Potrebbero piacerti anche
- Authorization For Medical Treatment, Anesthesia and Performance of OperationDocumento3 pagineAuthorization For Medical Treatment, Anesthesia and Performance of OperationNatasha SNessuna valutazione finora
- Informed Consent To Surgery: 1. Title of FormDocumento4 pagineInformed Consent To Surgery: 1. Title of FormChandran OchathevarNessuna valutazione finora
- Invoice: Bill To: Advance Medical IncDocumento6 pagineInvoice: Bill To: Advance Medical IncChrisNance100% (2)
- Credential IngDocumento13 pagineCredential Ingdr_rajatjainNessuna valutazione finora
- Taller #2Documento3 pagineTaller #2Luisa Fernanda AlegriaNessuna valutazione finora
- Darwin MosciskiDocumento4 pagineDarwin Mosciskirahul nNessuna valutazione finora
- UT Southwestern Surgical Consent Form TemplateDocumento2 pagineUT Southwestern Surgical Consent Form TemplateChristopherCookNessuna valutazione finora
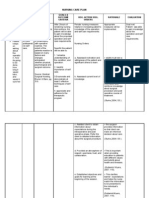
- NCP 1Documento4 pagineNCP 1Ke EjieNessuna valutazione finora
- PRE-1: Process For Obtaining Patient And/or Family Consent For Informed Decision Making About Their Care Are DocumentedDocumento20 paginePRE-1: Process For Obtaining Patient And/or Family Consent For Informed Decision Making About Their Care Are Documentedilyaskhosa032Nessuna valutazione finora
- Cross-Training: The Medical Assistant WorkbookDa EverandCross-Training: The Medical Assistant WorkbookNessuna valutazione finora
- Ambulatory Obstetrics GynecologyDocumento4 pagineAmbulatory Obstetrics GynecologyNelson R. PouNessuna valutazione finora
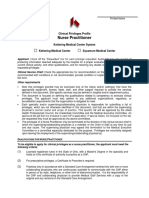
- AHP NursePractitionerDocumento14 pagineAHP NursePractitioneryogieNessuna valutazione finora
- Perioperative Nursing SkillsDocumento278 paginePerioperative Nursing SkillsNacel Celeste100% (3)
- Stelara SpecDocumento2 pagineStelara SpecPeter GiganteNessuna valutazione finora
- AAAASFI Surgical Standards ManualDocumento88 pagineAAAASFI Surgical Standards ManualAlexander Cespedes100% (1)
- General Practice - Fam Practice PrivilegesDocumento3 pagineGeneral Practice - Fam Practice PrivilegesRoos Beatrix WattimuryNessuna valutazione finora
- SBAR ExampleDocumento13 pagineSBAR Examplejugdeep15Nessuna valutazione finora
- Research Questionaire 1Documento3 pagineResearch Questionaire 1KARIZZA ABOLENCIANessuna valutazione finora
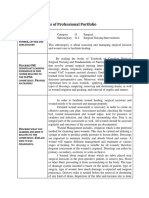
- NFDN 2003 Report On Progress of Professional PortfolioDocumento2 pagineNFDN 2003 Report On Progress of Professional Portfolioapi-304652587100% (2)
- Certified Nurse Midwife Delineation PrivilegesDocumento6 pagineCertified Nurse Midwife Delineation PrivilegesKesavan Anandha KumarNessuna valutazione finora
- Vision Claim Form 2016Documento1 paginaVision Claim Form 2016Shawna CashNessuna valutazione finora
- RN - Skills Check List.8.111Documento2 pagineRN - Skills Check List.8.111Nia Kaye100% (1)
- Priv Req Form 2011Documento5 paginePriv Req Form 2011Eko Wahyu AgustinNessuna valutazione finora
- Top 10 Most Read AORN Journal ArticlesDocumento107 pagineTop 10 Most Read AORN Journal ArticlesSandy Mapelli100% (1)
- Peace Corps MD and DO Privileging FormDocumento2 paginePeace Corps MD and DO Privileging FormAccessible Journal Media: Peace Corps Documents100% (2)
- CDC Test 3Documento7 pagineCDC Test 3Yucef Bahian-AbangNessuna valutazione finora
- Top 10 Most Read AORN Journal Articles PDFDocumento107 pagineTop 10 Most Read AORN Journal Articles PDFsriyanto ibsNessuna valutazione finora
- Proforma For Claiming Refund of Medical Expenses - 1 - Split - 2Documento2 pagineProforma For Claiming Refund of Medical Expenses - 1 - Split - 2ajayNessuna valutazione finora
- Sas 1 Cabahug, Victoria Mae IDocumento5 pagineSas 1 Cabahug, Victoria Mae Ibekbekk cabahugNessuna valutazione finora
- Resume For Cna JobDocumento7 pagineResume For Cna Jobgt72k5e5100% (1)
- Resume of Jasonmccormick69Documento2 pagineResume of Jasonmccormick69api-28896455Nessuna valutazione finora
- Surgery 1 - UCDocumento101 pagineSurgery 1 - UCEsvinch EsvinchNessuna valutazione finora
- Konsep Clinical PrivilegesDocumento5 pagineKonsep Clinical PrivilegesFebryan Cahya PermanaNessuna valutazione finora
- Citizen's Charter - VSU Hospital ServicesDocumento10 pagineCitizen's Charter - VSU Hospital ServicesvisayasstateuNessuna valutazione finora
- Thrombolytic Therapy For Acute Myocardial Infarction 01-30-13Documento1 paginaThrombolytic Therapy For Acute Myocardial Infarction 01-30-13Ushnish ChatterjeeNessuna valutazione finora
- Ppg-Gdch-Nur-43 Out On Pass PolicyDocumento5 paginePpg-Gdch-Nur-43 Out On Pass PolicyKenny Josef100% (1)
