagineProf AdFreeNursingNotes100% (2)
- Nursing JurisprudenceDocumento9 pagineNursing JurisprudenceFreeNursingNotes100% (3)
- Name: Date: 1. Laws Which Are Known To Be AuthoredDocumento12 pagineName: Date: 1. Laws Which Are Known To Be AuthoredFreeNursingNotesNessuna valutazione finora
- Oncological Emergencies From Pathophysiology and Diagnosis To Treatment: A Narrative ReviewDocumento22 pagineOncological Emergencies From Pathophysiology and Diagnosis To Treatment: A Narrative ReviewDeni IrwandiNessuna valutazione finora
- HyponatremiaDocumento19 pagineHyponatremiaapi-260357356Nessuna valutazione finora
- MEdical Surgical REVEWERDocumento86 pagineMEdical Surgical REVEWERennaedNessuna valutazione finora
- Pharma PrelimDocumento8 paginePharma PrelimNom NomNessuna valutazione finora
- Hyponatremia 2015Documento19 pagineHyponatremia 2015gastonsaloNessuna valutazione finora
- Table of Endocrine Glands and Secreted HormonesDocumento10 pagineTable of Endocrine Glands and Secreted HormonesQamarul SyahirNessuna valutazione finora
- 1013 1558 1 SMDocumento10 pagine1013 1558 1 SMHaniyyahNessuna valutazione finora
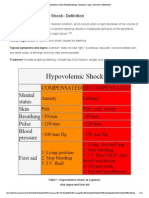
- Hypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarDocumento15 pagineHypovolemic Shock Pathophysiology, Symptoms, Signs, Treatment - EHealthStarKaloy KamaoNessuna valutazione finora
- 0 Pharmacology - Presentation.by - SIDRADocumento29 pagine0 Pharmacology - Presentation.by - SIDRASidra AlamNessuna valutazione finora
- Pharmacology TestDocumento88 paginePharmacology TestIrinotecanNessuna valutazione finora
- NCLEX Fluids & ElectrolytesDocumento6 pagineNCLEX Fluids & ElectrolytesNathalee Walker100% (1)
- Hiponatremia PDFDocumento11 pagineHiponatremia PDFNessa RojasNessuna valutazione finora
- Chapter 6 - Body Fluids, Water-Salt Balance RP1 PDFDocumento77 pagineChapter 6 - Body Fluids, Water-Salt Balance RP1 PDFpizzaNessuna valutazione finora
- Critical Care Notes Clinical Pocket Guide - (Hematology Oncology)Documento17 pagineCritical Care Notes Clinical Pocket Guide - (Hematology Oncology)Britanny NelsonNessuna valutazione finora
- Anph111 FinalsDocumento50 pagineAnph111 FinalsxeanNessuna valutazione finora
- IJGPDocumento10 pagineIJGPAndoni GogeascoecheaNessuna valutazione finora
- ICU Masterclass - Inotropes and Vasopressors HandbookDocumento79 pagineICU Masterclass - Inotropes and Vasopressors HandbookRj PolvorosaNessuna valutazione finora
- 1Documento28 pagine1Ed Daniel Tanseco DavisNessuna valutazione finora
- Homeostasis, Stress and Adaptation - Ppt2aDocumento154 pagineHomeostasis, Stress and Adaptation - Ppt2aV_RN100% (2)
- Icu Masterclass - Inotropes and Vasopressors: Christopher R. Tainter, MDDocumento78 pagineIcu Masterclass - Inotropes and Vasopressors: Christopher R. Tainter, MDHhaNessuna valutazione finora
- HypothalamusDocumento5 pagineHypothalamusBoneGrissleNessuna valutazione finora
- Pathophysiology of Diabetes Insipidus: DX: Serum ADHDocumento3 paginePathophysiology of Diabetes Insipidus: DX: Serum ADHkristian markus delos santosNessuna valutazione finora
- Pnle Medical Surgical ReviewDocumento17 paginePnle Medical Surgical ReviewKyla Rose ToledoNessuna valutazione finora
- Electrolytes and Related AbnormalitiesDocumento8 pagineElectrolytes and Related AbnormalitiesKyla CastilloNessuna valutazione finora
- The Neuroendocrinology of Love 14-02-17 PDFDocumento6 pagineThe Neuroendocrinology of Love 14-02-17 PDFKevin LagunaNessuna valutazione finora
- Best Practice in ShockDocumento30 pagineBest Practice in ShockFoungZanz D. LuffyzNessuna valutazione finora
- Question Paper Unit A161 02 Modules b1 b2 b3 Higher TierDocumento16 pagineQuestion Paper Unit A161 02 Modules b1 b2 b3 Higher TierAnonymous QFkCS837bNessuna valutazione finora
- Easy To ReadDocumento73 pagineEasy To Readdaljit chahalNessuna valutazione finora
- Electrolytes PDFDocumento5 pagineElectrolytes PDFFrances FranciscoNessuna valutazione finora
- Sample Book: Vasodilator DrugsDocumento4 pagineSample Book: Vasodilator DrugsManangioma ManNessuna valutazione finora