- Form of Essentiality Certificate B PDFDocumento2 pagineForm of Essentiality Certificate B PDFAnji KaringuNessuna valutazione finora
- Psychiatric Admission EvaluationDocumento5 paginePsychiatric Admission Evaluationfernlover3901Nessuna valutazione finora
- EBP ProjectDocumento14 pagineEBP ProjectCaroline KimNessuna valutazione finora
- Surgery Consent FormDocumento2 pagineSurgery Consent FormАлексей МалышкоNessuna valutazione finora
- HA WK4bDocumento26 pagineHA WK4bMARY ROSE FAJUTINANessuna valutazione finora
- MS Preoperative Part 2Documento5 pagineMS Preoperative Part 2Ano NymousNessuna valutazione finora
- Medical Fitness Declaration FormsDocumento2 pagineMedical Fitness Declaration FormsNoor SafwatNessuna valutazione finora
- Patient Identification SOPDocumento7 paginePatient Identification SOPIrma Nech100% (1)
- FACILITY NAME: - : I. Consent To Surgery or Special ProcedureDocumento11 pagineFACILITY NAME: - : I. Consent To Surgery or Special ProcedureJack Tedesco0% (1)
- Green Orange Blue Creative Healthcare Facility PresentationDocumento11 pagineGreen Orange Blue Creative Healthcare Facility PresentationhsqbhsyvmhNessuna valutazione finora
- Dialysis Nurse ResumeDocumento7 pagineDialysis Nurse Resumeaflkotkax100% (1)
- Credential and PrivilageDocumento125 pagineCredential and Privilagehatem newishyNessuna valutazione finora
- EBC EHAQ 4 Audit Tool Final January 2024Documento46 pagineEBC EHAQ 4 Audit Tool Final January 2024AberaNessuna valutazione finora
- Medical Assistant Duties For ResumeDocumento7 pagineMedical Assistant Duties For Resumef5dt39tp100% (2)
- Informed Consent For Laparoscopic CholecystectomyDocumento5 pagineInformed Consent For Laparoscopic CholecystectomyJatrik BiswasNessuna valutazione finora
- L Hi Appt Documents 02272023Documento9 pagineL Hi Appt Documents 02272023gelosmith3Nessuna valutazione finora
- Form For MedicalDocumento1 paginaForm For MedicalPamela Jane I. TornoNessuna valutazione finora
- Shouldice HospitalDocumento18 pagineShouldice HospitalAnonymous fky9Zn0JxNessuna valutazione finora
- Admitting A Client: Prepared By: Grace E. Guitguiten, R.N.,M.N. Clinical InstructorDocumento8 pagineAdmitting A Client: Prepared By: Grace E. Guitguiten, R.N.,M.N. Clinical InstructorGGie GetzNessuna valutazione finora
- Annexure - C Medical Reimbursement Claim Form For Outdoor TreatmentDocumento3 pagineAnnexure - C Medical Reimbursement Claim Form For Outdoor TreatmentPatiala BsnlNessuna valutazione finora
- Shouldice Hospital ReportDocumento9 pagineShouldice Hospital Reportakashmehta10Nessuna valutazione finora
- ASSISTING IN A MAJOR OPERATION Circulating Nurse Performance EvaluationDocumento2 pagineASSISTING IN A MAJOR OPERATION Circulating Nurse Performance EvaluationKrizzia Angela BacotocNessuna valutazione finora
- Form1 2 PDFDocumento8 pagineForm1 2 PDFerpNessuna valutazione finora
- Marketing Implant Dentistry: Attract and Influence Patients to Accept Your Dental Implant Treatment PlanDa EverandMarketing Implant Dentistry: Attract and Influence Patients to Accept Your Dental Implant Treatment PlanNessuna valutazione finora
- Authorization To Treat Mechanical Ventilator: Resuscitation and The Proper Use of A Manual Resuscitation DeviceDocumento1 paginaAuthorization To Treat Mechanical Ventilator: Resuscitation and The Proper Use of A Manual Resuscitation DeviceAccreditation ConsultantNessuna valutazione finora
- 1003 - Informed ConsentDocumento5 pagine1003 - Informed ConsentAccreditation ConsultantNessuna valutazione finora
- 08 - Privileges - Orthopaedics SurgeryDocumento3 pagine08 - Privileges - Orthopaedics SurgeryAccreditation ConsultantNessuna valutazione finora
- 08 - Privileges - General SurgeryDocumento3 pagine08 - Privileges - General SurgeryAccreditation ConsultantNessuna valutazione finora
- 1000-Ca Retail License and ExempteesDocumento1 pagina1000-Ca Retail License and ExempteesAccreditation ConsultantNessuna valutazione finora
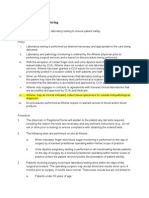
- 3 7 Laboratory MonitoringDocumento2 pagine3 7 Laboratory MonitoringAccreditation ConsultantNessuna valutazione finora
- 1 Senior Home Health Employee HandbookDocumento77 pagine1 Senior Home Health Employee HandbookAccreditation ConsultantNessuna valutazione finora
- Laser Plan & Policy 2011Documento14 pagineLaser Plan & Policy 2011Accreditation ConsultantNessuna valutazione finora
- Rights: THE of Our Patients, and TheirDocumento3 pagineRights: THE of Our Patients, and TheirAccreditation ConsultantNessuna valutazione finora